

519c9d24-5191-41bc-9605-ee753801e9fe.jpg
5e16fa54-0ef6-48f9-9e6d-c0efb5fb08f4.jpg
Ok explain me this ecg with corresponding ctpa finding
Reading File
Searching PubMed
pulmonary embolism ECG right heart strain S1Q3T3
Finding Sources
Finding Sources
Searching PubMed
pulmonary embolism ECG electrocardiogram findings
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
I now have all the information needed to give a thorough, referenced answer. Let me compile the full analysis.
ECG + CTPA Analysis: Jayadevan, M/36, Breathlessness
PATIENT SUMMARY
- Patient: Male, 36 years old
- Presenting complaint: Breathlessness
- ECG machine: Cardiart 9108, Glasgow V28.6.0, DH Mananthavady
- CTPA: Govt. Medical College Hospital, Wayanad, Mananthavady (Report date 4.7.26)
ECG ANALYSIS
Measured intervals (from machine):
| Parameter | Value |
|---|---|
| QRS | 100 ms |
| QT/QTc | 372/501 ms |
| P/QRS/T axes | 36/81/-95° |
| RV5/SV1 | 1.414 / 0.584 mV |
Machine interpretation: Right ventricular hypertrophy, right or left atrial abnormality, widespread ST-T abnormality possibly due to hypertrophy.
Manual ECG findings (lead-by-lead):
Rhythm & Rate:
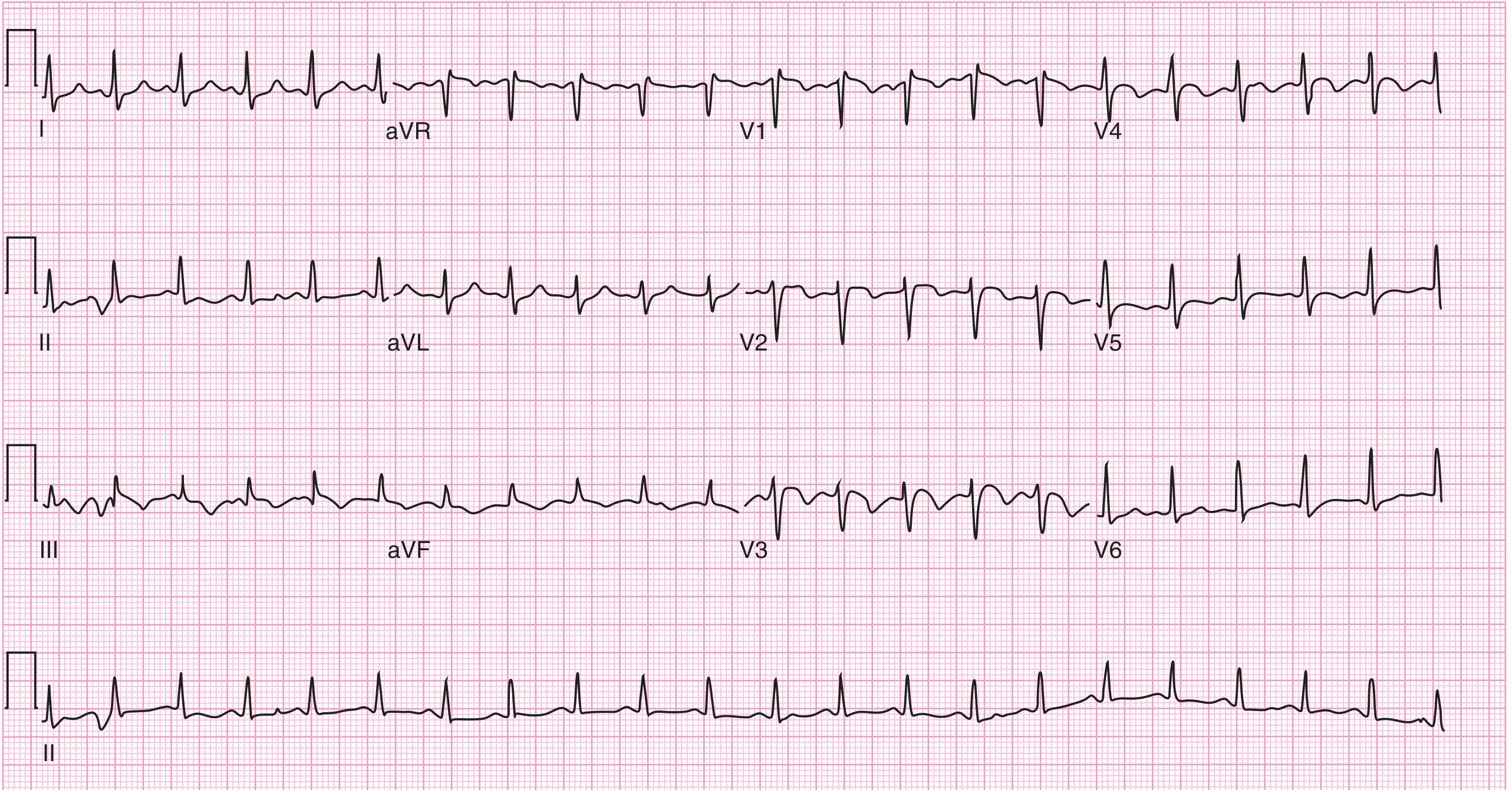
- Sinus tachycardia (~100-110 bpm estimated from tracing density)
The S1Q3T3 Pattern (classic PE sign):
- Lead I: Broad S wave present
- Lead III: Q wave + inverted T wave
- This is the McGinn-White sign / S1Q3T3 - the most cited, though relatively specific but insensitive ECG finding in PE
Right Axis Deviation:
- QRS axis ~+81° - borderline right axis deviation
Right Heart Strain Changes:
- T-wave inversions in V1-V4 (right precordial leads): This is actually the most common ECG abnormality in PE - it reflects RV strain and ischemia. The tracings in V1-V4 show progressive T-wave changes consistent with this.
