Brachial plexus and it's injuries
Reading File
Finding Sources
Searching PubMed
"brachial plexus injury" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Brachial Plexus and Its Injuries
Anatomy of the Brachial Plexus
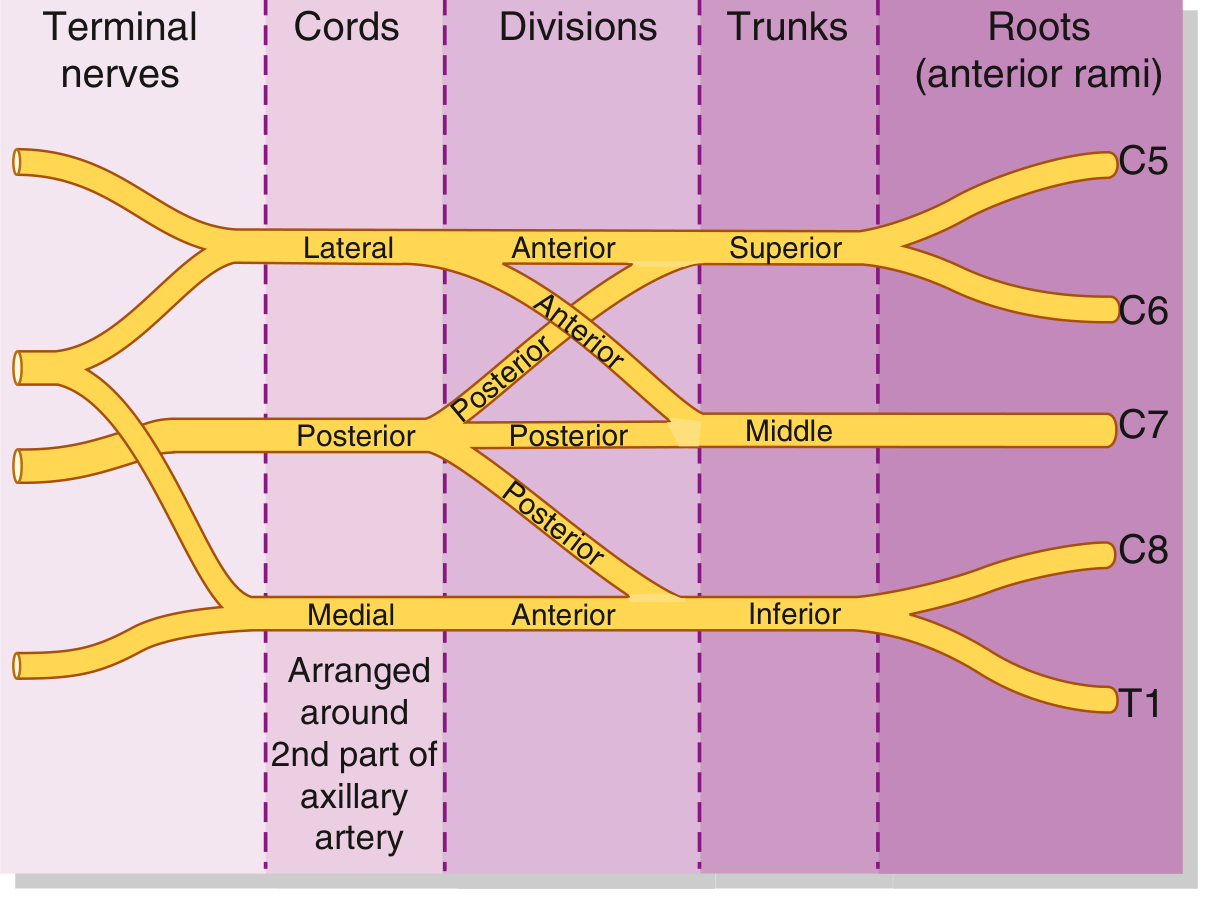
The brachial plexus is a somatic nerve network formed by the anterior rami of C5, C6, C7, C8, and T1. It originates in the neck between the anterior and middle scalene muscles, crosses rib I, and enters the axilla, where its cords surround the axillary artery.
