Explain surgery endoscopic Septoplasty
Reading File
Finding Sources
Finding Sources
Searching PubMed
endoscopic septoplasty technique outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile a thorough answer.
Endoscopic Septoplasty
Overview
Endoscopic septoplasty is a minimally invasive technique for correcting nasal septal deviations under direct endoscopic visualization, introduced by Giles and colleagues in 1994. It uses a rigid nasal endoscope (typically 0-degree or 30-degree) in place of, or in combination with, the traditional headlamp and nasal speculum, offering superior illumination and magnification - especially of posterior septal structures.
The name "septoplasty" derives from the Greek term meaning "to reshape or mold the septum." The goal is to maximize relief of nasal obstructive symptoms while preserving the structural integrity of the septum.
Indications
Endoscopic septoplasty is best suited for:
- Limited or focal septal deviations (not complex multi-level deformities)
- Isolated septal spurs, especially posterior spurs
- Concurrent endoscopic sinus surgery (ESS) - when a septal deviation obstructs access to the middle meatus or makes postoperative debridement difficult
- Patients where minimal mucosal dissection is preferred
It is less suitable for:
-
Caudal end deflections
-
Nasal spine prominence or maxillary crest irregularities
-
High dorsal deflections
-
Septal fractures
-
Complex deviations requiring wide mucoperichondrial flap elevation
-
Cummings Otolaryngology Head and Neck Surgery
Preoperative Preparation & Anesthesia
Before incision, topical and local vasoconstriction/analgesia is essential for:
- A dry operative field enabling careful dissection
- Analgesic effect
Topical agents used:
- 4% cocaine solution on cotton pledgets (2-4 mL in adults), or
- Oxymetazoline
Infiltrative anesthetic: 1% lidocaine (xylocaine) with 1:100,000 epinephrine (max 4-7 mg/kg). Preoperative IV fentanyl and midazolam (versed) stabilize cardiac and smooth muscle and counteract potential tachycardia/hypertension from vasoconstrictors.
Systemic toxicity from local anesthetics manifests as pupillary constriction, hypotension, vomiting, and cardiac or respiratory arrest - requiring 100% O2, vasopressors, and ventilatory support.
- Cummings Otolaryngology Head and Neck Surgery, p. 572
Surgical Technique
There are two main approaches to endoscopic septoplasty:
1. "Direct" Endoscopic Septoplasty (Fully Endoscopic)
This is used for focal deviations and spurs and is particularly convenient when combined with ESS:
| Step | Description |
|---|---|
| Incision | A small mucosal incision is made just anterior to the focal deviation or spur |
| Flap elevation | Bilateral submucoperichondrial (over cartilage) and submucoperiosteal (over bone) flaps are elevated circumferentially around the deviation |
| Resection | The offending deviated cartilage or bony spur is removed under direct endoscopic view |
| Closure | With small incisions, no sutures are typically needed; the mucosal flap is laid back down |
Key advantage: the endoscope gives excellent visualization of posterior structures that are difficult to see with a traditional headlamp.
2. "Assisted" Endoscopic Septoplasty
This hybrid approach uses:
- A conventional hemitransfixion incision (made with headlamp guidance)
- Once a ~1 cm submucoperichondrial flap has been elevated, the 0-degree endoscope is inserted to guide further dissection
A suction Freer elevator is especially useful here - it allows simultaneous irrigation/suction and dissection under endoscopic guidance. Dissection then proceeds as in conventional septoplasty but with the endoscope providing superior posterior visualization.
