I now have comprehensive information from multiple authoritative textbooks. Let me compile the full 15-mark MD exam answer.
---
# Inhalation Devices in COPD - Full Details (15 Marks Answer)
## Introduction
Inhaled therapy is the **cornerstone of pharmacological management** in COPD. It targets drug directly to the lungs, provides faster onset of action, allows lower drug doses, and reduces systemic adverse effects compared to oral therapy. Only 10-20% of an inhaled drug reaches the lungs - the remaining 80-90% is swallowed and enters systemic circulation via the GI tract and liver (first-pass effect).
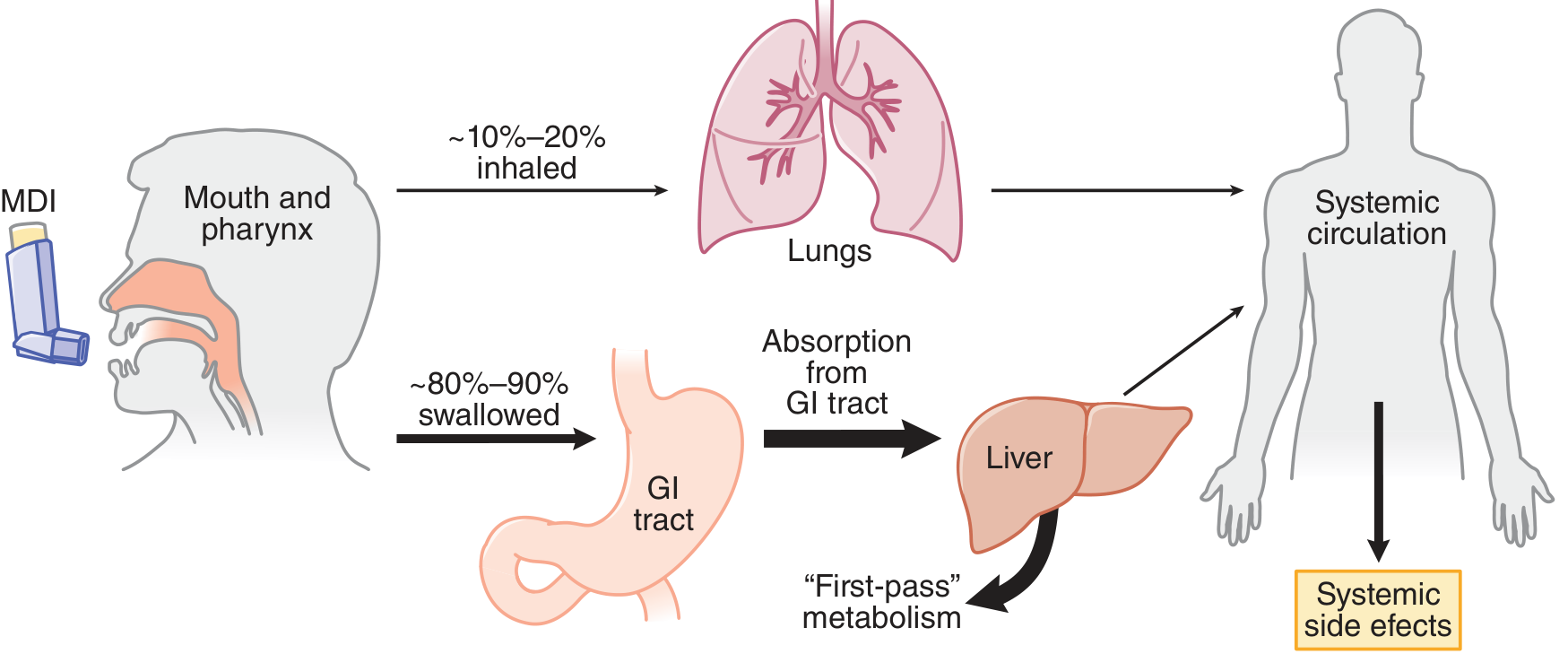
*Drug deposition after inhalation - Goodman & Gilman's Pharmacological Basis of Therapeutics*
---
## Classification of Inhalation Devices
| Device | Type |
|--------|------|
| 1. Pressurized Metered-Dose Inhaler (pMDI) | Propellant-driven |
| 2. Spacer / Valved Holding Chamber | pMDI add-on |
| 3. Dry Powder Inhaler (DPI) | Breath-actuated, propellant-free |
| 4. Nebulizer (Jet / Ultrasonic / Mesh) | Solution/suspension aerosolization |
| 5. Soft Mist Inhaler (SMI) | e.g., Respimat |
---
## 1. Pressurized Metered-Dose Inhaler (pMDI)
### Mechanism
- Drug is formulated as a **liquid suspension or solution** with a propellant inside a sealed pressurized canister.
