Cabg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"coronary artery bypass" AND revascularization
I now have comprehensive data from multiple authoritative textbooks. Here is the full structured overview of CABG:
Coronary Artery Bypass Grafting (CABG)
Definition
CABG is a cardiac surgical procedure that restores myocardial blood flow by creating a new conduit (graft) that routes blood around an obstructed coronary artery, anastomosing it distal to the stenotic lesion. The internal mammary artery (IMA) or radial artery is anastomosed directly to the coronary artery, while venous conduits (saphenous vein) are connected proximally to the aorta and distally to the target vessel.
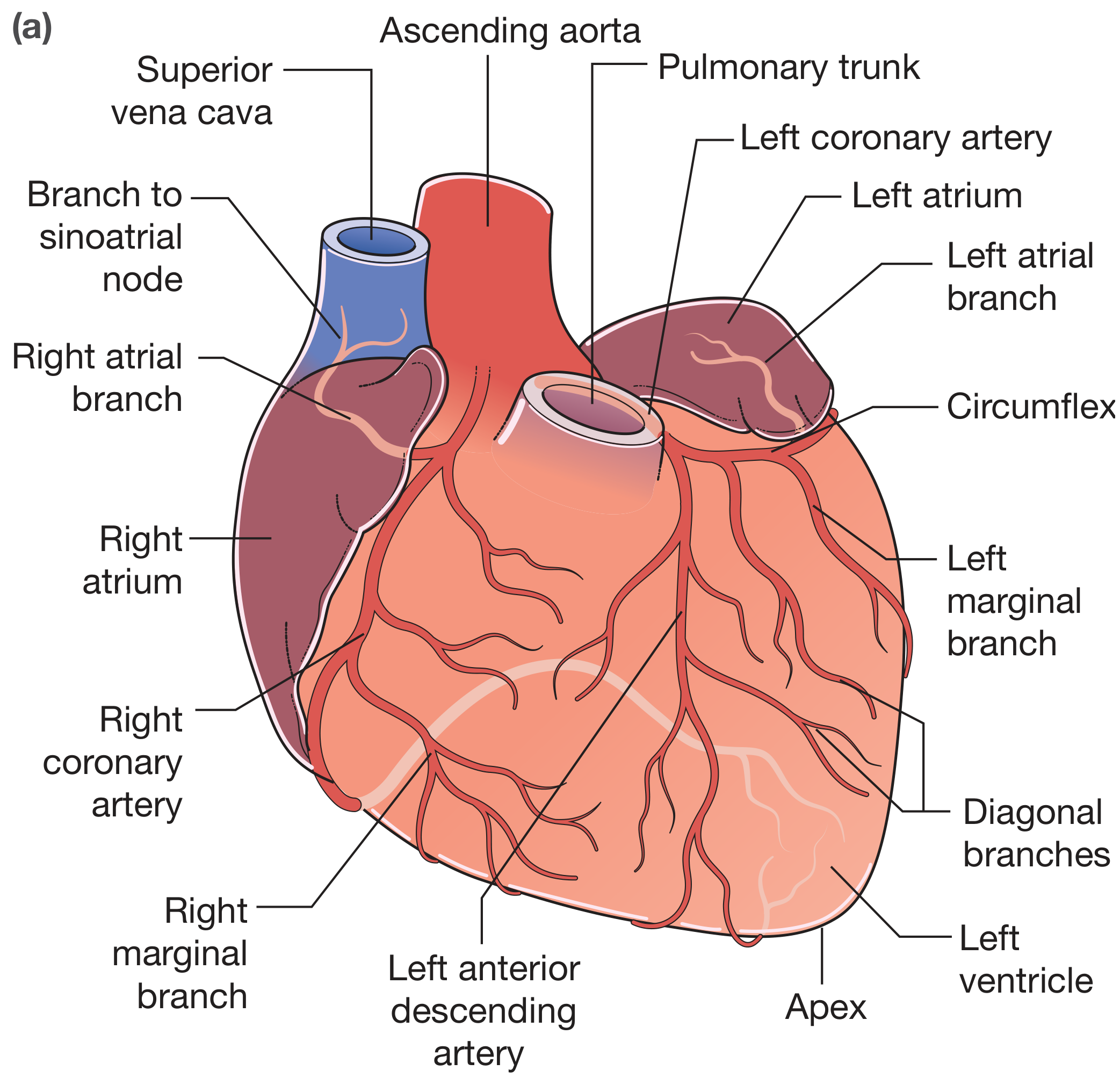
Coronary Anatomy Relevant to CABG
| Vessel | Territory | Common Disease Site |
|---|---|---|
| Left main (LMCA) | LAD + circumflex distribution | Origin |
| LAD (left anterior descending) | Anterior LV, septum | Proximal segment - most frequently bypassed |
| Circumflex (Cx) | Lateral LV wall, obtuse marginals | Mid-vessel |
| RCA | RV free wall, inferior LV | Proximal segment, crux |
- Right dominance (~90%): PDA arises from RCA
- Left dominance (~10%): PDA arises from circumflex
- Co-dominance (~5%): dual posterior descending arteries
Indications for CABG
Based on the 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization:
Class I (Benefit >>> Risk)
- Left main stenosis >50%
- Three-vessel disease (especially with reduced LVEF)
- Two-vessel disease including proximal LAD
- Multivessel disease with diabetes mellitus (CABG superior to PCI)
- Multivessel disease with LVEF <35% - survival benefit
Class IIa (Benefit >> Risk)
- Previous CABG with refractory angina due to LAD disease (when IMA can be used)
- Patients unable to tolerate/adhere to DAPT (dual antiplatelet therapy)
- Symptomatic recurrent diffuse in-stent restenosis (ISR)
Symptomatic Indications
- Troublesome angina inadequately controlled by optimal medical therapy
- Patients desiring an active life with severe stenoses and objective evidence of ischemia
Note: CABG is superior to PCI in patients with diabetes + multivessel disease, complex anatomy (high SYNTAX score), left main disease, and those needing concurrent cardiac surgery (e.g., valve repair).
Preoperative Workup
Investigations
| Test | Purpose |
|---|---|
| 12-lead ECG | Baseline; Q waves = prior MI |
| Cardiac troponin / CK-MB | ACS assessment |
| Echocardiography (TTE/TEE) | LVEF, regional wall motion, valvular disease |
| Stress echo or nuclear perfusion | Myocardial viability, ischemic burden |
| Coronary angiography (gold standard) | Extent, severity, location of stenoses; assesses distal tree quality |
| CT coronary angiography | Non-invasive alternative; 89-95% sensitivity |
| Cardiac MRA | Volumetric LVEF, viability (gold standard for LV volumes) |
| Carotid duplex / peripheral vascular exam | Comorbid atherosclerosis assessment |