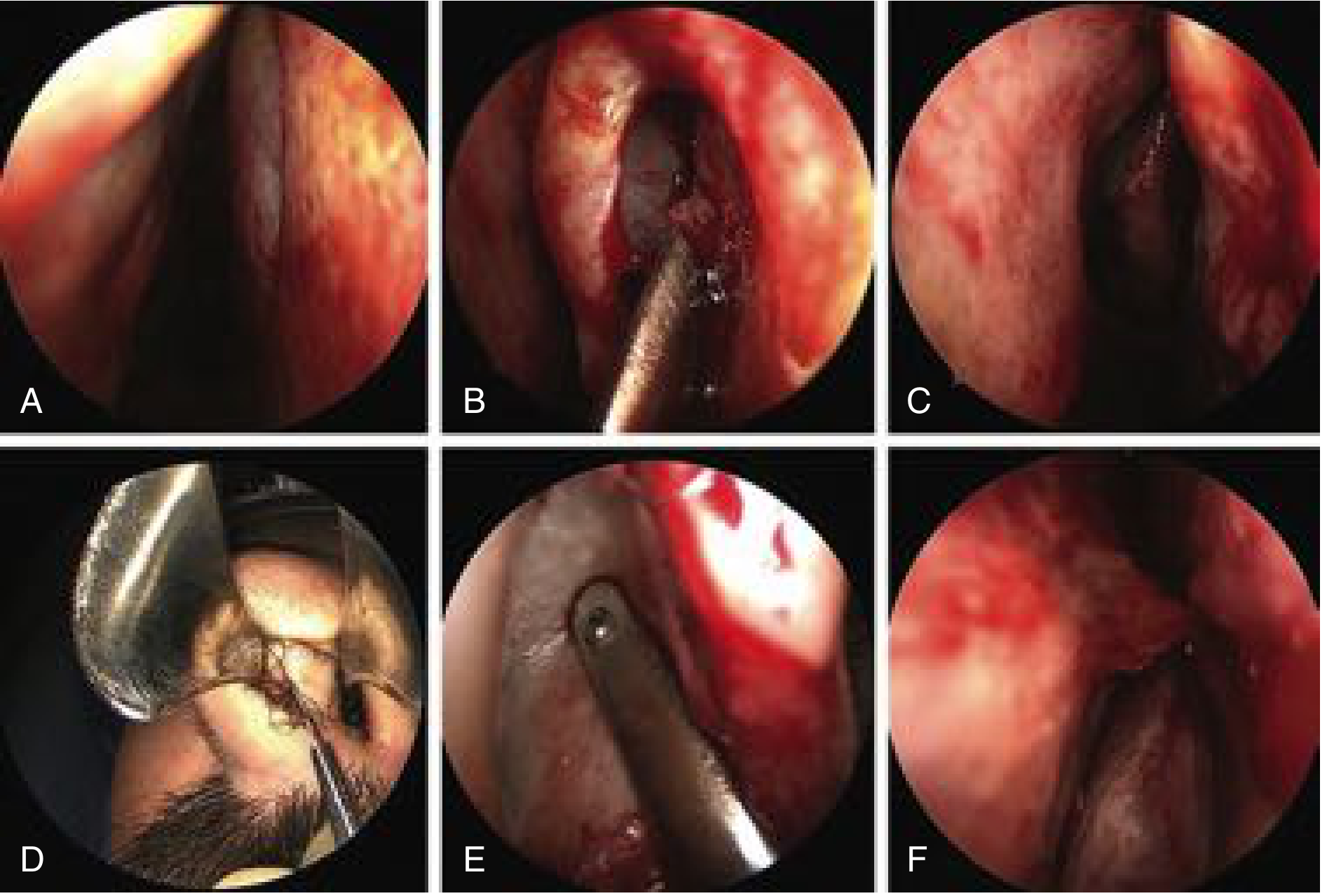
Fig. 44.25 - Endoscopic "direct" septoplasty (A-C) and "assisted" septoplasty (D-F). (Cummings Otolaryngology, p. 891)
Key Surgical Principles
- Mucosal preservation is the primary goal - a submucous approach protects the mucoperichondrial envelope
- Avoid contiguous bilateral mucosal tears (opposite sides of the septum) - these lead to septal perforation
- Any mucosal fenestrations, even unilateral ones, should be closed with 5-0 plain suture at the time of surgery
- If mucosal flaps are weakened, crushed cartilage grafts are interposed within the envelope to prevent perforation, support the membrane, and facilitate re-entry if revision is needed
- The septum is re-quilted with a continuous 5-0 plain mattress suture (using a curved needle, not a straight Keith needle, to avoid turbinate injury and synechiae)
Endoscopic Septoplasty vs. Conventional Septoplasty
| Feature | Endoscopic | Conventional |
|---|---|---|
| Visualization | Superior (esp. posterior) | Good anteriorly, limited posteriorly |
| Incision size | Smaller | Larger hemitransfixion/Killian |
| Sutures needed | Often none | Usually required |
| Best for | Focal deviations, spurs, combined with ESS | Complex/multi-level deformities |
| Mucosal flap elevation | Limited (circumferential around deviation only) | Wide bilateral elevation |
| Teaching value | High (shared screen visualization) | Standard |
| Outcomes (RCT data) | No significant difference vs. conventional for limited deviations (Bothra & Mathur, 80 patients) | Comparable |
Combined with Endoscopic Sinus Surgery (ESS)
This is one of the most common indications. A significant septal deviation can:
- Cause lateral displacement of the middle turbinate, obstructing the ostiomeatal complex (OMC)
- Make ESS technically difficult or impossible
- Impede postoperative endoscopic debridement
The recommended sequence: perform ESS on the side with adequate access first, then perform septoplasty and continue on the obstructed side.
