Systemic vs local immune response
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough comparison of systemic vs. local immune responses, drawn from Cellular and Molecular Immunology, Robbins Pathologic Basis of Disease, and Yamada's Textbook of Gastroenterology.
Systemic vs. Local Immune Response
Overview
The immune system operates at two scales simultaneously. The local response is the initial, contained reaction at the precise site of infection or injury. The systemic response is the whole-body reaction driven by mediators that spill into the circulation, affecting remote organs.
1. Local Immune Response
What it is
The local response begins the moment a pathogen breaches a barrier. It involves cells already resident in the tissue - macrophages, mast cells, dendritic cells - plus those rapidly recruited from blood.
Key components and events
| Component | Role |
|---|---|
| Tissue macrophages & dendritic cells | First responders; phagocytose pathogens, release TNF, IL-1, IL-6 |
| Neutrophils (recruited) | Arrive within hours; primary phagocytes of acute local response |
| Mast cells | Release histamine and eicosanoids; cause vasodilation and increased permeability |
| Complement | Activated locally; opsonization and direct lysis |
| Endothelial activation | Upregulation of E/P-selectins and ICAM-1 - adhesion molecules that anchor circulating leukocytes |
The classical local signs - rubor, calor, tumor, dolor (redness, heat, swelling, pain) - all result from local vasodilation, plasma exudation, and nerve stimulation.
Local innate response timeline
The diagram below shows the sequence:
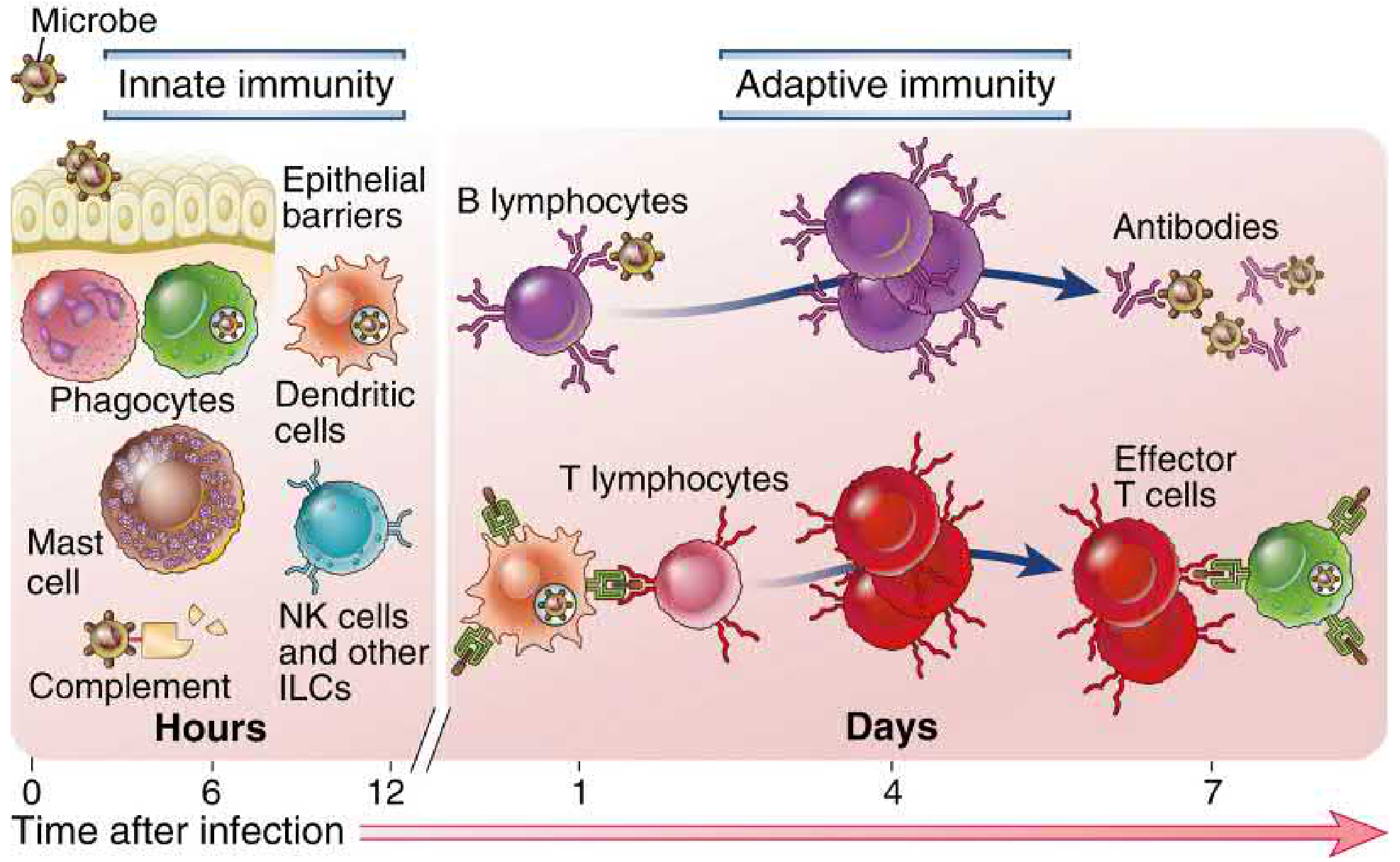
(Cellular and Molecular Immunology, 10e, Fig. 1.1)
- 0-12 hours: Innate cells (phagocytes, NK cells, complement) dominate locally
- Days 1-7: Adaptive response (T and B lymphocytes) amplifies and focuses the attack
Local adaptive response: mucosal immunity
A specialized form of local immunity exists at epithelial surfaces (gut, lung, urogenital tract). Its hallmark is secretory IgA (sIgA):
- Plasma cells in the lamina propria produce dimeric IgA linked by a J-chain
- Dimeric IgA binds the polymeric immunoglobulin receptor (pIgR) on epithelial cells and is transcytosed into the lumen
- Proteolytic cleavage releases secretory IgA - protected from luminal proteases by the secretory component
- sIgA does not activate complement, avoiding destructive inflammation at the mucosal surface
- Functions: blocks microbial adherence to epithelial cells, neutralizes toxins and intracellular pathogens, prevents antigen absorption
"The major function of secretory IgA in host defense is protection against bacteria, viruses, protozoa, and luminal antigens." - Yamada's Textbook of Gastroenterology, 7e
2. Systemic Immune Response
What it is
When local containment fails, or when the pathogen burden is large, cytokines (especially TNF, IL-1, IL-6) reach the bloodstream and trigger a coordinated whole-body response called the systemic acute-phase response.