Risk Stratification
- EuroSCORE II (most common in UK)
- STS PROM score (US standard) - incorporates age, sex, LVEF, diabetes, PVD, renal disease, prior CABG
Pre-op Medication Management
- Stop: antiplatelet agents (aspirin - hold 5 days), anticoagulants, oral hypoglycaemics
- Continue: cardiac medications, antihypertensives preoperatively
- Heart team discussion (surgeon + interventional cardiologist + non-interventional cardiologist) is Class I recommendation
Conduit Selection
Arterial Grafts (preferred)
| Conduit | Notes |
|---|---|
| LIMA (left internal mammary/thoracic artery) | Gold standard - 10-year patency >95%; anastomosed to LAD; reduces reoperation rate; STS quality measure |
| RIMA (right IMA) | Class IIa recommendation; bilateral IMA (BIMA) improves survival; caution in diabetics/obese (sternal wound infection risk); skeletonization reduces this risk |
| Radial artery (RA) | Class I recommendation over SVG for non-LAD targets; Allen's test required preoperatively; excellent 1- and 5-year patency |
Venous Grafts
| Conduit | Notes |
|---|---|
| Long saphenous vein (SVG) | Most common; easy harvest; patency 50-60% at 10 years; improved with aspirin + statins postoperatively |
| Short saphenous vein, cephalic vein | Alternative; poorer patency |
SVG graft occlusion: 10-20% in year 1, ~2%/year at 5-7 years, ~4%/year thereafter
Surgical Technique
On-Pump CABG (Conventional)
- Median sternotomy
- Heparinization
- Cardiopulmonary bypass (CPB) established - aortic cannula + venous return cannulas
- Aortic cross-clamping + cardioplegia (cold/warm) to arrest and protect the heart
- Distal anastomoses performed on the arrested, bloodless heart (end-to-side or side-to-side with running polypropylene suture)
- Proximal anastomoses to the ascending aorta (or sequential/Y-graft configurations)
- De-air, release cross-clamp, reperfusion
- Wean from CPB; heparin reversal with protamine
- Epicardial pacing wires placed
- Transfer to ICU
Off-Pump CABG (OPCAB)
- Performed on the beating heart using mechanical stabilizers
- Avoids CPB-related complications (microembolism, coagulopathy, inflammatory response)
- Used in select high-risk patients (renal disease, severe atherosclerotic aorta)
- No significant difference in neurocognitive outcomes vs. on-pump
Minimally Invasive Options
| Approach | Description |
|---|---|
| MIDCAB (Minimally Invasive Direct CABG) | Small left thoracotomy; LIMA to LAD only; no CPB |
| TECAB (Totally Endoscopic CABG) | Robotic; multi-vessel possible; recent meta-analysis shows comparable outcomes |
| Hybrid CABG | CABG for LIMA-LAD + PCI for other vessels |
CPB Complications
- Coagulopathy
- Air embolism
- Microembolization (brain, eyes)
- Myocardial depression
- Neurological dysfunction
- Postcardiotomy syndrome (Dressler's-like)
- Pulmonary injury
- GI complications (bowel/liver ischemia, pancreatitis)
- Systemic organ dysfunction
