Can u plz tell me authentically what is carnet sign actually is?
Carnett sign clinical examination abdominal wall pain
Carnett's Sign
What Is It?
How to Perform It (Step by Step)
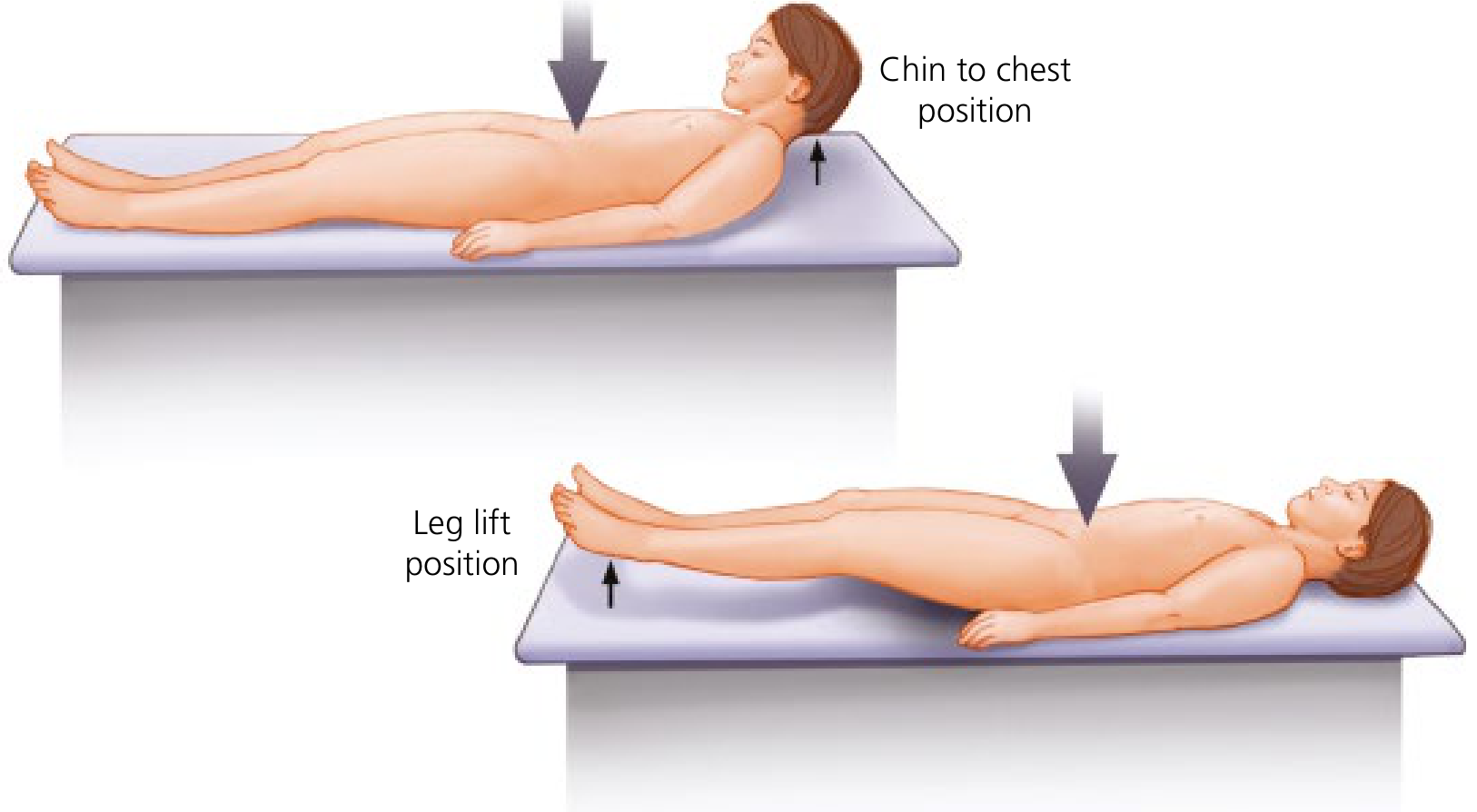
- Position: Have the patient lie supine on the examination table with abdominal muscles relaxed (legs can be slightly bent to help relaxation).