- Older propellant: **Chlorofluorocarbons (CFC/Freon)** - now replaced by ozone-friendly **Hydrofluoroalkanes (HFA)** / Hydrofluorocarbons (HFC).
- On actuation, rapid vaporization of propellant aerosolizes the drug into fine particles.
- Typically delivers **50-200 doses** per canister.
### Particle Size and Lung Deposition
- Optimal particle size for lower airway deposition: **1-5 micrometers (MMAD)**
- HFA pMDIs deliver finer particles to smaller airways but also increase systemic absorption.
- With standard technique: only ~10-20% of the dose reaches the lungs.
### Correct Inhalation Technique (Critical for Exams)
1. Shake the inhaler
2. Exhale fully
3. Place mouthpiece in mouth and form a tight seal
4. **Actuate at the START of a deep, slow inhalation** lasting ~5 seconds
5. Hold breath for **at least 5 seconds** at end of inspiration
6. Wait 1 minute before second puff if needed
- Common errors: failure to inhale slowly and deeply; poor hand-mouth coordination (especially in elderly).
### Breath-Actuated pMDI
- Triggered by patient's inspiratory flow to overcome coordination problems.
- Examples: Autohaler, Easi-Breathe.
- However, studies show no advantage over correct conventional pMDI technique.
### Advantages
- Compact and portable
- Multidose (50-200 doses)
- Quick treatment time
- Drug in sealed canister (protected from humidity)
- Inexpensive
### Disadvantages
- High oropharyngeal deposition (up to 80-90% without spacer)
- Requires good hand-mouth coordination
- Propellants may cause "cold Freon" effect
- HFA propellants contribute to climate change (carbon footprint)
- Difficult to assess when canister is empty
---
## 2. Spacer Devices (Valved Holding Chambers)
### Mechanism
- A spacer is an add-on chamber placed **between the pMDI and the patient's mouth**.
- Reduces the high velocity of aerosol cloud.
- Allows evaporation of liquid propellant, producing **smaller drug particles** that deposit deeper in the lungs.
- **Traps large particles** on the plastic walls, reducing oropharyngeal impaction.
### Types of Spacers
| Type | Description |
|------|-------------|
| Valved holding chamber | Has a one-way inhalation valve - allows drug to be inhaled when patient is ready |
| Simple extension device | Non-valved; still requires reasonable coordination |
| Reverse-flow device | Aerosol actuated away from patient into a collapsible bag |
### Clinical Importance in COPD
- Reduces **oropharyngeal deposition of inhaled corticosteroids (ICS)** - thus reducing local side effects (oral candidiasis, dysphonia) and systemic absorption via GI tract.
- Useful in **elderly patients** and **children as young as 3 years** with face mask attachment.
- Particularly helpful in patients with poor coordination.
### Key Points for Correct Spacer Use
- **Prime** the spacer with the pMDI before use.
- Actuate **one puff at a time** - not multiple simultaneous doses (reduces electrostatic charge effect).
- Wash with **ionic detergent** and air dry to reduce electrostatic charge.
- Should be prescribed with **compatible pMDI only** - not interchangeable between devices.
- Antistatic spacers are available.