Outcomes
| Metric | Data |
|---|---|
| Operative mortality (low-risk) | <1% |
| Angina relief | ~90% of patients after complete revascularization |
| SVG patency at 10 years | 50-60% |
| LIMA patency at 10 years | >95% |
| Survival benefit (LMS or 3-VD with low LVEF) | Clearly demonstrated |
| CABG vs. PCI in DM | CABG superior - fewer deaths, MIs, repeat revascularizations |
Higher risk is associated with: LV dysfunction, advanced age (≥80), reoperation, emergency surgery, diabetes mellitus.
Postoperative Management
ICU Phase
- Most patients extubated within a few hours
- ICU stay ~24 hours; discharge 4-8 days
Early Complications
| Complication | Notes |
|---|---|
| Atrial fibrillation | Most common arrhythmia; 30-60% post-CABG; treat with K+ >4.5 mmol/L, beta-blockers, amiodarone, cardioversion |
| Bleeding | 2-3%; cardiac tamponade requires emergency resternotomy |
| Low cardiac output | Inotropes (dobutamine), IABP, optimize preload/afterload |
| Wound infection (sternal) | Higher with BIMA, obesity, diabetes |
| Neurocognitive dysfunction | Embolic/inflammatory; higher in on-pump |
| Renal failure | Especially in pre-existing CKD |
Long-term Medical Therapy (Guideline-Directed)
- Aspirin: continue indefinitely (antiplatelet, improves SVG patency)
- Statins: mandatory - improve graft patency, reduce risk factor progression
- Beta-blockers: post-revascularization
- Cardiac rehabilitation: structured exercise + risk factor modification
- Psychosocial care: depression screening post-CABG
Special Populations
| Population | Consideration |
|---|---|
| Diabetes | CABG clearly superior to PCI; insulin-sensitizing strategy best |
| Females | Higher short-term mortality; smaller vessel size |
| Renal disease | Increased perioperative risk; off-pump preferred |
| Elderly (≥70-80 yrs) | Higher mortality; careful case selection |
| Obese | Avoid BIMA (sternal infection); skeletonization if BIMA needed |
| Pregnancy | Rare; high maternal/fetal risk |
CABG vs. PCI - Key Points
| Factor | Favors CABG | Favors PCI |
|---|---|---|
| Anatomy | Left main, 3-VD, high SYNTAX score | 1-2 VD, low SYNTAX, simple lesions |
| Diabetes | Clear benefit | Less durable |
| LVEF | Depressed EF benefits more from CABG | - |
| DAPT intolerance | CABG avoids stent thrombosis risk | - |
| Reoperation risk | Lower long-term repeat revascularization | Higher repeat revasc |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), p. 575-612
- Sabiston Textbook of Surgery, p. 2480-2560
- Bailey & Love's Short Practice of Surgery 28th Ed., p. 968-975
- 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization (cited throughout)
Recent evidence (2024-2025):
- Frailty significantly worsens CABG outcomes [PMID: 39725933]
- Totally endoscopic CABG (TECAB) shows comparable outcomes to conventional CABG in meta-analysis [PMID: 39567250]
This is a shared conversation. Sign in to Orris to start your own chat.