Treatment of IBS-D in an 40 year old female
Reading File
Finding Sources
Searching PubMed
"irritable bowel syndrome" AND "diarrhea" AND treatment
Searching the Web
IBS-D treatment guidelines 2024 2025 female alosetron rifaximin
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have comprehensive data from multiple textbooks and current guidelines. Let me now compile the full, structured answer.
Treatment of IBS-D in a 40-Year-Old Female
IBS-D (diarrhea-predominant IBS) is characterized by chronic abdominal pain, urgency, and loose/frequent stools. In a 40-year-old woman, the treatment approach is stepwise, combining lifestyle modifications, general pharmacotherapy, and IBS-D–specific agents — with alosetron holding a special FDA indication for women.
1. General Principles & Non-Pharmacologic Measures
- Dietary modifications: Low-FODMAP diet reduces fermentable substrates and is effective for global IBS symptoms. Soluble fiber (psyllium) may help regulate stool consistency.
- Psychosocial/behavioral therapy: CBT, gut-directed hypnotherapy, and mindfulness have evidence for reducing IBS symptom severity.
- Patient education: Reassurance about the benign nature of the condition is important for adherence and symptom management.
- Avoid triggers: Caffeine, alcohol, large fatty meals, and insoluble fiber can worsen diarrhea.
2. First-Line Pharmacotherapy
Loperamide (Imodium)
- Mechanism: μ-opioid receptor agonist → slows intestinal transit, reduces stool frequency
- Dose: 2–16 mg/day; most effective when taken prophylactically before predictable events
- Evidence: Reduces stool frequency and urgency, but does not improve abdominal pain or bloating
- AGA recommendation: Conditional, moderate evidence; generally used as first symptomatic measure
- Cautions: Avoid overuse; no major systemic effects at standard doses
Tricyclic Antidepressants (TCAs)
- Agents: Amitriptyline, desipramine, nortriptyline — 10–50 mg/day (sub-antidepressant dose)
- Mechanism: Alters central processing of visceral afferent pain; anticholinergic properties reduce stool frequency and liquidity; modulates enteric serotonin receptors
- AGA recommendation: Conditional, moderate evidence for pain and global symptoms
- Note: SSRIs are not recommended by AGA for IBS (insufficient evidence, conditional recommendation against)
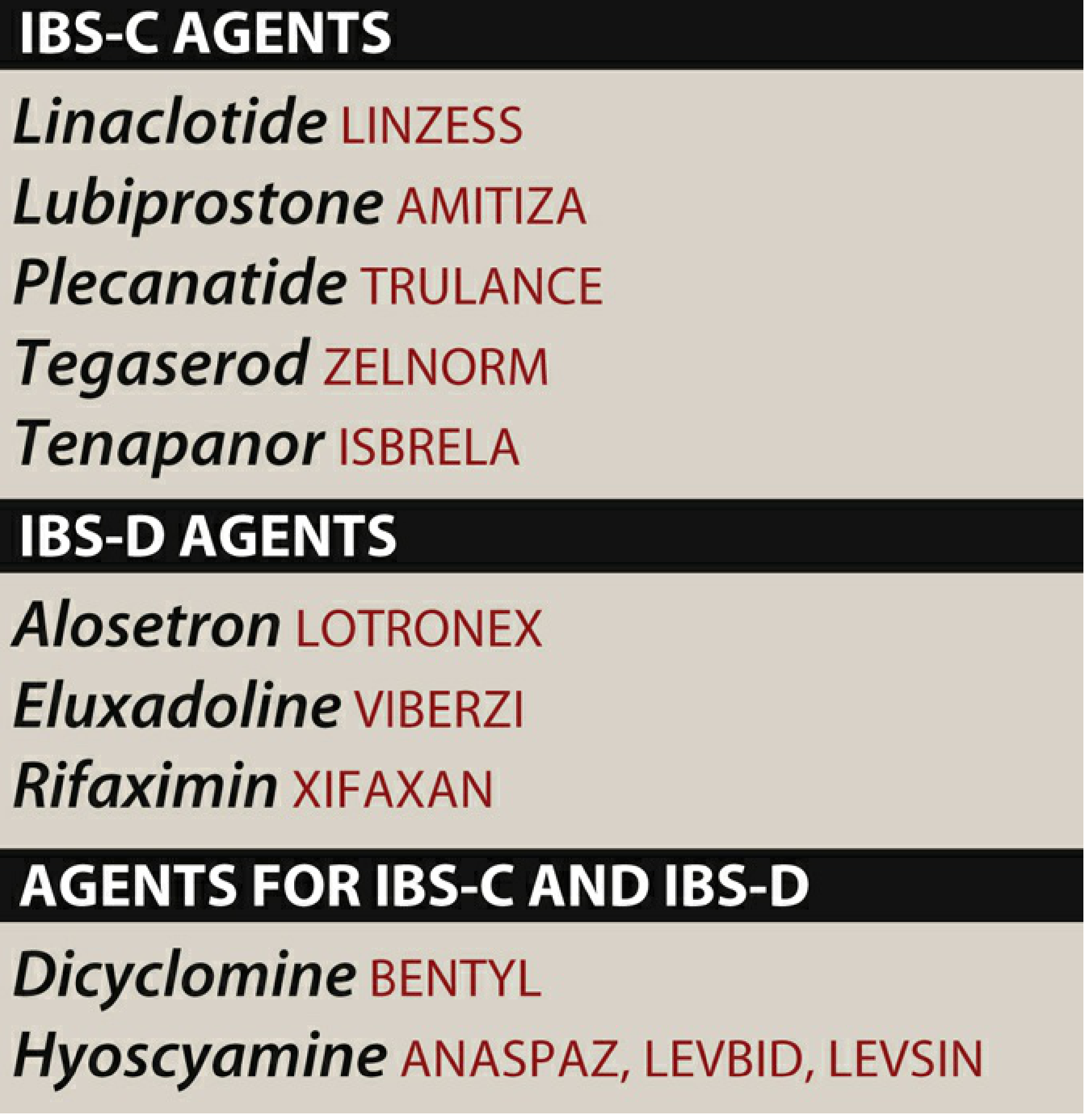
Antispasmodics (Anticholinergics)
- Agents: Dicyclomine (Bentyl), hyoscyamine (Levsin) for both IBS-C and IBS-D
- Mechanism: Antimuscarinic → reduces GI spasm and motility
- Evidence: Meta-analysis (NNT ~5) for pain and global symptoms; long-term efficacy not firmly established