Asymptomatic deviations may still warrant correction if they interfere with ESS access or postoperative care.
Postoperative Care
- Nasal packs (if used) are removed early; after removal, saline nasal flushing 4x/day is started
- Antibiotic ointment instilled into each vestibule beginning 24 hours postoperatively
- Gentle suctioning on postoperative days 5-10
- Gentle nose blowing permitted after week 3
- Strenuous exercise avoided for 6 weeks
- Internal nasal splints are used selectively (septal perforation repair, excoriated membrane) - soft silastic splints (0.02-inch) are preferred over hard commercial splints
Complications
| Complication | Cause |
|---|---|
| Persistent nasal obstruction | Most common; often due to inadequate addressing of posterior bony septum/spurs |
| Septal hematoma | Failure to use quilting mattress suture |
| Septal perforation | Bilateral contiguous mucosal tears, failure to reskeletonize the envelope |
| Nasal shape changes (tip ptosis, saddle deformity) | Overresection of caudal septum or dorsal support loss |
| Infection | Rare |
| Synechiae (adhesions) | Traumatic suturing technique, especially with straight needles |
| Rhinorrhea | May persist for months postoperatively |
- Cummings Otolaryngology Head and Neck Surgery, p. 582
Summary
Endoscopic septoplasty is an effective, minimally invasive alternative or adjunct to conventional septoplasty, ideally suited for focal deviations and septal spurs - especially when combined with ESS. Its main advantages are superior visualization of the posterior nasal cavity, smaller incisions, and reduced mucosal disruption. For complex or multi-level deformities, conventional open septoplasty still provides wider access and remains the preferred approach.
A recent 2024 meta-analysis (PMID: 39572690) confirmed that septoplasty - endoscopic or conventional - significantly benefits patients with deviated nasal septum, including those with concurrent allergic rhinitis, supporting its use even in this subgroup.
What is VC polyps and explain MLS for vc polyp
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
vocal fold polyp microlaryngoscopy surgery treatment
Reading File
Loading Image
Loading Image
I now have comprehensive information. Here is the full answer:
Vocal Cord (Vocal Fold) Polyps
Definition
A vocal cord (VC) polyp - more precisely called a vocal fold polyp - is a fibrovascular, subepithelial lesion arising from the mid-membranous portion of the true vocal fold (free vibratory edge). It is a benign, non-neoplastic growth that develops within Reinke's space (the superficial lamina propria).
Anatomy Recap
The vocal fold has five layers:
- Epithelium (squamous)
- Reinke's space (superficial lamina propria) - where polyps arise
- Intermediate lamina propria
- Deep lamina propria
- Vocalis muscle
Polyps displace and distort this layered microarchitecture, impairing mucosal wave vibration and causing dysphonia.
Etiology & Pathophysiology
| Factor | Details |
|---|---|
| Voice abuse/misuse | Most common trigger - repeated phonotrauma causes capillary rupture in Reinke's space |
| Resolving hematoma | A hemorrhagic polyp often begins as a blood blister after sudden vocal strain (shearing forces rupture submucosal capillaries) |
| Capillary ectasia | Predisposes to vascular injury with vocal exertion |
| Cigarette smoking | Associated with polyp formation, especially in combination with vocal abuse |
| Acute infective episode | Can trigger polyp development |
| Acid reflux (GERD) | Dilates capillaries and increases hyperemia; promotes development |
Epidemiology: More common in men, particularly those who engage in intermittent severe voice abuse or who work in noisy environments.