- Locate the tender point: Ask the patient to point with one finger to the spot of maximum pain/tenderness. This is important - it should be a focal, localized area.
- Baseline palpation: Apply firm, steady pressure with your fingertip to that point while the muscles are still relaxed. Note the level of pain.
- Muscle tensing: Keeping your finger at the same spot and pressure, ask the patient to either:
- Lift their head and shoulders off the table (chin-to-chest position, like a partial sit-up), OR
- Raise both legs off the table with knees extended
- Both maneuvers contract the anterior abdominal wall muscles equally well.
- Interpret the result: Does the pain increase, stay the same, or decrease?
Interpretation
| Result | Meaning |
|---|---|
| Pain stays the same or WORSENS (Positive Carnett) | Pain is from the abdominal wall |
| Pain DECREASES or disappears (Negative Carnett) | Pain is likely visceral/intra-abdominal in origin |
- Sabiston Textbook of Surgery, 21st ed.: "Carnett sign - Continued or increased abdominal pain when abdominal wall muscles are tensed - Abdominal wall source of pain."
- Yamada's Textbook of Gastroenterology, 7th ed.: "Worsening abdominal pain on contraction of the abdominal wall muscle" = positive test; associated conditions include cutaneous nerve entrapment, myofascial pain syndromes, rectus sheath hematoma, and rib tip syndrome.
What Causes a Positive Carnett Sign?
- Anterior Cutaneous Nerve Entrapment Syndrome (ACNES) - the most common cause. The anterior cutaneous branches of intercostal nerves (T7-T12) become trapped as they pierce the rectus abdominis fascia. This accounts for 10-30% of patients with chronic abdominal pain in gastroenterology practice.
- Myofascial Pain Syndrome (MFPS) - pain from trigger points in the abdominal skeletal muscle.
- Rectus sheath hematoma - bleeding into the rectus muscle sheath (often post-trauma or anticoagulant use).
- Rib tip syndrome (slipping rib).
- Post-surgical scar pain - pain in healed abdominal incisions that worsens with head-flexion confirms an abdominal wall source.
Clinical Significance
- Avoids unnecessary investigations: A positive Carnett sign redirects the clinician away from expensive GI workups and toward abdominal wall-specific diagnoses.
- Harrison's Principles (22nd ed., 2025) explicitly states: "Patients with an abdominal wall source of upper abdominal pain may exhibit a positive Carnett's sign of increased tenderness with tensing of abdominal muscles upon lifting the head from the pillow."
- Sleisenger & Fordtran's GI and Liver Disease notes the sign is also seen in Centrally Mediated Abdominal Pain Syndrome (CAPS), where it can be harder to interpret.
Limitations and Caveats
- The sign can be difficult to interpret in patients with psychogenic or functional abdominal pain (CAPS), where pain may appear to worsen regardless.
- It requires patient cooperation and the ability to contract abdominal muscles.
- A modified Carnett test exists for pelvic pain during bimanual examination.
- Confirmatory test: if Carnett is positive, injection of local anesthetic (e.g., 1% lidocaine) at the tender point that produces ≥50% pain relief confirms the abdominal wall diagnosis and guides treatment with a corticosteroid-anesthetic trigger point injection (typically lidocaine + triamcinolone 40 mg), which has a 70-99% response rate for ACNES.
- Yamada's Textbook of Gastroenterology, 7th ed., Chapter 34
- Sabiston Textbook of Surgery, 21st ed., Table 85-4
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter on Abdominal Wall Pain
- Harrison's Principles of Internal Medicine, 22nd ed. (2025)
- AAFP Clinical Review: Abdominal Wall Pain evaluation
Thanks
Tell me now what is fothergill sign/test?
Fothergill sign test abdominal wall mass rectus sheath clinical examination
Fothergill Sign
What Is It?
How to Perform It
- Position: Patient lies supine, muscles relaxed.
- Locate the mass: Palpate and identify the abdominal mass.
- Muscle contraction: Ask the patient to tense the abdominal wall by either:
- Lifting the head and shoulders off the table (chin-to-chest), OR
- Raising both legs with knees extended
- Observe what happens to the mass during contraction.