Key components
Fever
- TNF and IL-1 act on the hypothalamus, stimulating prostaglandin E2 (PGE2) synthesis
- PGE2 raises the thermoregulatory set point - producing fever
- Fever enhances phagocyte activity and inhibits microbial replication
Leukocytosis
- TNF and IL-1 drive accelerated release of granulocytes from bone marrow
- WBC rises to 15,000-20,000 cells/mL (leukemoid reactions: up to 100,000 cells/mL)
- Pattern of leukocytosis reflects the pathogen:
- Bacteria - neutrophilia
- Viruses - lymphocytosis
- Parasites/allergy - eosinophilia
- A "shift to the left" (immature neutrophils in blood) indicates high demand from bone marrow
Acute-Phase Proteins (liver)
Stimulated by IL-6 (mainly) and TNF/IL-1, hepatocytes produce:
| Protein | Function |
|---|---|
| C-reactive protein (CRP) | Binds microbial cell walls; opsonin; activates complement |
| Fibrinogen | Causes rouleaux formation - basis of elevated ESR |
| Serum amyloid A (SAA) | Opsonin; prolonged elevation can cause secondary amyloidosis |
| Hepcidin | Sequesters iron from pathogens (but causes anemia of chronic disease) |
| Thrombopoietin | Increases platelet count (thrombocytosis) |
"Three of the best known of the proteins are C-reactive protein (CRP), fibrinogen, and serum amyloid A (SAA) protein. Synthesis of these molecules in hepatocytes is stimulated by cytokines, especially IL-6 (for CRP and fibrinogen) and IL-1 or TNF (for SAA)." - Robbins Pathologic Basis of Disease
Other systemic effects
- Increased heart rate and blood pressure
- Decreased sweating (blood redirected from skin to deep vessels to conserve heat)
- Muscle catabolism and negative nitrogen balance (mediated by TNF)
- Insulin resistance and hyperglycemia
When systemic response becomes dangerous: Septic Shock
In severe bacterial infections, massive cytokine release (a "cytokine storm") causes:
- Disseminated intravascular coagulation (DIC)
- Hypotensive shock (TNF dilates blood vessels, reduces cardiac contractility)
- Metabolic abnormalities (insulin resistance, hyperglycemia) This triad is septic shock / SIRS (systemic inflammatory response syndrome).
3. Head-to-Head Comparison
| Feature | Local Response | Systemic Response |
|---|---|---|
| Scope | Restricted to site of injury/infection | Whole body |
| Onset | Immediate (minutes to hours) | Hours to days after local response |
| Key cells | Macrophages, neutrophils, mast cells, local lymphocytes | Liver (hepatocytes), bone marrow, hypothalamus |
| Key mediators | Histamine, prostaglandins, local cytokines, complement | Circulating TNF, IL-1, IL-6; acute-phase proteins |
| Cardinal signs | Rubor, calor, tumor, dolor | Fever, leukocytosis, elevated CRP/ESR, tachycardia |
| Antibody type | sIgA at mucosal surfaces; local IgG/IgM | Circulating IgG, IgM (systemic humoral response) |
| Protective purpose | Contain and eliminate pathogen locally | Amplify defense, alert remote tissues, metabolic support |
| When it harms | Abscess, chronic granuloma, local tissue destruction | Septic shock, DIC, amyloidosis, anemia of chronic disease |
4. The Bridge: How Local Becomes Systemic
The transition happens when cytokines overwhelm local containment:
- Resident macrophages and dendritic cells at infection site release TNF, IL-1, IL-6
- At low concentrations - purely local effects (adhesion molecules, local recruitment)
- At higher concentrations - cytokines spill into bloodstream
- They reach the hypothalamus (fever), liver (acute-phase proteins), and bone marrow (leukocytosis)
- If massively elevated (e.g., gram-negative sepsis) - vascular collapse and SIRS
This gradient from local to systemic is not a sharp boundary but a continuum driven by pathogen burden and host response intensity.
Sources:
- Cellular and Molecular Immunology, 10e (Abbas et al.)
- Robbins & Kumar Pathologic Basis of Disease (Robbins Pathology)
- Yamada's Textbook of Gastroenterology, 7e
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.