Types of VC Polyps
1. Hemorrhagic (Vascular) Polyp
- Arises from rupture of a deeper capillary - blood accumulates focally like a blood blister
- Appears dark red/purple in early stages
- Alters vocal fold margin contour and stiffens mucosa (seen stroboscopically)
- Classic history: abrupt onset hoarseness during extreme vocal effort (shouting at a party, sporting event, loud sneeze)
- May re-bleed intermittently; discoloration evolves through bruise stages
2. Pedunculated (End-Stage) Polyp
- Long-standing hemorrhagic polyp loses its vascular appearance and becomes pale, gelatinous, pedunculated
- May move in and out of the glottis with respiration
- During phonation, may be displaced upward onto the fold's superior surface
- Large pedunculated polyps can cause dyspnea and airway obstruction (ball-valve effect)
3. Sessile (Broad-Based) Polyp
- Attached to the fold by a broad base rather than a narrow pedicle
- Contains unorganized gelatinous debris in the subepithelial space
Clinical Features
Primary symptom: Dysphonia (hoarseness)
- Chronic vocal huskiness
- Intermittent aberrant vocal sounds
- Impaired or absent falsetto register
- Large polyps may cause dyspnea, respiratory stridor, or ball-valve airway obstruction
- Sudden enlargement if bleeding occurs into the polyp
Contact reaction: A nodule or contact reaction may appear on the contralateral fold at the area opposing the polyp (due to repeated mechanical trauma).
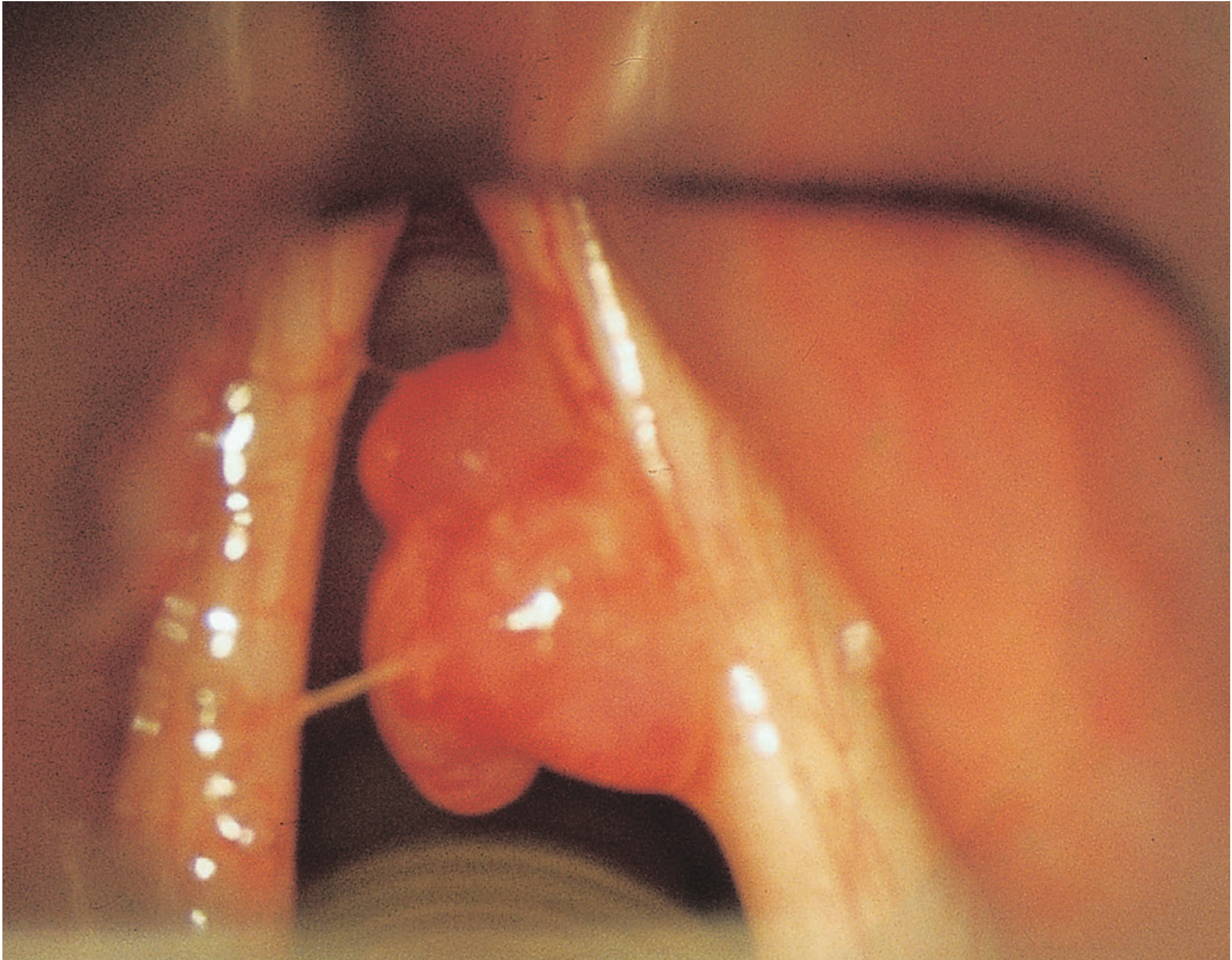
Vocal fold polyp as seen at laryngoscopy (Bailey and Love's Short Practice of Surgery)
Diagnosis
1. History
- Voice abuse history, smoking, reflux, abrupt onset of hoarseness with exertion
2. Laryngoscopy / Office Endoscopy
- Subepithelial mass, broad-based or pedunculated
- Normal overlying epithelium (distinguishes from malignancy)
- Can be translucent (pale/gelatinous) or hemorrhagic (dark/blood-filled)
3. Videostroboscopy
- Preserved mucosal wave (key finding distinguishing polyp from scar or sulcus)