Memory aid: "Robert Taylor Drinks Cold Beer" - Roots, Trunks, Divisions, Cords, Branches
Anatomical diagram (Gray's Anatomy for Students)

Schematic: Roots → Trunks → Divisions → Cords
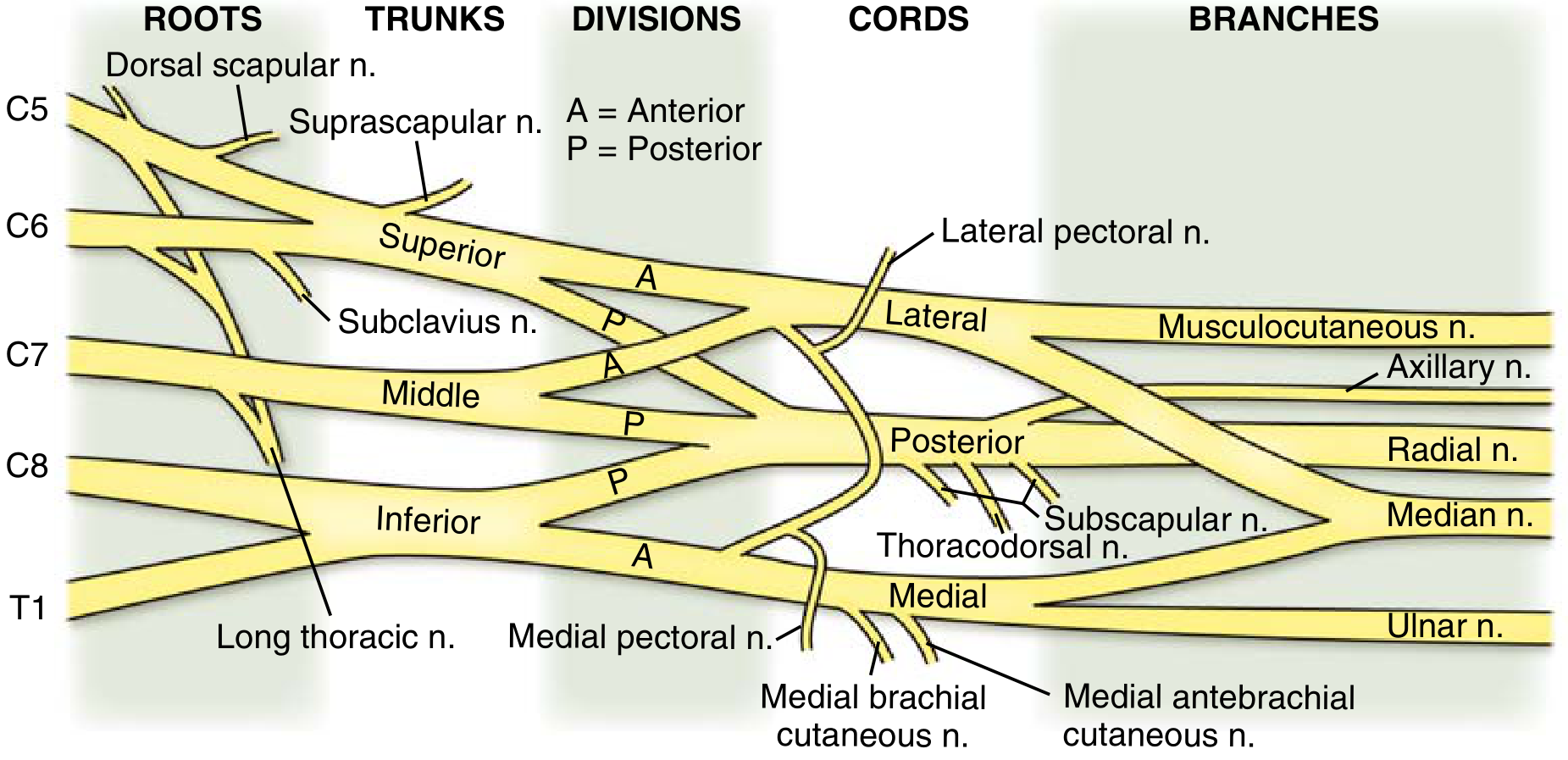
Full plexus with named branches (Miller's Orthopaedics)
Components
| Level | Details |
|---|---|
| Roots | Anterior rami of C5-T1; receive gray rami communicantes (postganglionic sympathetic) |
| Trunks | Superior (C5+C6), Middle (C7), Inferior (C8+T1); pass laterally over rib I |
| Divisions | Each trunk divides into anterior + posterior (6 divisions total); anterior = flexor compartments, posterior = extensor compartments |
| Cords | Named by relation to axillary artery: Lateral cord (anterior divisions of superior + middle trunks), Medial cord (anterior division of inferior trunk), Posterior cord (all three posterior divisions) |
| Branches (terminal) | Musculocutaneous (lateral cord), Axillary (posterior cord), Radial (posterior cord), Median (lateral + medial cords), Ulnar (medial cord) |
Pre-terminal branches (from roots/trunks)
- Dorsal scapular nerve (C5) - rhomboids
- Long thoracic nerve (C5-7) - serratus anterior
- Nerve to subclavius (C5-6)
- Suprascapular nerve (C5-6, from superior trunk) - supraspinatus + infraspinatus
Classification of Nerve Injuries
Seddon's Classification (1943) - 3 types
| Type | Features | Prognosis |
|---|---|---|
| Neuropraxia | Focal demyelination; axon intact; conduction block | Full recovery; weeks to months |
| Axonotmesis | Axonal continuity lost; endoneurium ± perineurium intact | Variable; slow (1 mm/day) but possible spontaneous recovery |
| Neurotmesis | Complete nerve transection; all layers disrupted including epineurium | No recovery without surgery |
Sunderland's Classification (5 degrees)
| Degree | Structural Damage | Seddon Equivalent |
|---|---|---|
| 1st | Focal demyelination only | Neuropraxia |
| 2nd | Axon lost; endoneurium intact | Axonotmesis |
| 3rd | Axon + endoneurium lost; perineurium intact | Axonotmesis |
| 4th | Axon + endoneurium + perineurium lost; epineurium intact | Axonotmesis |
| 5th | All structures disrupted | Neurotmesis |
| 6th | Mixed injury (Mackinnon-Dellon modification) | Mixed |
- Sabiston Textbook of Surgery, Table 41.5
Types of Brachial Plexus Injuries
By Level
1. Upper Trunk Injury - Erb's Palsy (C5-C6)
- Mechanism: Forced depression of the shoulder (traction away from neck); most common in neonates with shoulder dystocia; also motorcycle accidents
- Clinical features:
- Arm hangs at side, internally rotated, elbow extended, forearm pronated - the classic "waiter's tip" or "bellhop's tip" posture
