Parkinsonism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here is a complete, structured overview of Parkinsonism:
Parkinsonism
Definition and Cardinal Features
Parkinsonism is a clinical syndrome - not a single disease - defined by the presence of some or all of six cardinal motor features:
- Tremor at rest - 4-6 Hz "pill-rolling" tremor, suppressed by voluntary movement
- Bradykinesia - slowness of movement, including reduced amplitude (hypokinesia) and absence of movement (akinesia)
- Rigidity - increased tone throughout the range of motion ("lead pipe"), often with "cogwheeling" when superimposed on tremor
- Loss of postural reflexes - impaired righting reflexes, leading to falls
- Flexed posture - stooped trunk and limb posture
- Freezing (motor blocks) - sudden involuntary inability to initiate or continue movement
The four core features are neatly summarized by the acronym TRAP: Tremor, Rigidity, Akinesia, Postural disturbances.
- Bradley and Daroff's Neurology in Clinical Practice
Classification of Parkinsonism
I. Parkinson Disease (PD) - Most Common
- Idiopathic / sporadic - the vast majority (~90%)
- Hereditary - see genetic causes below
II. Parkinsonism-Plus Syndromes (Atypical Parkinsonism)
Multisystem degenerations where parkinsonism is one component:
| Syndrome | Key Features |
|---|---|
| Progressive Supranuclear Palsy (PSP) | Vertical gaze palsy, falls backwards, axial rigidity |
| Multiple System Atrophy (MSA) | Autonomic failure; MSA-P (striatonigral) or MSA-C (cerebellar) |
| Corticobasal Degeneration (CBD) | Apraxia, alien limb phenomenon, cortical sensory loss |
| Dementia with Lewy Bodies (DLB) | Fluctuating cognition, visual hallucinations, REM sleep disorder |
III. Heredodegenerative Parkinsonism
Conditions where parkinsonism occurs as part of a broader hereditary syndrome:
- Wilson disease, Huntington disease, spinocerebellar ataxias
- Neurodegeneration with brain iron accumulation (NBIA)
- Frontotemporal dementia with parkinsonism (FTDP)
- Dopa-responsive dystonia (Segawa disease)