- QTc of 501 ms - significantly prolonged, reflecting RV strain/ischemia
Atrial Abnormality:
- P-axis of 36° with atrial abnormality flagged by the machine - likely right atrial dilation secondary to increased pulmonary vascular resistance
QRS duration 100 ms: At the upper limit of normal - may represent incomplete RBBB pattern consistent with acute RV pressure overload
ECG Summary Pattern: The combination of sinus tachycardia + S1Q3T3 + right precordial T-wave inversions + right atrial abnormality + QTc prolongation is the classic electrophysiological footprint of acute cor pulmonale from PE with right heart strain.
As Harrison's states: "The most frequently cited abnormality, in addition to sinus tachycardia, is the S1Q3T3 sign... RV strain and ischemia cause the most common abnormality, T-wave inversion in leads V1-V4." (Harrison's Principles of Internal Medicine 22E, p.2203)
Here is the reference ECG from Harrison's showing this classic pattern:
Harrison's Figure 290-11: ECG with S1Q3T3 sign + T-wave inversions in V1-V4, typical of a large PE - this closely mirrors your patient's ECG.
CTPA FINDINGS & CORRELATION
Key CTPA findings and their ECG correlates:
| CTPA Finding | ECG Correlate | Mechanism |
|---|---|---|
| Partial filling defect - subsegmental PA, superior segment RLL | Sinus tachycardia, S1Q3T3 | Acute RV afterload increase from thrombus |
| Mildly dilated pulmonary arteries (MPA = 33 mm; normal <29 mm) | Right precordial T-wave inversions (V1-V4), RV strain | Chronic/acute PAH with RV pressure overload |
| Cardiomegaly | Atrial abnormality on ECG | Cardiac chamber enlargement |
| Prominent IVC and hepatic veins | Right atrial pressure elevation | Increased RV filling pressures backing up into systemic veins |
| Mosaic attenuation of lung parenchyma | - | Heterogeneous perfusion - consistent with chronic thromboembolic disease or pulmonary vascular disease |
| Lung cysts bilaterally + fibrotic bands + traction bronchiectasis | - | Underlying parenchymal lung disease, possibly contributing to PAH |
IMPRESSION: Integrated Clinical Picture
This 36-year-old male has a multi-layered cardiopulmonary diagnosis:
-
Acute-on-chronic PE: Subsegmental thrombus in the right lower lobe on CTPA, but with background features (dilated MPA 33 mm, cardiomegaly, mosaic attenuation, lung cysts, fibrotic bands) that suggest this is not a first-time acute PE. The underlying lung disease and PAH suggest possible chronic thromboembolic pulmonary hypertension (CTEPH) or a connective tissue/ILD-related process contributing to baseline PAH.
-
Right heart strain: Confirmed by both ECG (S1Q3T3, precordial T-inversions, atrial abnormality, prolonged QTc) and CTPA (dilated MPA, cardiomegaly, prominent IVC/hepatic veins).
-
The ECG and CTPA are entirely concordant: Every ECG abnormality maps to a structural CTPA finding.
Immediate priorities:
- ECHO (as recommended in the CTPA report) - to assess RV size/function, TR jet, RV/LV ratio, TAPSE
- Risk stratify the PE: This appears a low-to-intermediate risk PE (subsegmental, hemodynamically stable based on the presentation), but background PAH raises the stakes
- Anticoagulation is the cornerstone
- Investigate underlying cause: Hypercoagulable workup, ANA/ENA (for CTD-associated PAH/ILD), PFTs, 6-minute walk test
- If ECHO confirms PAH with RV dysfunction, formal right heart catheterization and PAH specialist referral would be warranted
The MPA diameter of 33 mm and the mosaic attenuation pattern on CTPA are particularly important - these suggest this patient may have a pre-existing pulmonary vascular disease that the acute PE is now decompensating. The CTPA radiologist's recommendation for ECHO correlation is well-placed.
This is a shared conversation. Sign in to Orris to start your own chat.