- Stiffness of the fold at the polyp site
- Size, turgidity, and pedunculation affect vocal capabilities
Treatment Overview
| Approach | Details |
|---|---|
| Medical | Stop NSAIDs/anticoagulants; treat GERD with PPIs |
| Voice therapy | Short course; useful for voice care education; polyps do not regress with therapy alone, but voice may improve |
| Surgery (MLS) | Definitive treatment - excision via microlaryngoscopy (see below) |
| KTP Laser (532 nm) | In-office or via microlaryngoscopy; useful for vascular polyps |
Unlike nodules, vocal fold polyps do not resolve with voice therapy alone and typically require surgical removal. - K.J. Lee's Essential Otolaryngology
Microlaryngoscopy Surgery (MLS) for Vocal Cord Polyp
What is MLS?
Microlaryngoscopy (MLS), also called suspension microlaryngoscopy or direct laryngoscopy with microscope, is the gold standard operative technique for surgical removal of benign vocal fold lesions including polyps. It provides:
- Binocular magnification via the operating microscope
- Direct bimanual access to both vocal folds
- A hands-free operative field
Setup and Positioning
| Element | Detail |
|---|---|
| Patient position | Supine, neck extended ("sniffing position") |
| Laryngoscope | Rigid direct laryngoscope (e.g., Dedo laryngoscope, Hollinger laryngoscope for difficult airways) introduced transorally |
| Suspension | The laryngoscope is suspended on a chest support/Mayo stand apparatus - this frees both hands of the surgeon |
| Microscope | Operating microscope positioned over the laryngoscope for 6-25x magnification |
| Anesthesia | General anesthesia with orotracheal intubation (small tube, e.g., 5.0-6.0 mm microlaryngoscopy tube), jet ventilation, or controlled intermittent apnea |
Key step: Care is taken not to place unnecessary tension at the anterior commissure, which would distort the vocal folds and lead to inaccurate excision.
The false vocal fold is lateralized with a spatula to expose the laryngeal ventricle and true vocal fold.