Interpretation
| Result | Meaning |
|---|---|
| Mass remains palpable and becomes FIXED (Positive Fothergill) | Mass is in the abdominal wall (e.g., rectus sheath hematoma) |
| Mass becomes LESS distinct or impalpable (Negative Fothergill) | Mass is intra-abdominal / visceral in origin |
Sabiston Textbook of Surgery, 21st ed.: "Fothergill sign - Abdominal wall mass that does not cross the midline and is palpable when the rectus is contracted - Rectus sheath hematoma."
Schwartz's Principles of Surgery, 11th ed.: "Palpation of a mass that does not change during contraction of the rectus muscle, known as Fothergill's sign, is also associated with rectus sheath pathology."
StatPearls / NCBI: "The mass remains palpable (Fothergill sign), suggesting an abdominal wall source rather than an intra-abdominal etiology."
Classic Association: Rectus Sheath Hematoma (RSH)
- Anticoagulant therapy (most common in modern practice)
- Vigorous coughing, sneezing, or exercise (forceful rectus contraction)
- Abdominal trauma or iatrogenic injury (e.g., laparoscopic trocar placement)
- Chronic pulmonary disease (repeated coughing fits)
- Pregnancy
- Acute, sudden-onset abdominal pain
- Palpable, firm, non-pulsatile, tender abdominal mass
- Mass does NOT move with respiration
- Mass typically does NOT cross the midline (important feature)
- Positive Fothergill sign (mass persists with muscle contraction)
- Positive Carnett sign (pain worsens with muscle contraction)
- Possible ecchymosis (bruising) on the abdominal wall
Fothergill Sign vs. Carnett Sign - Side by Side
| Feature | Carnett Sign | Fothergill Sign |
|---|---|---|
| What is tested | Pain | The mass |
| Positive finding | Pain increases on muscle contraction | Mass stays fixed/palpable on muscle contraction |
| Primary use | Diagnose abdominal wall pain | Diagnose abdominal wall mass |
| Main association | ACNES, myofascial pain, RSH | Rectus sheath hematoma |
Important Additional Notes
- The sign can be inconclusive in obese or pregnant patients because the mass may be too deep to assess accurately with or without contraction.
- Confirmation: Ultrasound (80-90% sensitivity) or CT abdomen with IV contrast (100% sensitivity) should be used to confirm the diagnosis - CT is the gold standard.
- Treatment of RSH depends on hemodynamic stability: stable small hematomas can be observed; larger ones may need hospitalization, blood products, or angiographic embolization; surgery (hematoma evacuation + vessel ligation) is reserved for cases where embolization fails.
- Sabiston Textbook of Surgery, 21st ed., Table 85-4
- Schwartz's Principles of Surgery, 11th ed., Chapter on Acquired Abdominal Wall Abnormalities
- StatPearls - Rectus Sheath Hematoma (NCBI Bookshelf)
- Medscape: Rectus Sheath Hematoma - Clinical Presentation
What if a mass is felt mildly in epigastric region and if head is elevated again resistance and the mass protrude out. What it shows?
epigastric mass protrudes head elevation Valsalva linea alba hernia epigastric hernia diagnosis
Epigastric Mass That Protrudes on Head Elevation
1. Epigastric Hernia (Most Likely Diagnosis)
Why does it protrude more on head raising?
