Prescription for hematuria without pain patient is not willing to admit
Reading File
Finding Sources
Searching PubMed
painless hematuria outpatient management evaluation
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information to give a thorough, structured answer. Let me compile it.
Painless Hematuria - Outpatient Management (Patient Refusing Admission)
Why This Is a Red Flag
Painless hematuria is a classic presentation of urological malignancy - specifically bladder cancer, which accounts for up to 25% of hematuria cases in adults. Key points:
- Painless gross hematuria is the presenting symptom in 85% of newly diagnosed bladder cancer patients
- The risk of malignancy with gross hematuria is ~20.4%; with microscopic hematuria ~2.6-5.2%
- Even a single episode of gross hematuria must be fully evaluated, even if subsequent urinalysis is negative
- Anticoagulation use does NOT exempt the patient from a full workup - it cannot be attributed to anticoagulants without investigation
"The most common cause of gross hematuria in a patient older than 50 years of age is bladder cancer." - Campbell-Walsh-Wein Urology
Outpatient Management Plan
Step 1 - Rule Out Pseudohematuria First
- Confirm with clean-catch midstream urinalysis with microscopy (dipstick alone is insufficient - specificity only 65%)
- Urine dipstick FALSE positives occur with: myoglobinuria, hemoglobinuria, medications (rifampicin, pyridium), beets
- True hematuria = ≥3 RBCs/hpf on microscopy
Step 2 - Urgent Investigations (All Outpatient)
| Investigation | Purpose |
|---|---|
| Urine microscopy + culture | Confirm hematuria, rule out UTI |
| Renal function (creatinine, BUN) | Assess for nephropathy |
| Urine protein/spot PCR ratio | Rule out glomerular cause |
| FBC, coagulation screen | Bleeding disorders |
| PSA (male, after counselling) | Prostate cancer (~10% of recurrent gross hematuria) |
| CT Urogram (CTU) | Upper tract malignancy, stones, RCC |
| Cystoscopy | Gold standard for bladder cancer - NO imaging replaces it |
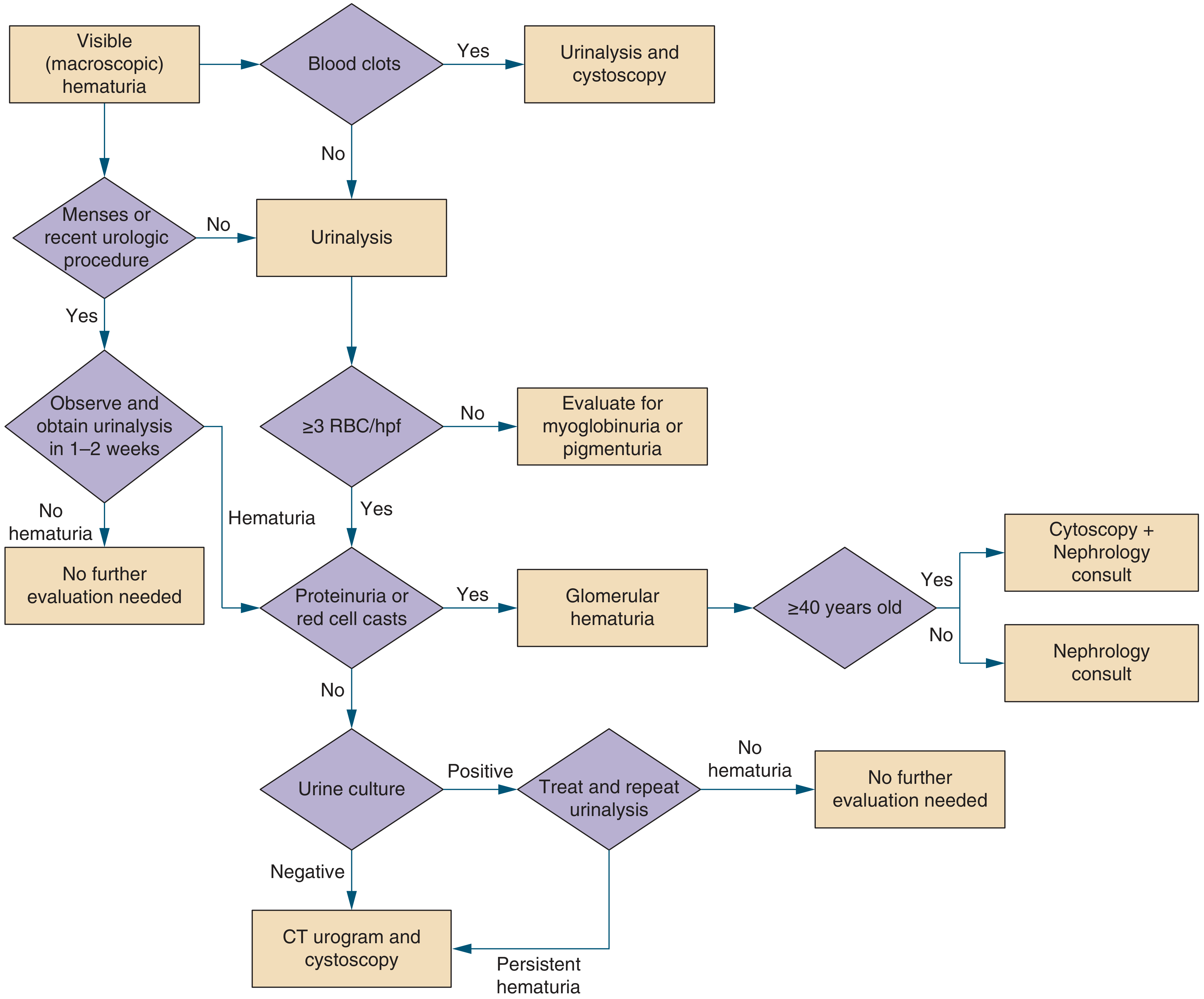
Step 3 - Based on Findings
Diagram from Symptom to Diagnosis (4th Ed):
Risk Stratification (AUA Guidelines)
High-risk features requiring urgent and thorough evaluation:
- Age > 35-40 years
- Male sex
- Smoking history (accounts for 60% of bladder cancers in males)
- Occupational chemical exposure (aromatic amines, aniline dyes, rubber workers, miners, hairdressers)
- Prior pelvic radiation
- Chronic UTI / schistosomiasis (endemic areas)
- Alkylating chemotherapy history (cyclophosphamide)
- Analgesic abuse
- Prior urothelial cancer history
Low-risk patients (young women, likely UTI-related): cystoscopy may be deferred initially.