- Adverse effects: Anticholinergic: dry mouth, blurred vision, urinary retention, constipation
- Also: Peppermint oil (180–200 mg TID, 30 min before meals) — NNT ~3, well tolerated; heartburn/perianal burning can occur
3. IBS-D–Specific Agents
A. Rifaximin (Xifaxan) ⭐ First-line IBS-D specific
- Mechanism: Non-absorbable antibiotic (rifampin analog) → reduces luminal bacterial load, decreases fermentation and gas production
- Dose: 550 mg TID × 14 days
- Efficacy: Improves global symptoms, bloating, stool consistency; ~10.5% absolute benefit over placebo (NNT ~8–16)
- Retreatment: Evidence supports re-treatment with the same regimen if symptoms recur after initial response
- Safety: Excellent — profile similar to placebo; low systemic absorption; minimal C. difficile risk; low resistance concern
- AGA recommendation: Conditional, moderate evidence (2a/2b)
B. Eluxadoline (Viberzi) ⭐ Approved for IBS-D
- Mechanism: Mixed opioid receptor modulator — μ-opioid agonist (slows transit) + δ-opioid antagonist + κ-opioid agonist → reduces pain and diarrhea without typical opioid systemic effects
- Dose: 75 mg or 100 mg BID
- Efficacy: ~27% response vs. 17% placebo (phase III trials); NNT ~7–15
- Contraindications: Prior cholecystectomy (no gallbladder → risk of sphincter of Oddi spasm), alcohol dependence (>3 drinks/day), pancreatitis, hepatic impairment
- AGA recommendation: Conditional, moderate evidence
C. Alosetron (Lotronex) ⭐ Female-specific, second-line
- Mechanism: Selective 5-HT₃ receptor antagonist → reduces visceral afferent pain, slows colonic transit (especially left colon)
- Dose: 0.5 mg BID (start); may titrate to 1 mg BID
- Efficacy: 50–60% adequate relief vs. 30–40% placebo; reduces pain, urgency, stool frequency
- FDA indication: Women only with severe IBS-D who have failed conventional therapies — NNT ~8
- Serious adverse effects:
- Constipation (up to 30%; drug discontinuation in 10%)
- Ischemic colitis (up to 3/1000 patients — some fatal)
- Severe constipation complications requiring hospitalization (1/1000)
- REMS program required: Prescribers must be enrolled; patient must sign informed consent
- ACG position: Second-line for women with severe IBS-D not responding to conventional therapy
- This patient: A 40-year-old woman is an appropriate candidate if conventional therapies fail
4. Drug Summary Table (IBS-D Specific)
| Drug | Brand | Mechanism | Key AE | Notes |
|---|---|---|---|---|
| Loperamide | Imodium | μ-opioid agonist | Constipation | OTC; no pain benefit |
| Rifaximin | Xifaxan | Non-absorbable antibiotic | Rare C. diff | 14-day course; retreatable |
| Eluxadoline | Viberzi | μ/δ/κ opioid modulator | Pancreatitis, constipation | Avoid if no gallbladder |