Classic Features (from S. Das Manual on Clinical Surgery, 13th ed.):
- Small, round midline swelling between the xiphisternum and umbilicus
- Usual patient is a strong muscular labourer (classically)
- Three stages:
- Sacless herniation of extraperitoneal fat through linea alba - no symptoms
- A pouch of peritoneum is drawn in
- A small tag of omentum enters and adheres to the sac - patient now gets dragging pain, discomfort after food (mimicking peptic ulcer)
- The mass cannot be moved over the underlying structures - this favours epigastric hernia over lipoma
- Often no impulse on coughing and frequently cannot be reduced (because the omental tag gets adherent)
- Pain is localized to the hernia site, not deep visceral pain
On examination maneuver:
2. Divarication of the Recti (Diastasis Recti) - Important Differential
How it looks:
- On head raising, a broad, fusiform midline bulge appears between the two visible rectus muscles
- It can look dramatic and alarming
- But there is NO discrete hernial sac, NO ring you can feel around it, and the bulge is very wide and long (not a focal small lump)
Key distinguishing points:
| Feature | Epigastric Hernia | Diastasis Recti |
|---|---|---|
| Defect type | True hole in linea alba | Stretching/thinning of linea alba, no hole |
| Fascial ring | Present - you can feel a firm ring around it | Absent - wide, soft, diffuse |
| Size of bulge | Small and focal | Broad and elongated |
| Risk of strangulation | YES - contents can strangulate | NO - not a true hernia |
| Needs surgery | Yes if symptomatic | No - cosmetic only |
| Common in | Muscular labourers, men | Multiparous women, obese patients, elderly |
Sleisenger & Fordtran's GI and Liver Disease: "Diastasis recti is a separation of the rectus abdominis muscles without a defect in the abdominal fascia and can be demonstrated as a midline defect exaggerated by a Valsalva maneuver. No fascial ring can be palpated, and the defect is often very wide and long. This condition does not require repair and is cosmetic only."
Schwartz's Principles of Surgery, 11th ed.: "A fusiform bulge is usually apparent. This bulge worsens with contraction of the rectus muscles or Valsalva maneuver."
Summary: What Does It Show?
| Scenario | Diagnosis |
|---|---|
| Small, focal, hard-edged midline lump in epigastrium that protrudes more on head raising, with a palpable ring around it | Epigastric Hernia |
| Broad, soft, diffuse midline bulge on head raising, no ring felt, very wide defect | Diastasis Recti (not a true hernia) |
- S. Das Manual on Clinical Surgery, 13th ed.
- Sleisenger & Fordtran's GI and Liver Disease - Other Ventral Hernias
- Schwartz's Principles of Surgery, 11th ed. - Rectus Abdominis Diastasis
- Merck Manual Professional Edition - Hernias of the Abdominal Wall
What is valsalva manuver and why it is done
Valsalva maneuver physiology indications clinical uses
The Valsalva Maneuver
What Is It?
How to perform it:
- The patient takes a deep breath and holds it
- Then bears down (strains) as if trying to push the air out but does not let it escape
- This is maintained for 10-20 seconds
- Alternatively: ask the patient to blow into their thumb (closing lips around it), OR push against the examiner's hand placed on the abdomen
What this creates:
- A sharp rise in intrathoracic pressure (30-40 mmHg)
- A simultaneous rise in intra-abdominal pressure
The 4 Phases of the Valsalva Maneuver
| Phase | What Happens | Physiological Mechanism |
|---|---|---|
| Phase I (Strain onset) | Transient rise in blood pressure | Raised intrathoracic pressure squeezes blood out of pulmonary vessels into the aorta |
| Phase II (Sustained strain) | Blood pressure falls, heart rate rises (tachycardia) | Raised intrathoracic pressure reduces venous return to the heart → reduced stroke volume → baroreceptors trigger reflex tachycardia and peripheral vasoconstriction |
| Phase III (Release) | Blood pressure drops further briefly | Sudden drop in intrathoracic pressure creates a transient suction effect on blood |
| Phase IV (Recovery) | Blood pressure overshoots above baseline, heart rate slows (bradycardia) | Venous return floods back → increased cardiac output → baroreceptors trigger reflex parasympathetic bradycardia |
Adams & Victor's Principles of Neurology, 12th ed.: "With the release of intrathoracic pressure, the venous return, stroke volume, and blood pressure rise to higher-than-normal levels; reflex parasympathetic influence then predominates and a bradycardia results."
Why Is It Done? (Clinical Uses)
1. Cardiology - Treating and Diagnosing Arrhythmias
- Most important use: Terminates SVT (Supraventricular Tachycardia)
- The Phase II rise in vagal tone slows AV node conduction, breaking re-entrant circuits
- Roberts & Hedges' Clinical Procedures in Emergency Medicine: "During the Valsalva maneuver, intrathoracic pressure increases and leads to decreased venous return... vagal tone is increased, thereby leading to a compensatory decrease in SA and AV conduction. This is the expected or desired diagnostic or therapeutic response."
