Moa of HTN in patient less than 55 years
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Here is a complete, well-sourced answer:
First-Line Treatment of HTN in Patients Under 55 Years: ACE Inhibitors (or ARBs)
Why Under 55?
Younger patients (<55 years) with hypertension tend to have high-renin, high-angiotensin II driven hypertension. Their blood pressure is primarily maintained through overactivation of the Renin-Angiotensin-Aldosterone System (RAAS). This makes RAAS-blocking drugs the most effective first-line choice.
In contrast, patients over 55 (and Black patients of any age) tend to have low-renin, volume-dependent hypertension, where calcium channel blockers (CCBs) or thiazide diuretics work better.
The RAAS Pathway (Why It Matters)
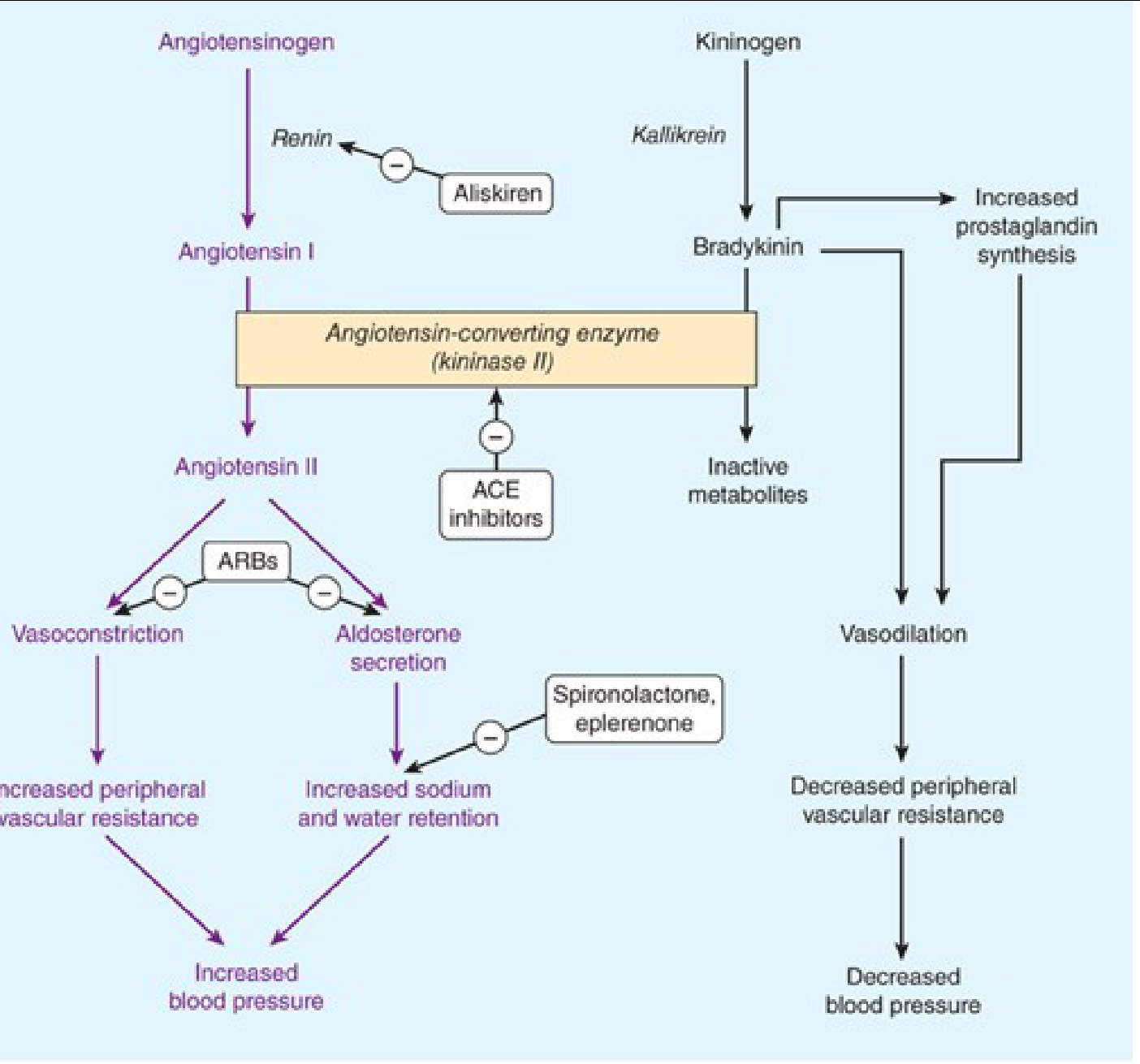
Sites of action of drugs that interfere with the renin-angiotensin-aldosterone system - Katzung's Basic & Clinical Pharmacology, 16e
The normal RAAS cascade:
- Renin (released by kidney in response to low renal perfusion pressure, sympathetic stimulation, or low distal Na⁺) cleaves angiotensinogen → Angiotensin I (inactive decapeptide)
- ACE (angiotensin-converting enzyme, also called kininase II), located on vascular endothelium, converts Angiotensin I → Angiotensin II (active octapeptide)
- Angiotensin II acts on AT₁ receptors to cause:
- Vasoconstriction → increased peripheral vascular resistance → raised BP
- Aldosterone secretion from adrenal cortex → Na⁺ and water retention → raised BP
- Angiotensin II/III also promote cardiac hypertrophy via trophic effects in tissue RAAS
Mechanism of ACE Inhibitors (Primary Drug Class)
ACE inhibitors (e.g., ramipril, enalapril, lisinopril) lower BP by two complementary mechanisms:
| Mechanism | Effect |
|---|---|
| Block ACE - prevent conversion of Ang I → Ang II | Reduces vasoconstriction and aldosterone secretion → decreases peripheral vascular resistance and Na⁺/H₂O retention |
| Inhibit bradykinin degradation - ACE normally breaks down bradykinin (a vasodilator) | Bradykinin accumulates → vasodilation → further BP reduction |
- Cardiac output and heart rate are not significantly changed
- No reflex sympathetic activation (unlike direct vasodilators) - safe in ischaemic heart disease
