Antibiotic causes diarrhea and relation with pernicious anemia and its cuases
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Searching PubMed
antibiotic associated diarrhea Clostridioides difficile
Loading Image
I now have all the information needed for a thorough answer. Let me compile it.
Antibiotic-Associated Diarrhea, Pernicious Anemia, and Their Relationship
Part 1: Antibiotic-Associated Diarrhea (AAD)
Definition and Epidemiology
Antibiotic-associated diarrhea is otherwise unexplained diarrhea that occurs in association with the administration of antibiotics. It complicates up to 25% of antibiotic courses.
- Symptom to Diagnosis, 4th Ed.
Mechanisms of AAD
There are two main pathways:
1. Non-infectious (direct antibiotic effect)
- Disruption of intestinal flora: Normal colonic bacteria metabolize carbohydrates; antibiotics wipe these out, causing osmotic diarrhea from undigested carbohydrates in the colon.
- Promotility effects: Erythromycin acts as a motilin receptor agonist, speeding gut transit and causing diarrhea directly.
- Yamada's Textbook of Gastroenterology, 7th Ed.
2. Infectious (C. difficile)
- About 10-20% of diarrhea in the setting of antibiotic exposure is caused by Clostridioides difficile.
- Antibiotics disrupt normal colonic microbiota, allowing C. difficile overgrowth and toxin production.
- Symptom to Diagnosis, 4th Ed.
Antibiotics Most Commonly Responsible
| Highest Risk (C. difficile) | Common AAD (any mechanism) |
|---|---|
| Clindamycin | Clindamycin |
| Fluoroquinolones | Cephalosporins |
| 3rd/4th-gen cephalosporins | Ampicillin, amoxicillin, amoxicillin-clavulanate |
- Symptom to Diagnosis, 4th Ed.; Medical Microbiology 9e
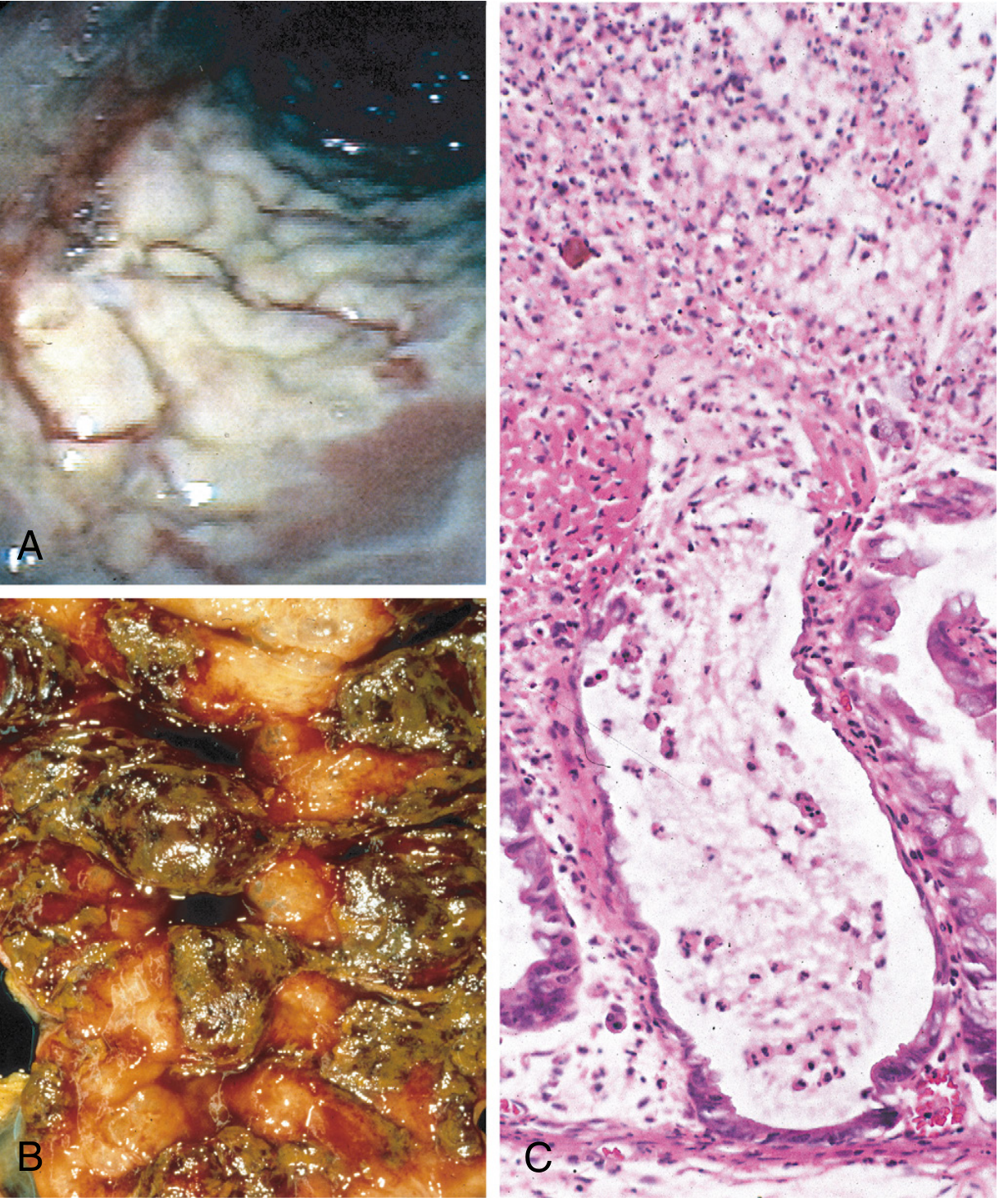
Pathogenesis of Pseudomembranous Colitis (Severe AAD)
C. difficile toxins (Toxin A and Toxin B) ribosylate small GTPases such as Rho, leading to:
- Disruption of the epithelial cytoskeleton
- Tight junction barrier loss
- Cytokine release and apoptosis
- Neutrophil dysfunction - forming the characteristic "volcano" mucopurulent exudates and white pseudomembranes on the colonic mucosa
Clinical Features and Treatment
- Symptoms: fever, leukocytosis, watery diarrhea, abdominal cramps
- Develops typically 5-10 days after antibiotic initiation
- Diagnosis: stool toxin detection (not culture)
- Treatment:
- Discontinue the offending antibiotic
- Metronidazole or vancomycin for severe disease
- Fecal microbiota transplant for recurrent disease
- Probiotics reduce risk and may shorten episodes
- Medical Microbiology 9e; Robbins Pathologic Basis of Disease
Part 2: Pernicious Anemia - Causes
Pernicious anemia is an autoimmune megaloblastic anemia caused by vitamin B12 (cobalamin) deficiency due to failure of intrinsic factor (IF) secretion.
Pathogenesis
The sequence is:
- Autoimmune destruction of gastric parietal cells (type A chronic atrophic gastritis)