- Performed with legs passively elevated (modified Valsalva) for better success rates
2. Cardiology - Differentiating Heart Murmurs
| Murmur | Response in Phase II (↓ venous return) | Why |
|---|---|---|
| Most murmurs (e.g., aortic stenosis) | Decrease (softer) | Less blood = less turbulence |
| Hypertrophic Cardiomyopathy (HCM/HOCM) | Increase (louder) | Smaller LV cavity → more outflow obstruction |
| Mitral Valve Prolapse | Increase (louder, click moves earlier) | Smaller LV → leaflets prolapse more |
Fuster & Hurst's The Heart: "Most systolic murmurs will decrease during [phase II]; the exceptions are the murmurs of mitral valve prolapse and hypertrophic cardiomyopathy."
3. Surgery / General Medicine - Diagnosing Hernias
- Raised intra-abdominal pressure makes occult hernias protrude and become visible
- Used for epigastric hernias, umbilical hernias, inguinal hernias, diastasis recti
- This is exactly the principle used when you ask a patient to lift their head against resistance (as discussed in your previous question)
4. Neurology - Testing Autonomic Function
- Valsalva ratio = max HR during phase II ÷ lowest HR within 30 seconds after
- Normal ratio > 1.5
- Failure of HR to rise in phase II = sympathetic dysfunction
- Failure of HR to slow in phase IV = parasympathetic dysfunction
- Used to diagnose diabetic autonomic neuropathy, Parkinson's disease autonomic failure, etc.
5. Neurology - Spine / Disc Disease
- Raised intraspinal pressure aggravates nerve root compression
- If Valsalva reproduces or worsens radicular (shooting) pain, it suggests a herniated disc or spinal nerve impingement
- Also used to detect dural tears after spinal surgery (CSF leak causes headache)
6. ENT - Ear Pressure Equalization
- Used to open the Eustachian tube and equalize middle ear pressure (e.g., when flying or diving)
- Helps treat barotrauma or serous otitis media
7. Urology/Gynaecology
- Demonstrates stress urinary incontinence (urine leaks on straining)
- Shows maximum pelvic organ prolapse on gynecological examination
- Valsalva Leak Point Pressure - used in urodynamic studies
8. Otolaryngology
- K.J. Lee's Essential Otolaryngology: "Larynx closes tightly with inflated lungs - stabilizes thorax for muscular actions (e.g., heavy lifting); increases intra-abdominal pressure for defecation, vomiting, and childbirth"
Contraindications (When NOT to Do It)
- Severe coronary artery disease (sudden hemodynamic swings can trigger ischemia)
- Known aortic aneurysm or aortic dissection
- Recent eye surgery (raises intraocular pressure)
- Glaucoma
- Stroke risk (transiently reduces cerebral perfusion)
- Patients who cannot cooperate (dyspneic, agitated)
Simple Summary
| Question | Answer |
|---|---|
| What is it? | Forced expiration against a closed glottis |
| Mechanism | Raises intrathoracic + intra-abdominal pressure |
| Main cardiac use | Terminate SVT, differentiate murmurs |
| Main surgical use | Unmask hidden hernias |
| Main neuro use | Test autonomic function, detect disc prolapse |
| Main ENT use | Equalize ear pressure (Eustachian tube) |
- Fuster and Hurst's The Heart, 15th ed. - Dynamic Auscultation
- Adams and Victor's Principles of Neurology, 12th ed. - Autonomic Testing
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - SVT management
- K.J. Lee's Essential Otolaryngology
- Sleisenger & Fordtran's GI and Liver Disease - Hernia diagnosis
What manuver is done to see diverication of recti or epigastric hernia?
