Countercurrent mechanism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive explanation of the countercurrent mechanism in the kidney:
Countercurrent Mechanism
The countercurrent mechanism is the process by which the kidney generates and maintains a corticopapillary osmotic gradient in the renal medulla (300 mOsm/L at the cortex → up to 1200–1400 mOsm/L at the papilla), enabling concentration of urine. It has two distinct components:
- Countercurrent multiplication — Loop of Henle (active process, creates the gradient)
- Countercurrent exchange — Vasa recta (passive process, preserves the gradient)
Overview
A countercurrent system is one where inflow runs parallel to, counter to, and in close proximity to the outflow over some distance. This applies to both the loop of Henle and the vasa recta in the renal medulla. About 25% of nephrons are juxtamedullary nephrons with long loops that extend deep into the medulla — these are essential for generating the maximum osmotic gradient.
Part 1: Countercurrent Multiplication (Loop of Henle)
Anatomical basis
- Thin descending limb (TDL): highly permeable to water (via aquaporin-1), relatively impermeable to solutes
- Thick ascending limb (TAL): actively transports Na⁺/K⁺/2Cl⁻ (NKCC2 cotransporter), impermeable to water
- Thin ascending limb (in juxtamedullary nephrons): impermeable to water, but permeable to NaCl
The Two-Step Repeating Process
Step 1 — The Single Effect:
The TAL actively pumps NaCl out into the medullary interstitium (via Na⁺-K⁺-2Cl⁻ cotransporter), but water cannot follow (TAL is water-impermeable). This creates a ~200 mOsm/L concentration gradient between the tubular lumen and the interstitium. The interstitial osmolarity rises, and because the TDL is water-permeable, water exits the TDL to equilibrate — raising TDL fluid osmolarity.
Step 2 — Flow of Tubular Fluid:
New isoosmotic fluid (300 mOsm/L) continuously enters the TDL from the proximal tubule and pushes the concentrated fluid down toward the loop's bend. Meanwhile, dilute fluid leaves the TAL into the distal tubule. This reduces the concentration gradient against which the pump must work, so more NaCl is pumped out.