- Also reduce glomerular efferent arteriolar resistance → decrease intraglomerular pressure (renoprotective)
(Katzung's Basic and Clinical Pharmacology, 16e)
Mechanism of ARBs (Alternative/Equivalent First-Line)
ARBs (e.g., losartan, candesartan, valsartan) act one step downstream:
- Block AT₁ receptors directly, preventing Ang II from binding
- Same net effect: reduced vasoconstriction + reduced aldosterone secretion
- Do not inhibit bradykinin degradation, so they do not cause dry cough or angioedema
- Still teratogenic; may cause hyperkalemia
(Barash's Clinical Anesthesia, 9e)
Summary Table: Drug Choices by Age/Ethnicity
| Patient | First-Line Drug | Rationale |
|---|---|---|
| Under 55, non-Black | ACE inhibitor or ARB | High-renin RAAS-driven HTN |
| Over 55, or Black (any age) | CCB or thiazide diuretic | Low-renin, volume-dependent HTN |
| Diabetic/CKD with proteinuria | ACE-i or ARB (any age) | Proven renoprotection |
| Heart failure post-MI | ACE-i preferred | Proven mortality benefit |
Key Adverse Effects of ACE Inhibitors to Remember
- Dry cough (bradykinin accumulation) - switch to ARB if intolerable
- Angioedema (rare but serious - also bradykinin-mediated)
- Hyperkalemia (reduced aldosterone)
- First-dose hypotension (especially if volume-depleted)
- Acute kidney injury in bilateral renal artery stenosis
- Teratogenic - avoid in pregnancy
The combined use of any two RAAS inhibitors (ACE-i + ARB, or + direct renin inhibitor) should be avoided - it offers minimal extra BP reduction with high risk of renal impairment and hyperkalemia. (Goldman-Cecil Medicine, International Edition)
Why is there high renin raas driven HTN in young patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have excellent textbook content. Let me compile the complete answer.
Why Do Young Patients (<55 years) Have High-Renin, RAAS-Driven Hypertension?
This is actually a fascinating pathophysiology question, and the answer involves several converging mechanisms. The short answer: young patients tend to have neurogenic/adrenergic-dominant hypertension with high sympathetic tone driving renin release, whereas older patients accumulate salt sensitivity and vascular stiffening that shift the mechanism toward a volume/low-renin pattern.