- Loss of intrinsic factor secretion
- IF is required for B12 absorption in the terminal ileum
- Without IF, B12 cannot be absorbed → megaloblastic anemia + neurological damage
Two types of autoantibodies are involved:
-
Anti-parietal cell antibodies (in majority of cases)
-
Anti-intrinsic factor antibodies
-
Tietz Textbook of Laboratory Medicine, 7th Ed.; Dermatology 5e; Goldman-Cecil Medicine
Complete Causes of Vitamin B12 Deficiency (leading to pernicious-type picture)
A. Inadequate Dietary Intake
- Total vegetarianism (no eggs, milk, or animal products)
- Chronic alcoholism (rare)
B. Inadequate Absorption (most important)
- Pernicious anemia - autoimmune antibodies against parietal cells and/or IF
- Gastrectomy (total or partial) - loss of parietal cells removes IF source
- H2-receptor antagonists (e.g., ranitidine, cimetidine) - suppress both acid AND intrinsic factor production; long-term use can cause B12 deficiency
- Abnormal ileum - Crohn's disease, sprue, inflammatory bowel disease (ileum is where IF-B12 complex is absorbed)
- Bacterial overgrowth - gram-negative anaerobes in the small intestine can bind the B12-IF complex, preventing its absorption
- Parasitic infections - fish tapeworm (Diphyllobothrium latum) competes for B12
- Histology: A Text and Atlas; Rosen's Emergency Medicine; Goldman-Cecil Medicine
C. Inadequate Utilization
- Enzyme deficiency
- Abnormal B12-binding proteins
D. Increased Requirement / Increased Loss
-
Increased body metabolism demands more B12
-
Rosen's Emergency Medicine, Box 109.7
Part 3: The Connection Between Antibiotics and Pernicious Anemia
This is a subtle but real relationship operating through several mechanisms:
1. Bacterial Overgrowth and B12 Malabsorption
Normal gut flora in the small intestine can become pathologically overgrown. Gram-negative anaerobic bacteria compete for and bind the vitamin B12-intrinsic factor complex, preventing ileal absorption. Antibiotics treating bacterial overgrowth can actually improve B12 absorption in this scenario. However, inappropriate antibiotic use that disrupts normal flora can also paradoxically alter the gut microbiome in complex ways.
- Histology: A Text and Atlas (Folder 17.1)
2. H. pylori Eradication and Pernicious Anemia
Helicobacter pylori causes chronic gastritis that can progress to atrophic gastritis and pernicious anemia. Antibiotic eradication of H. pylori (triple/quadruple therapy) can halt progression and sometimes partially reverse atrophic gastritis, potentially preventing or improving pernicious anemia. H. pylori antigens mimic gastric epithelial antigens (molecular mimicry), triggering autoantibodies that damage parietal cells.
- Histology: A Text and Atlas (Folder 17.1)
3. Metformin and Long-term Antibiotics (indirect)
Some antibiotics alter the gut microbiome chronically, affecting absorption pathways for fat-soluble and B-complex vitamins.