By repeating this cycle, osmolarity progressively builds up from cortex to papilla.
Stepwise diagram (Ganong's):
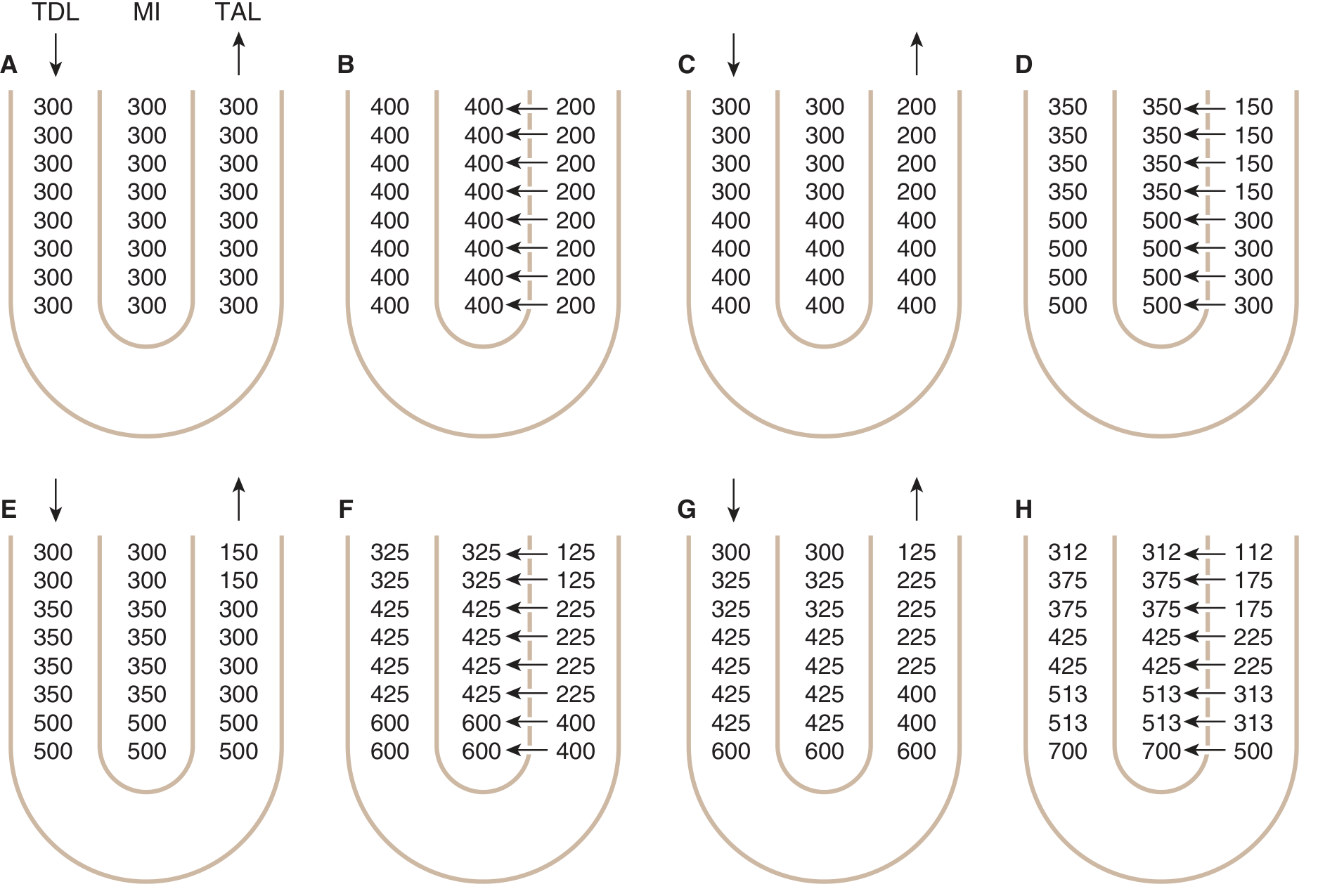
Fig. 37-15 (Ganong's) — Progressive stepwise generation of the medullary osmotic gradient. Numbers are osmolalities (mOsm/kg H₂O) in the TDL, medullary interstitium (MI), and TAL.
Role of juxtamedullary nephrons
In nephrons with longer loops and thin ascending limbs, the osmotic gradient is spread over a greater distance and osmolality at the loop tip is higher. The thin ascending limb is water-impermeable but permeable to NaCl, so NaCl diffuses passively down its concentration gradient into the interstitium — passive countercurrent multiplication. The longer the loop, the greater the maximum papillary osmolality achievable.
Part 2: Role of Urea
Urea accounts for ~40–50% of the papillary osmolarity. In the inner medullary collecting duct (IMCD), ADH upregulates urea transporters (UT-A1, UT-A3), allowing urea to diffuse out into the medullary interstitium. This urea then enters the thin descending limb and thin ascending limb of the loop of Henle, recycling through the system and amplifying the osmotic gradient. A high-protein diet increases urinary urea and enhances concentrating ability; a low-protein diet diminishes it.
Part 3: Countercurrent Exchange (Vasa Recta)
The vasa recta are hairpin-shaped capillaries that descend into and ascend from the medulla alongside the loop of Henle. Only ~5% of renal blood flow perfuses the medulla — this slow flow is critical.
Mechanism (purely passive):
- As blood descends, it is exposed to increasingly hyperosmotic interstitium → solutes (NaCl, urea) diffuse in, water diffuses out → blood osmolarity rises to ~1200 mOsm/L at the tip
- As blood ascends, the reverse occurs → solutes diffuse out, water diffuses in
The net result: most solutes deposited in the medulla are "trapped" and recirculated locally rather than being washed out into the systemic circulation.