### Advantages
- Overcomes coordination problems
- Reduces oropharyngeal deposition
- Reduces local and systemic ICS side effects
- Useful for elderly, children, and acute exacerbations
### Disadvantages
- Bulky and less portable
- Electrostatic charge can reduce drug delivery
- Must be device-specific (not universally compatible)
---
## 3. Dry Powder Inhaler (DPI)
### Mechanism
- **Propellant-free** devices.
- Drug is present as **finely milled powder particles** either:
- Bound to larger **lactose carrier molecules**
- As loose powder aggregates
- **Breath-actuated**: patient's own inspiratory effort disperses and de-aggregates the drug from the carrier particle.
- Requires **minimum inspiratory flow rate** for adequate drug dispersion (usually >30-60 L/min).
### Classification of DPIs
| Type | Examples | Details |
|------|----------|---------|
| **Single-dose (unit-dose)** | Handihaler (tiotropium) | Drug loaded individually from gelatin capsules; capsule is punctured and drug inhaled |
| **Multi-unit-dose** | Accuhaler/Diskus | Drug sealed in individual foil blisters on a moving strip |
| **Multi-dose (reservoir)** | Turbuhaler, Genuair | Drug metered from a powder reservoir; requires priming |
### DPI Devices Used in COPD (Examples)
- **Turbuhaler** - Budesonide, formoterol
- **Accuhaler (Diskus)** - Salmeterol/fluticasone, tiotropium
- **Handihaler** - Tiotropium (single-capsule device)
- **Breezhaler** - Indacaterol, glycopyrronium
- **Genuair/Pressair** - Aclidinium
- **Ellipta** - Umeclidinium/vilanterol, fluticasone furoate
### Problems in COPD Patients
- Patients with **moderate-to-severe COPD** may not generate adequate inspiratory flows.
- Insufficient inspiratory effort is the **most common inhaler error** with DPIs - associated with worsening disease and increased exacerbation frequency.
- Children under 7 years cannot use DPIs effectively.
- **Humidity** can degrade the powder - must be stored in dry environment.
### Advantages
- Compact and portable
- Quick treatment time
- Breath-actuated - no hand-mouth coordination needed
- No propellant (no ozone/climate issue)
- Simple to use if adequate inspiratory flow can be generated
### Disadvantages
- Requires adequate inspiratory flow (problematic in severe COPD)
- High oropharyngeal deposition
- Humidity degrades the drug
- Patients may be intolerant to lactose carrier (rare)
- Not suitable for very young children or acutely ill patients with very poor inspiratory effort
---
## 4. Nebulizers
### Mechanism
- Drug is dissolved or suspended in liquid (saline-based) and **aerosolized into a fine mist** for tidal breathing inhalation.
- Does NOT require coordination or high inspiratory effort.
- Suitable for tidal breathing at rest.
- Can deliver **much higher drug doses** than pMDIs.
### Types of Nebulizers
#### A. Jet Nebulizer
- Uses **compressed gas (air or oxygen)** or an electrical compressor.
- High-velocity air directed through a **Venturi opening** across the liquid drug to produce aerosolized droplets.
- Most widely used type.
- Larger, noisier.
- Effective for both solutions and suspensions.
#### B. Ultrasonic Nebulizer
- Uses a **rapidly vibrating piezoelectric crystal** at high frequency to produce aerosol.
- Does NOT require a compressed gas source.
- Smaller and quieter than jet nebulizers.
- More expensive and less robust.
- **Less effective for nebulizing suspensions**.
#### C. Mesh Nebulizer (newer generation)
- Drug passes through a vibrating mesh with thousands of laser-drilled holes.
- More efficient drug delivery, less waste during exhalation.
- Better portability and consistency.
- Provides **feedback for compliance monitoring**.
- More expensive but cost-effective due to reduced drug waste.
### Clinical Use in COPD
- **Acute exacerbations of COPD** - most common use, especially in hospital.
- When airway obstruction is extreme (severe COPD, inability to use other devices).
- Patients who are very old, very young, or mentally incapacitated.
- Delivery of high-dose antibiotics (e.g., inhaled tobramycin in bronchiectasis/COPD overlap).
- Drugs that must be given at high doses.