Blood Smear in Megaloblastic (Pernicious) Anemia
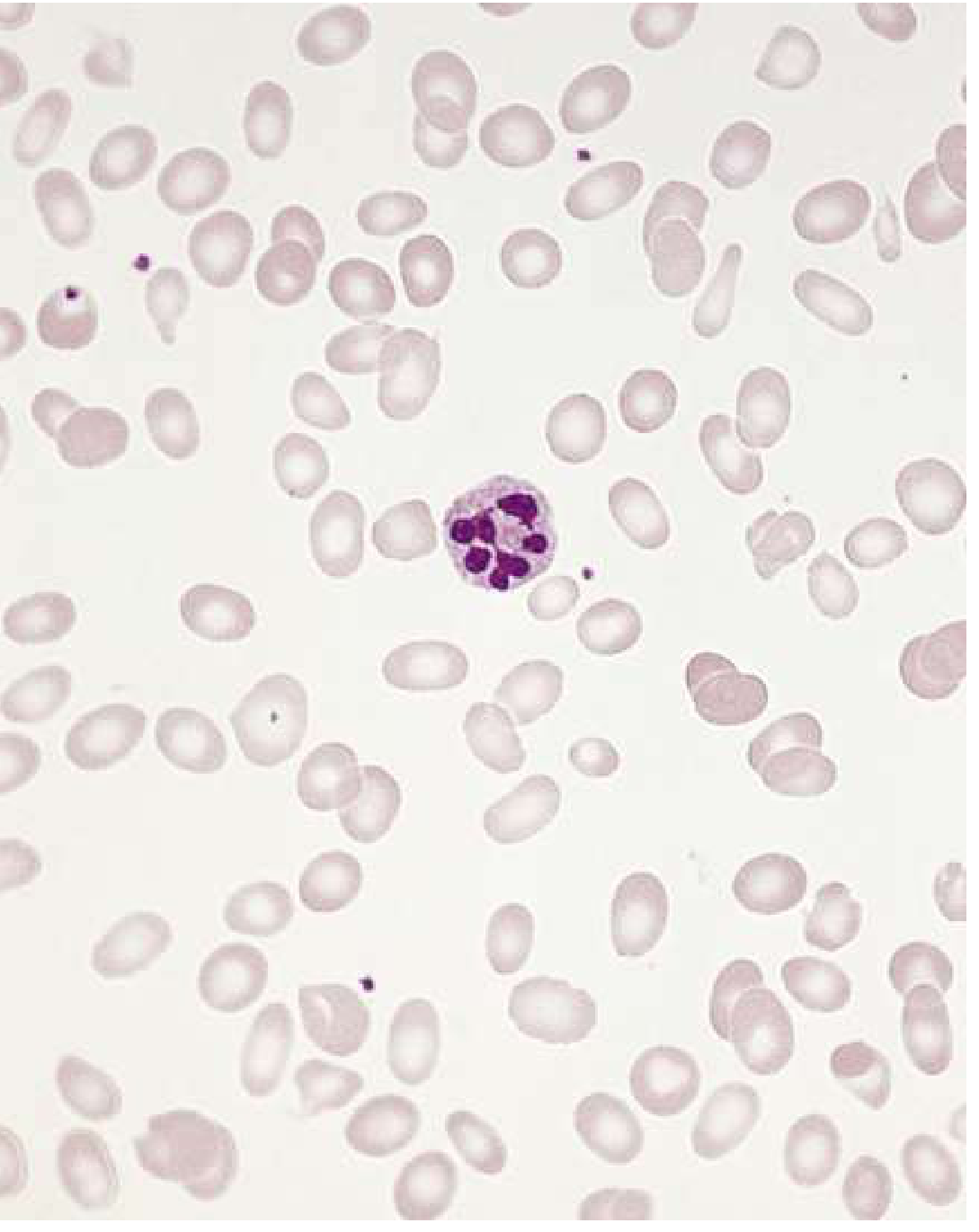
Key diagnostic findings:
- MCV > 100 fL (macrocytosis)
- Macro-ovalocytes and anisocytosis on smear
- Hypersegmented neutrophils (>5 lobes)
- Elevated serum LDH
- Low serum B12 (<200 μg/L)
- Elevated homocysteine and methylmalonic acid
Summary Table
| Feature | Antibiotic-Associated Diarrhea | Pernicious Anemia |
|---|---|---|
| Primary mechanism | Gut flora disruption / C. difficile toxins | Autoimmune loss of intrinsic factor |
| Key organisms/targets | C. difficile (Toxin A/B), normal flora | Gastric parietal cells, IF |
| Classic antibiotics | Clindamycin, fluoroquinolones, cephalosporins | H2-blockers worsen B12 absorption |
| Treatment | Stop antibiotic; vancomycin/metronidazole | Lifelong B12 replacement (IM or high-dose oral) |
| Connection | Antibiotics alter gut flora; H. pylori eradication antibiotics can prevent/improve pernicious anemia; bacterial overgrowth treated with antibiotics can restore B12 absorption | - |
Recent evidence note: A 2025 Cochrane systematic review (PMID 40931979) evaluated probiotics for prevention of C. difficile-associated diarrhea - confirming probiotic use alongside antibiotics is an evidence-based preventive strategy.
This is a shared conversation. Sign in to Orris to start your own chat.