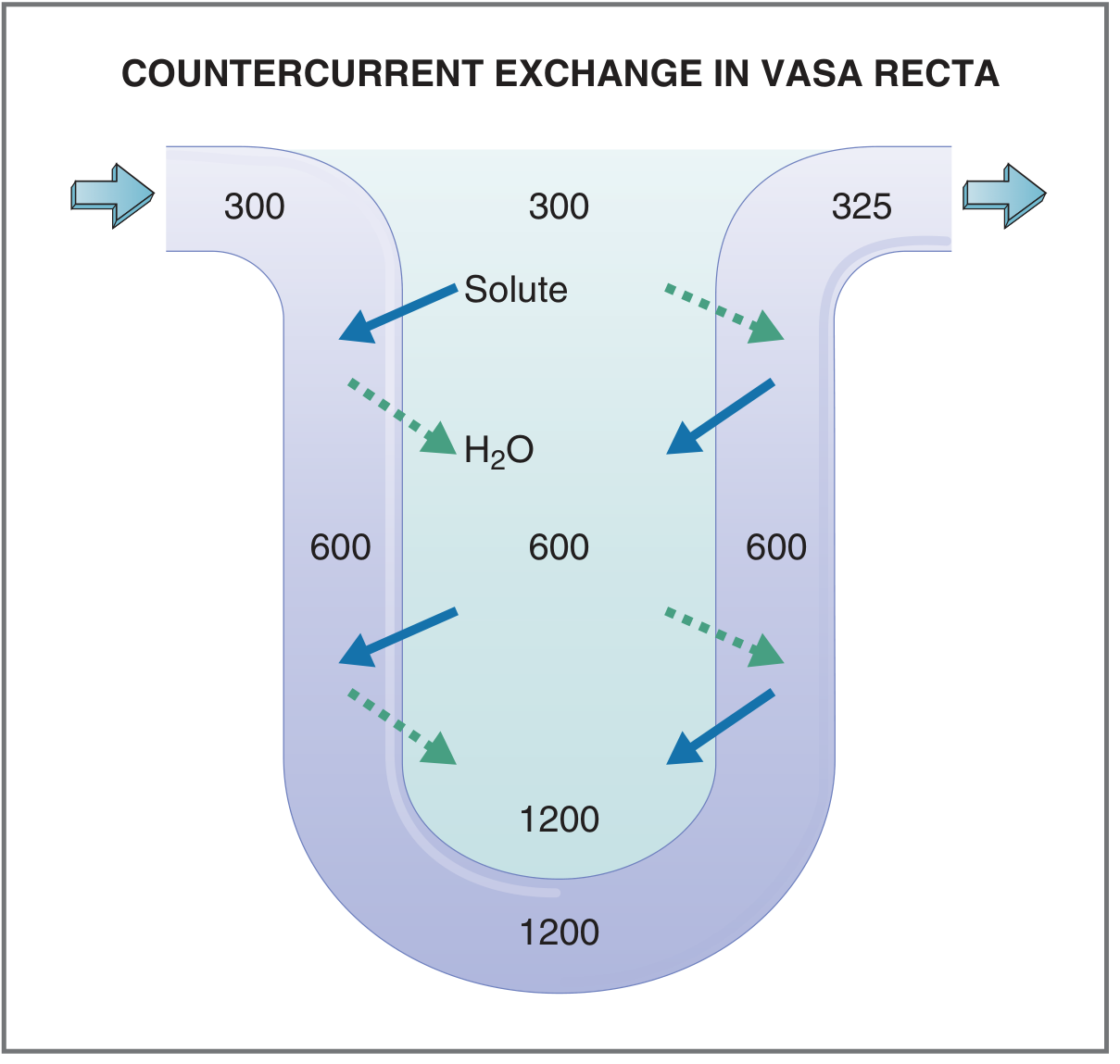
Countercurrent exchange in the vasa recta. Blood entering at 300 mOsm/L exits at only ~325 mOsm/L, preserving the medullary gradient.
Note: The gradient does slowly dissipate via the vasa recta, but is continuously replenished by countercurrent multiplication and urea recycling.
Tubule Permeability Summary (Guyton & Hall)
| Segment | Active NaCl Transport | H₂O Permeability | NaCl Permeability | Urea Permeability |
|---|---|---|---|---|
| Thin descending limb | 0 | ++ | + | + |
| Thin ascending limb | 0 | 0 | + | + |
| Thick ascending limb | ++ | 0 | 0 | 0 |
| Inner medullary collecting duct | + | +ADH | 0 | +ADH |
Role of ADH
ADH (vasopressin) acts at three levels to enhance concentrating ability:
- Increases water permeability of principal cells in the late distal tubule and collecting duct (via aquaporin-2 insertion)
- Increases activity of the Na⁺-K⁺-2Cl⁻ cotransporter in the TAL → augments countercurrent multiplication
- Increases urea permeability in the IMCD → enhances urea recycling
In states of high ADH (dehydration), the corticopapillary gradient is maximally built up and dilute urine from the TAL is reabsorbed as it passes through the collecting duct → concentrated urine. In ADH deficiency (central DI) or ADH resistance (nephrogenic DI), the gradient is diminished and large volumes of dilute urine are excreted.
Sources: Ganong's Review of Medical Physiology (26th ed.), Costanzo Physiology (7th ed.), Guyton & Hall Textbook of Medical Physiology.
This is a shared conversation. Sign in to Orris to start your own chat.