### Factors Affecting Nebulizer Delivery
- Crying in children greatly reduces lung deposition.
- Shallow/rapid breathing reduces efficiency.
- Face mask must fit correctly to avoid drug deposition on the face and eyes.
- Significant variability in output between different nebulizer models.
### Advantages
- **Large doses** of drug can be delivered
- **Tidal breathing** - no coordination or inspiratory effort needed
- Suitable for all ages including very young, elderly, acutely ill
- Many drug solutions can be aerosolized
- No patient cooperation needed for technique
### Disadvantages
- **Bulky, cumbersome, and expensive**
- Wasted drug in nebulizer reservoir (significant loss during exhalation with conventional nebulizers)
- Variable aerosol output between models
- **Time consuming** (5-15 minutes per treatment)
- Requires power source
- Requires regular **cleaning and maintenance** (infection risk)
---
## 5. Soft Mist Inhaler (SMI) - e.g., Respimat
- Uses a spring-driven mechanical system to produce a **slow-moving fine aerosol mist** without propellant.
- More drug reaches the lungs (~50%) compared to pMDI (~10-20%).
- Slow aerosol velocity reduces oropharyngeal impaction.
- The combination of **albuterol + ipratropium** is available in SMI form.
- Useful in patients who struggle with pMDI coordination.
- Does not require strong inspiratory effort like DPIs.
---
## Comparison Table: Advantages and Disadvantages
| Device | Advantages | Disadvantages |
|--------|------------|---------------|
| **pMDI** | Compact, portable, multidose, inexpensive, sealed canister | Poor oropharyngeal deposition, needs coordination, propellant issues |
| **Spacer** | Reduces side effects, helps elderly/children, better lung deposition | Bulky, device-specific, electrostatic charge issues |
| **DPI** | Compact, breath-actuated, no propellant | Needs high inspiratory flow, humidity-sensitive, not for severe COPD |
| **Nebulizer** | High dose delivery, tidal breathing, universal | Bulky, slow, expensive, variable output, maintenance required |
| **SMI** | Higher lung deposition, slow mist, no propellant | More expensive, specific device |
---
## Factors Determining Choice of Inhaler in COPD
1. **Disease severity** - Severe COPD patients may not achieve adequate inspiratory flow for DPIs; nebulizers may be preferred.
2. **Patient ability** - Poor coordination favors DPIs, SMI, or spacer+pMDI; very old/young patients may need nebulizers.
3. **Setting** - Acute exacerbation: nebulizer preferred; stable outpatient: pMDI or DPI.
4. **Drug availability** - Not all drugs are available in all devices.
5. **Cost** - pMDI generally cheapest; mesh nebulizers most expensive.
6. **Compliance** - Same device type for all drugs improves compliance.
7. **Technique training** - Healthcare workers must assess and regularly review inhaler technique.
8. **Environmental considerations** - pMDI propellants (HFAs) contribute to climate change.
---
## Key Exam Points
- **DPIs are breath-actuated** - require adequate inspiratory flow; problematic in severe COPD.
- **pMDIs need hand-mouth coordination** - solved by spacers or breath-actuated pMDIs.
- **Nebulizers are gold standard in acute exacerbations** and extreme airway obstruction.
- **Spacers reduce ICS side effects** (oral candidiasis, dysphonia, systemic absorption).
- Studies show **pMDI, DPI, and SMI are equally effective as nebulizers** in stable COPD patients who use correct technique.
- GOLD guidelines emphasize periodic **reassessment of inhaler technique** - incorrect technique is universal and worsens outcomes.
- More than **250 device-drug combinations** exist; prescribers and patients are commonly confused.
- A newer generation of DPIs requires **lower inspiratory flows** or delivers drug independent of breathing maneuver.
---
*Sources: Fishman's Pulmonary Diseases and Disorders (5th ed.) - Inhaler Devices, p. 804-805; Goodman & Gilman's Pharmacological Basis of Therapeutics - Delivery Devices, p. 2351-2357; Murray & Nadel's Textbook of Respiratory Medicine - COPD Management, p. 1826-1828*