- Deltoid, biceps, brachialis, brachioradialis paralyzed
- Loss of shoulder abduction/external rotation, elbow flexion, forearm supination
- Absent biceps reflex
- Hand movements preserved
- Most common brachial plexus injury (~20x more frequent than Klumpke's)
2. Lower Trunk Injury - Klumpke's Palsy (C8-T1)
- Mechanism: Forced extension/abduction of the arm over the head
- Clinical features:
- Claw hand deformity - intrinsic hand muscle paralysis (interossei + lumbricals)
- Absent grasp reflex
- If T1 sympathetic fibers involved: Horner syndrome (ptosis, miosis, anhidrosis, enophthalmos)
- Weakness similar to ulnar nerve injury
- Rare in clinical practice
3. Complete Plexus Injury (C5-T1)
- Flail, anesthetic arm
- Rarest pattern; most severe
- Often associated with root avulsions
By Injury Type
| Type | Features |
|---|---|
| Root avulsion | Most severe; proximal to dorsal root ganglion (preganglionic); no hope of spontaneous recovery; Horner sign if C8-T1; histamine test positive (skin flare intact) |
| Rupture | Continuity broken but root not avulsed; can be grafted |
| Stretch/traction | Most common adult mechanism; varies from neuropraxia to rupture |
| Compression | Pancoast tumor, cervical rib, hematoma, thoracic outlet |
| Penetrating | Knife wounds (common in brachial plexus), bullet wounds (poor prognosis) |
Special Patterns
- Obstetric brachial plexus palsy: Large newborns with shoulder dystocia; upper plexus (Erb) most common; may be associated with diaphragmatic paralysis (C3-5), Horner syndrome, fractured clavicle/humerus
- Radiation plexopathy: Progressive painless weakness post-radiotherapy; myokymia on EMG; must differentiate from neoplastic infiltration (which is painful)
- Thoracic outlet syndrome: Lower trunk compression; weakness of intrinsic hand muscles; mainly ulnar sensory loss; cervical rib possible
- Pancoast tumor: Apical lung tumor compressing lower trunk (C8-T1) + sympathetics = arm pain + Horner syndrome
Assessment
Clinical
- Document sensory + motor deficits precisely
- Test biceps reflex (C5-6), triceps reflex (C7), finger reflexes
- Moro reflex asymmetry in neonates
- Progressive deficits suggest expanding hematoma - consider early exploration
Investigations
- EMG/NCS: Do at 3-6 weeks post-injury (Wallerian degeneration needs time; before 3 weeks results are uninformative)
- Myokymia on EMG suggests radiation plexopathy
- MRI/CT: Rule out disc herniation, spondylosis, subluxation, tumor infiltration; identify root avulsion
- Plain X-ray: Exclude skeletal injury (clavicle fracture, etc.)