head raising test divarication recti epigastric hernia examination maneuver difference
Maneuvers Used to Detect Divarication of Recti and Epigastric Hernia
The Maneuvers Used
1. Head-Raising Test (Primary Maneuver)
- Patient lies supine, muscles relaxed
- Ask them to lift their head and shoulders off the table (like a partial sit-up / chin-to-chest)
- This is the single most important bedside test for both conditions
2. Valsalva Maneuver / Coughing
- Ask the patient to cough forcefully, OR
- Ask them to bear down / strain (Valsalva)
- Both sharply raise intra-abdominal pressure
3. Straight Leg Raise (Alternative)
- Patient lies supine and raises both legs together off the table with knees straight
- This also contracts the abdominal wall and raises intra-abdominal pressure
What Each Condition Looks Like Under These Maneuvers
| Feature | Divarication of Recti (Diastasis Recti) | Epigastric Hernia |
|---|---|---|
| What appears | Broad, soft, fusiform (spindle-shaped) ridge running down the midline | Small, focal, round lump exactly in the midline |
| Width | Wide - often several centimetres across | Narrow - fingertip-sized |
| Fascial ring | ABSENT - no firm edge around it | PRESENT - you can feel a firm ring/defect around it |
| Reducible? | Not applicable (no true sac) | Often NOT reducible (omental tag gets stuck) |
| Impulse on cough | Diffuse bulge with no discrete impulse | May or may not have impulse |
| Pain | Usually none | Pain localized to the lump |
| Danger | None - no strangulation risk | Yes - can strangulate |
| Needs surgery | No - cosmetic only / physio | Yes if symptomatic |
The Key Clinical Trick to Tell Them Apart
Run your finger along the edge of the bulge and feel for a firm fascial ring.
- Feel a firm edge/ring? → Epigastric hernia (true defect in linea alba with herniated fat/omentum inside a sac)
- No ring, just a wide soft valley between two muscle ridges? → Diastasis recti (muscles separated, fascia merely stretched, no hole)
Step-by-Step Examination Sequence
1. Patient supine, muscles relaxed
→ Inspect and palpate the epigastric region at rest
→ Note any mass at rest
2. Ask patient to raise head and shoulders (head-raising test)
→ Watch the midline carefully
3. If a bulge appears:
→ Feel its width (broad = diastasis; focal = hernia)
→ Feel for a fascial ring around it
→ Try to reduce it (push it back gently)
→ Ask if it is tender
4. Ask patient to cough (Valsalva equivalent)
→ Does the bulge appear / worsen?
5. If still unclear → Ultrasound of the abdominal wall
(can directly measure inter-recti distance and identify a fascial defect)
Important Point About Epigastric Hernia Specifically
Summary in One Line
Both conditions are revealed by the head-raising test (or Valsalva/coughing). Diastasis recti shows a wide, soft, ringless midline ridge; epigastric hernia shows a small, focal lump with a palpable fascial ring around it.
- Schwartz's Principles of Surgery, 11th ed.
- Sleisenger & Fordtran's GI and Liver Disease
- S. Das Manual on Clinical Surgery, 13th ed.
- Emedicine/Medscape - Abdominal Hernias Clinical Presentation
- TeachMeSurgery - Abdominal Hernia
Is fothergill test used for diverication of recti
No - Fothergill Test is NOT for Divarication of Recti
What the Fothergill Sign Requires
- Remains palpable and becomes fixed when the rectus muscle contracts
- Does not cross the midline
Sabiston Textbook of Surgery, 21st ed.: "Fothergill sign - Abdominal wall mass that does not cross midline and is palpable when rectus is contracted - Rectus sheath hematoma"
Why It Cannot Apply to Divarication of Recti
- No discrete lump
- No hernial sac
- No fascial ring
- No palpable solid structure
Sleisenger & Fordtran's GI and Liver Disease: "Diastasis recti is a separation of the rectus abdominis muscles without a defect in the abdominal fascia... No fascial ring can be palpated, and the defect is often very wide and long."
Quick Comparison Table
| Fothergill Sign | Divarication of Recti | |
|---|---|---|
| Requires a mass? | YES - a firm, discrete mass | NO - no mass present |
| Used for? | Rectus sheath hematoma | Not tested with Fothergill |
| On muscle contraction | Mass stays fixed and palpable | A wide soft ridge appears, no mass |
| Fascial defect? | YES (within rectus sheath) | NO (linea alba stretched, not defective) |
| Danger? | YES (can cause significant bleeding) | NO (cosmetic, no strangulation) |