Instruments Used
- Microlaryngoscopy forceps - various angles (right-turning, left-turning, heart-shaped, alligator) for grasping and mobilizing the polyp
- Microsurgical scissors - for cold-instrument excision
- Suction Freer elevator - for submucosal dissection
- Microsurgical cup forceps - to remove tissue fragments
- Cocaine-soaked pledgets - for hemostasis
- Laryngeal telescope (0° or 30°, 5 mm) with digital video - for telescopic visualization; provides better depth assessment than microscope alone
Step-by-Step MLS Technique for Vocal Fold Polyp
Step 1 - Laryngoscope Insertion and Suspension
The rigid laryngoscope is introduced transorally and advanced to expose the glottis. It is then suspended using a suspension apparatus/chest support - freeing both hands for microsurgery. Both vocal folds are systematically inspected.
Step 2 - Arytenoid Palpation
The arytenoid cartilages are palpated with a spatula to confirm mobility (rules out cricoarytenoid fixation or malignant involvement).
Step 3 - Polyp Identification and Assessment
Under the operating microscope, the polyp is inspected for:
- Size and extent
- Pedunculation vs. broad base
- Location on the fold
- Vascularity (hemorrhagic vs. pale)
Step 4 - Mucosal Incision (Cold Technique - Microflap)
A microflap technique is preferred to preserve the delicate Reinke's space:
- A small incision is made in the overlying mucosa at the superior surface or free edge of the fold, just at the base of the polyp
- Using microsurgical elevators or suction instruments, the mucosa is gently elevated off the polyp
Step 5 - Polyp Excision
- For pedunculated polyps: The polyp is grasped with heart-shaped or right-turning forceps to reveal its pedunculation and confirm mucosal flexibility; microsurgical scissors then cut the pedicle
- For broad-based / sessile polyps: Submucosal dissection separates the polyp from the underlying vocal ligament, then forceps and scissors excise the lesion
- The goal is to remove the polyp at the level of Reinke's space while preserving the vocal ligament and as much overlying epithelium as possible
"A long-standing polyp, whether hemorrhagic or at end stage and pale, should be trimmed away superficially at the time spot coagulations take place." - Cummings Otolaryngology
Step 6 - Hemostasis
- Spot coagulation of large capillaries identified in Reinke's space