- In neonates: electrodiagnostic tests technically difficult; serial examinations more practical
Prognosis
- Neonatal Erb's palsy: Evidence of recovery within 2-4 weeks = good prognosis for full recovery; ~75% recover fully; biceps function is the key prognostic indicator
- ~25% of birth palsies have persistent deficits
- Rate of nerve regeneration: ~1 mm/day (3 mm/month)
- Root avulsions have the worst prognosis
Management
Conservative
- All injury types: Occupational and physiotherapy at a multidisciplinary center by 1 month of age (neonates)
- Early range-of-motion exercises
- Splinting to prevent contractures
- Serial examinations to track recovery
Surgical Indications
- Adults: No functional improvement after 3 months of conservative management
- Neonates: No evidence of spontaneous recovery at 3 months
- Progressive deficit (expanding hematoma) - early surgical exploration
- Clean, sharp injuries - may benefit from early primary repair
Surgical Options
| Procedure | Indication |
|---|---|
| Primary neurorrhaphy (end-to-end repair) | Clean lacerations, no tension |
| Nerve grafting | Bridging a gap after resection of damaged segment; sural nerve commonly harvested (pure sensory, minimal donor morbidity) |
| Nerve transfer (neurotization) | Root avulsions where proximal stump unavailable; e.g., intercostal nerves → musculocutaneous nerve to restore elbow flexion; spinal accessory → suprascapular nerve; ulnar/median fascicles → biceps (Oberlin transfer) |
| Tendon transfers | Late reconstruction |
| Arthroscopic/open joint release | Shoulder contracture in birth palsy |
| Derotational humeral osteotomy | Internal rotation contracture in Erb's palsy |
Intraoperative principle: If electrical testing shows conduction across the injury, continue observation. No conduction = resect and repair/graft.
A 2025 systematic review and meta-analysis (PMID: 40856835) compared nerve transfer options for elbow flexion restoration in brachial plexus injury, finding ulnar/median fascicle transfers competitive with intercostal nerve transfers. Another 2025 systematic review (PMID: 40988532) examined management of brachial plexus injuries after shoulder dislocation.
Summary Table: Clinical Syndromes at a Glance
| Syndrome | Roots | Posture/Signs | Common Cause |
|---|---|---|---|
| Erb's palsy | C5-C6 | "Waiter's tip"; no elbow flexion, arm internally rotated | Shoulder dystocia, motorcycle crash |
| Klumpke's palsy | C8-T1 | Claw hand + Horner syndrome | Arm abducted/forced over head |
| Complete palsy | C5-T1 | Flail, anesthetic arm | Severe traction injury |
| Thoracic outlet syndrome | Lower trunk | Intrinsic hand weakness + ulnar sensory loss | Cervical rib, postural compression |
| Pancoast syndrome | C8-T1 + sympathetics | Hand weakness + Horner + shoulder pain | Apical lung tumor |
Sources: Gray's Anatomy for Students (8e); Miller's Review of Orthopaedics (9e); Campbell's Operative Orthopaedics (15e, 2026); Schwartz's Principles of Surgery (11e); Sabiston Textbook of Surgery; Bradley and Daroff's Neurology in Clinical Practice; Adams and Victor's Principles of Neurology (12e)
This is a shared conversation. Sign in to Orris to start your own chat.