Outpatient Prescription Summary
1. Urinalysis with microscopy - immediately
2. Urine culture and sensitivity - immediately
3. Renal function + CBC + coagulation - blood tests
4. CT Urogram - urgent outpatient referral (within 2 weeks)
5. Cystoscopy - urgent urology referral (within 2 weeks for high-risk; mandatory for gross hematuria)
6. Urine cytology - recommended in patients with gross hematuria or persistent hematuria after negative initial workup
7. PSA - in men, after counselling
Do NOT prescribe:
- Empirical antibiotics unless culture-confirmed UTI
- Iron/haematinics without a confirmed diagnosis
- Haemostatics as outpatient for frank haematuria without completing workup first
Regarding Refusal of Admission
If admission is truly not possible:
- Document the refusal clearly in notes - informed refusal with explanation of cancer risk
- Expedite outpatient investigations - arrange CT urogram and urology referral within 1-2 weeks
- Safety-net: Instruct patient to return to ER immediately if:
- Clot retention / inability to void
- Haemodynamic instability / heavy bleeding
- Urinary retention
- Consider flexible cystoscopy as day-procedure (no admission required)
- Admission would be indicated for: clot retention, haemodynamic compromise, or inability to pass urine - these are absolute indications
Key Teaching Points
- Never attribute gross hematuria to anticoagulants without full workup - malignancy co-exists
- Even intermittent hematuria must be evaluated - bladder cancer bleeds intermittently, giving false reassurance between episodes
- Urine cytology has low sensitivity alone (misses well-differentiated tumors); cystoscopy cannot be replaced by any imaging or marker
- Cystoscopy + biopsy is the gold standard diagnosis for bladder cancer
- If initial full workup is negative: annual urinalysis surveillance for 2 years; repeat cystoscopy if hematuria persists
Sources: Campbell-Walsh-Wein Urology (9780323546423); Symptom to Diagnosis 4th Ed (9781260121117); Textbook of Family Medicine 9th Ed (9780323239905); Harrison's Principles of Internal Medicine 22E
Write the rx
Here is the outpatient prescription for painless hematuria:
Rx — Painless Hematuria (Outpatient)
Investigations
- Urine microscopy, culture & sensitivity — stat
- Urine protein-creatinine ratio (spot) — stat
- CBC, RFT (creatinine, BUN), LFT, coagulation screen — stat
- PSA (male patients, after counselling)
- CT Urogram (abdomen + pelvis with delayed phase) — urgent, within 1 week
- Urine cytology (3 consecutive morning samples)
- Flexible cystoscopy — urology referral, within 2 weeks
Medications
-
Tab. Tranexamic Acid 500 mg — TDS × 5 days (haemostatic - only if active visible bleeding; omit if not needed)
-
Tab. Tamsulosin 0.4 mg — OD at night × 2 weeks (alpha-blocker to ease voiding if lower urinary tract symptoms present; especially in males)
-
Tab. Cranberry Extract / D-Mannose — as per pack — BD (adjunct urinary health support; optional)
If urine culture positive → treat per sensitivity report (e.g., Tab. Nitrofurantoin 100 mg SR BD × 7 days OR Tab. Cotrimoxazole 960 mg BD × 7 days depending on organism)
Referrals
- Urology — urgent (flexible cystoscopy + further evaluation)
- Nephrology — if proteinuria, red cell casts, elevated creatinine, or hypertension present
Advice to Patient
- Increase fluid intake (2-3 L water/day)
- Avoid NSAIDs and nephrotoxic drugs
- Stop smoking immediately
- Return to ER immediately if:
- Unable to pass urine (clot retention)
- Heavy / continuous bleeding
- Dizziness, fainting, or drop in blood pressure
- Attend all follow-up investigations as scheduled
- Do NOT ignore even if bleeding appears to stop — bladder cancer bleeds intermittently
Follow-up: Within 1 week with investigation results
Note: No admission required at this stage provided patient is haemodynamically stable, able to void freely, and investigations are arranged urgently. Informed refusal of admission documented.
This is a shared conversation. Sign in to Orris to start your own chat.