1. High Sympathetic Nervous System (SNS) Activity in Youth
Young patients with essential hypertension characteristically show:
- Elevated heart rate
- Raised plasma catecholamines (norepinephrine)
- Increased directly measured sympathetic nerve discharge
The SNS acts on the kidney in two ways that directly drive renin:
- Beta-1 adrenoceptors on juxtaglomerular (JG) cells - sympathetic stimulation directly triggers renin secretion
- Alpha-adrenoceptors on tubular cells - increase tubular Na⁺ reabsorption, reducing Na⁺ delivery to the macula densa, which is a second signal for renin release
"In the kidneys, sympathetic nerves mediate renin release. Furthermore, innervation of each individual nephron affects sodium reabsorption." - Comprehensive Clinical Nephrology, 7e
2. The Three Stimuli for Renin Release (and why they are active in young patients)
Renin release from JG cells is triggered by three mechanisms, all of which can be exaggerated in young hypertensives:
| Stimulus | Mechanism | Why active in young |
|---|---|---|
| Low renal perfusion pressure | Baroreceptor in afferent arteriole senses stretch | Stress/sympathetic tone reduces effective renal perfusion |
| Sympathetic stimulation (beta-1) | Direct neural trigger on JG cells | SNS hyperactivity is prominent in younger patients |
| Low Na⁺ at macula densa | Tubuloglomerular feedback sensor | Sympathetic-driven Na⁺ reabsorption upstream reduces distal delivery |
"Renin release from the kidney cortex is stimulated by reduced renal arterial pressure, sympathetic neural stimulation, and reduced sodium delivery or increased sodium concentration at the distal renal tubule." - Katzung's Basic & Clinical Pharmacology, 16e
3. Why the Pattern SHIFTS With Age (>55 years)
As patients age, the pattern of hypertension changes from high-renin to low-renin for these reasons:
a) Arterial stiffening and reduced baroreflex sensitivity:
The carotid sinus and baroreflex-sensing sites become less distensible with age and atherosclerosis. The baroreflex becomes blunted - so it no longer effectively reduces sympathetic tone in response to high BP. Paradoxically, older hypertensives may have higher sympathetic activity than younger ones, but their kidneys respond differently.
b) Structural renal changes with age:
Glomerulosclerosis, hypertrophy of afferent arterioles, and fibrosis in the JG apparatus blunt renin secretion even when BP is high. This means the kidneys lose their ability to mount a renin response.
"Sclerotic and fibrotic changes in the glomeruli...combined with hypertrophy of the afferent arterioles, limit the sensing of BP in the juxtaglomerular apparatus...This blunts renin release." - National Kidney Foundation Primer, 8e
c) Salt sensitivity accumulates with age:
Older patients develop greater salt retention, expanding blood volume. High circulating volume suppresses renin via negative feedback (high Na⁺ delivery to macula densa inhibits JG cell secretion). So their HTN becomes volume/salt-driven rather than RAAS-driven.
d) Reduced nephron mass:
Age-related loss of nephrons reduces the number of JG cells available to produce renin.
4. The Renin Profile Spectrum in Essential HTN
About 20% of essential hypertension patients have high-renin (predominantly younger), 60% have normal-renin, and 20% have low-renin (predominantly older, Black patients, and salt-sensitive individuals):
| Profile | Age tendency | Mechanism | Best drug |
|---|---|---|---|
| High renin (~20%) | Younger (<55) | SNS-driven excess renin/Ang II | ACE-i / ARB |
| Normal renin (~60%) | Any age | Mixed | ACE-i/ARB + CCB/diuretic |
| Low renin (~20%) | Older, Black, obese | Volume/salt-driven, suppressed RAAS | CCB / Thiazide |
Summary: The Key Mechanism in Young Patients
High SNS activity (youth/stress)
↓
Beta-1 stimulation of JG cells
↓
↑ Renin → ↑ Ang I → ↑ Ang II
↓
Vasoconstriction + Aldosterone
↓
↑ Peripheral resistance + Na/H₂O retention
↓
HYPERTENSION (high-renin type)
This is why ACE inhibitors and ARBs - which block this very cascade - are so effective in patients under 55. They target the actual driver of hypertension in this age group, rather than simply addressing downstream consequences.
(Sources: Katzung's Basic & Clinical Pharmacology 16e; National Kidney Foundation Primer on Kidney Diseases 8e; Fuster & Hurst's The Heart 15e; Comprehensive Clinical Nephrology 7e)
This is a shared conversation. Sign in to Orris to start your own chat.