| Alosetron | Lotronex | 5-HT₃ antagonist | Ischemic colitis, constipation | Women only, REMS |
| Dicyclomine | Bentyl | Antimuscarinic | Anticholinergic | Both IBS-C & IBS-D |
| TCA (amitriptyline) | Elavil | Central/enteric modulation | Sedation, dry mouth | Low dose for pain |
5. Stepwise Management Algorithm
Step 1 (All patients):
→ Dietary modification (low-FODMAP), trigger avoidance, education
Step 2 (Symptomatic relief):
→ Loperamide (urgency/stool frequency) ± antispasmodic/peppermint oil (pain)
→ TCA at low dose if pain is prominent
Step 3 (IBS-D specific — first line):
→ Rifaximin 550 mg TID × 14 days
(retreatment if recurrence)
Step 4 (If inadequate response):
→ Eluxadoline 75–100 mg BID
(avoid if cholecystectomy/alcohol dependence)
Step 5 (Severe, refractory — women only):
→ Alosetron 0.5–1 mg BID (via REMS)
(after failure of conventional therapy)
Comorbid anxiety/depression:
→ TCA preferentially; consider psychological interventions (CBT, hypnotherapy)
6. Special Considerations in a 40-Year-Old Woman
| Consideration | Clinical Implication |
|---|---|
| Alosetron eligibility | Approved only for women — this patient qualifies if severe and refractory |
| Eluxadoline caution | Ask about prior cholecystectomy and alcohol use before prescribing |
| TCAs | Effective; also treat comorbid anxiety/insomnia common in IBS; avoid in suicidal ideation |
| Pregnancy potential | Lubiprostone (Category C) should be avoided if there is pregnancy potential |
| Bile acid diarrhea | Up to 30% of IBS-D patients may have idiopathic bile acid diarrhea — bile acid sequestrants (e.g., cholestyramine) can be a diagnostic-therapeutic trial |
Recent Evidence (2023–2026)
- Probiotics (PMID 37686889): Network meta-analysis (2023) shows strain-specific benefits; no universal recommendation yet.
- Mesalamine (PMID 36858143): Meta-analysis (CGH 2024) shows no significant benefit in IBS — not recommended.
- Acupuncture (PMID 39560589): Meta-analysis (2024) supports acupuncture for IBS-D with comorbid anxiety/depression as adjunct therapy.
- 2025 Seoul Consensus: Reaffirms rifaximin (moderate evidence, weak recommendation) and 5-HT₃ antagonists (high evidence) as effective in IBS-D; alosetron proposed as second-line in women with severe symptoms.
Sources: Katzung's Basic & Clinical Pharmacology 16e | Sleisenger & Fordtran's GI & Liver Disease | Lippincott Illustrated Reviews: Pharmacology | Harrison's Principles of Internal Medicine 22e | AGA Clinical Practice Guidelines on IBS-D (2022) | ACG Guidelines | 2025 Seoul Consensus
This is a shared conversation. Sign in to Orris to start your own chat.