- Cocaine-soaked pledgets applied for vasoconstriction and hemostasis
- For hemorrhagic polyps: the large feeding capillaries must be interrupted (slightly deeper coagulation may be needed to reach the capillary level)
Step 7 - Wound Check
- Inspect the residual wound - ideally a "tiny residual wound" is all that remains
- Ensure no contralateral mucosal injury (which could cause adhesions/web)
- Confirm no residual polyp tissue at the pedicle
Hemorrhagic Polyp: Special Surgical Considerations
For a recent, large hemorrhagic polyp (blood-blister appearance):
- Evacuation through a tiny incision may be preferred over waiting, as spontaneous resorption is unlikely and progression to chronic polyp is expected
- After hematoma evacuation, detect and interrupt the large capillaries within Reinke's space using spot coagulation
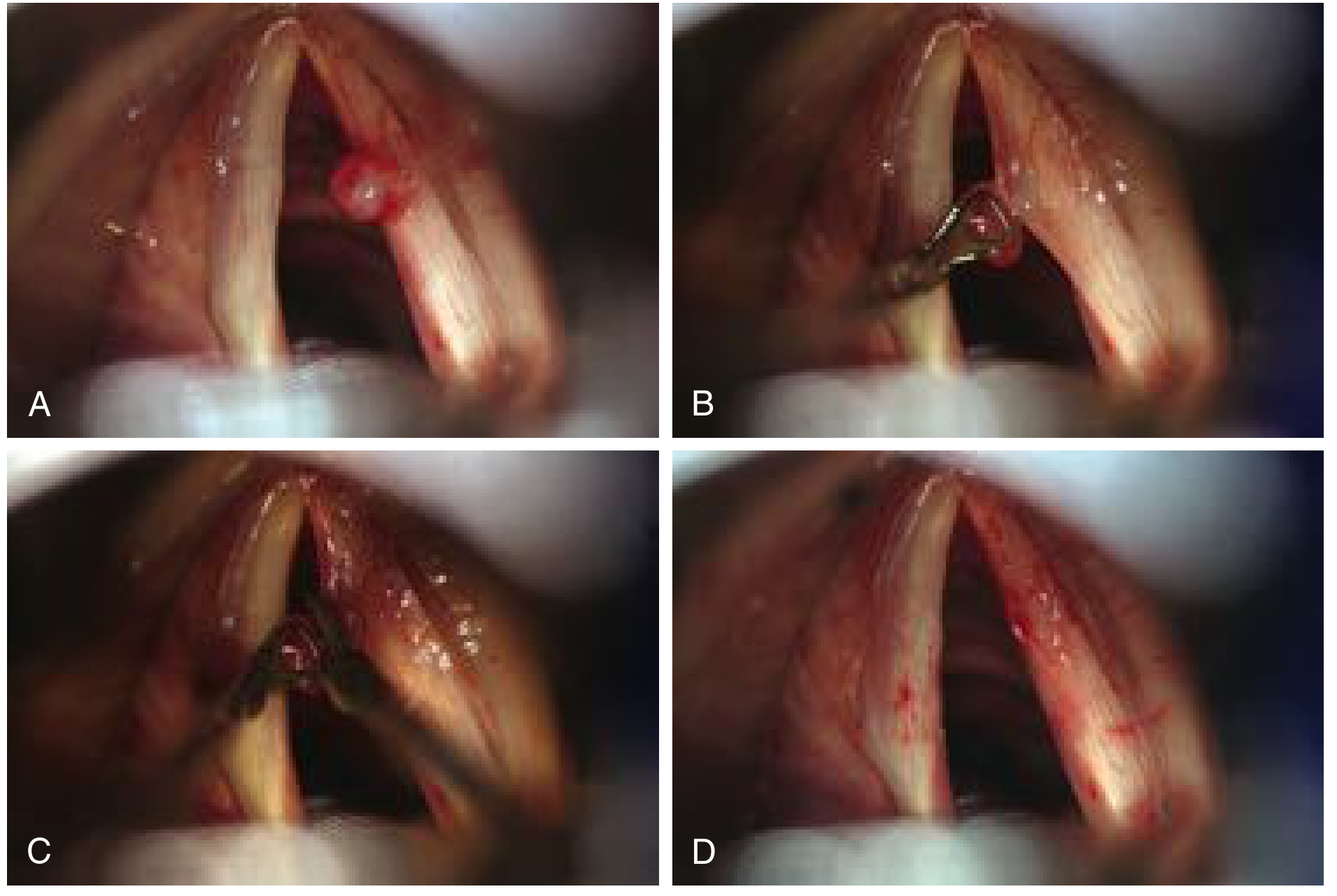
Fig. 60.12 - MLS excision of hemorrhagic vocal fold polyp (Cummings Otolaryngology, p. 1117)
Difficult Airway Considerations
Large pedunculated polyps pose a significant airway risk:
- A ball-valve pedunculated polyp can block the airway on expiration and may be dislodged into the trachea during intubation
- In such cases, awake fiberoptic nasotracheal intubation in the sitting position is the preferred approach
- A small cuffed ETT (5.0-6.0 mm microlaryngoscopy tube) is requested
- Hollinger laryngoscope (with narrow neck and distal anterior flare) provides better glottic exposure than the Dedo laryngoscope in difficult cases
Postoperative Care
- Voice rest for 5-7 days after surgery
- Voice therapy (short course) for vocal hygiene and to prevent recurrence
- Treat underlying GERD with PPIs
- Prognosis for full return of vocal functioning after precision microsurgery is excellent
Comparison: MLS vs. KTP Laser
| Feature | Cold Instrument MLS | KTP Laser (532 nm) |
|---|---|---|
| Anesthesia | General (suspension) | In-office OR under GA |
| Precision | Very high | High (vascular targeting) |
| Best for | All polyps; broad-based | Vascular/hemorrhagic polyps |
| Tissue preservation | Maximal | Good |
| Scar risk | Low with microflap technique | Low |
| Access | OR required | Can be office-based |
Sources: Cummings Otolaryngology Head and Neck Surgery | K.J. Lee's Essential Otolaryngology | Bailey and Love's Short Practice of Surgery, 28th ed.
Ot procedure
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.