IV. Secondary (Acquired, Symptomatic) Parkinsonism
| Category | Examples |
|---|---|
| Drugs | Antipsychotics, antiemetics (metoclopramide), reserpine, tetrabenazine, methyldopa, lithium, flunarizine |
| Toxins | MPTP, carbon monoxide, manganese, mercury |
| Infectious | Postencephalitic, HIV, Creutzfeldt-Jakob disease |
| Vascular | Lacunar infarcts in the basal ganglia ("lower-body parkinsonism") |
| Structural | Normal-pressure hydrocephalus, tumor, trauma |
| Metabolic | Hypoparathyroidism (basal ganglia calcification) |
- Bradley and Daroff's Neurology in Clinical Practice
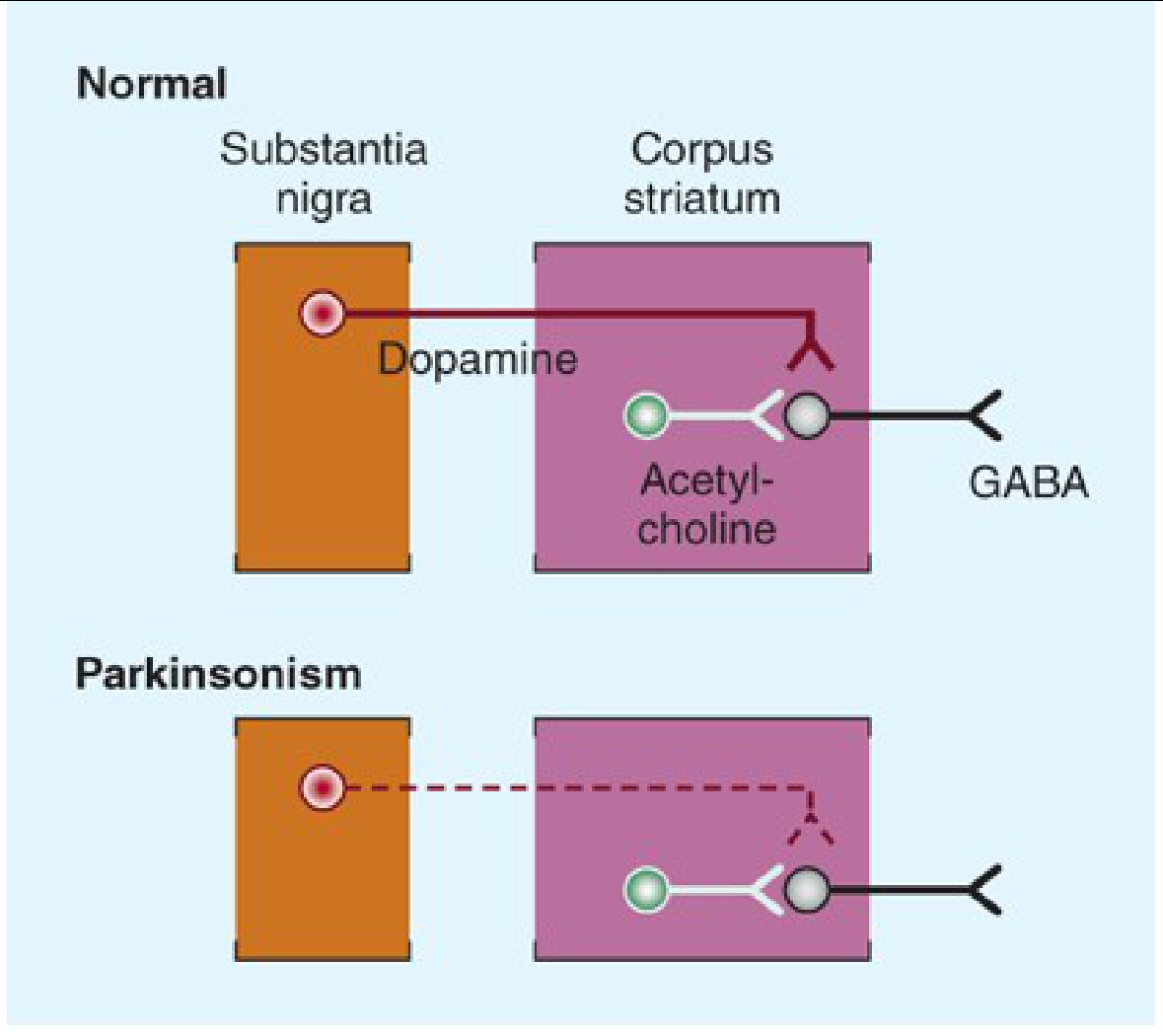
Pathophysiology
Normal Circuit
Dopaminergic neurons in the substantia nigra pars compacta (SNpc) project via the nigrostriatal pathway to the corpus striatum. They normally inhibit the GABAergic output neurons there, counterbalancing the excitatory cholinergic interneurons.
In Parkinsonism
There is selective loss of dopaminergic neurons in the SNpc. This tips the balance toward excessive cholinergic (acetylcholine) activity relative to dopamine - resulting in the over-inhibition of motor circuits. The result is the hypokinetic state of parkinsonism.
Pathological Hallmark of PD
- Lewy bodies - intraneuronal cytoplasmic inclusions containing misfolded α-synuclein protein
- Loss of >60-80% of dopaminergic neurons in SNpc before motor symptoms appear
Genetics of PD
| Gene (Locus) | Inheritance | Protein | Notes |
|---|---|---|---|
| PARK-SNCA (PARK1) | AD | α-Synuclein | Rare; missense mutations, duplications |
| PARK-Parkin (PARK2) | AR | Parkin | Up to 50% of early-onset PD |
| PARK-PINK1 (PARK6) | AR | PTEN-induced kinase 1 | Early onset |
| PARK-DJ-1 (PARK7) | AR | DJ-1 | Early onset |
| PARK-LRRK2 (PARK8) | AD | LRRK2 (dardarin) | Common in North Africans, Ashkenazi Jews |
| PARK-VPS35 (PARK17) | AD | VPS35 | |
| PARK-ATP13A2 (PARK9) | AR | Lysosomal P-type ATPase | Kufor-Rakeb syndrome |
Less than 10% of all PD has a definitive causative mutation.
- Bradley and Daroff's Neurology in Clinical Practice
Clinical Features of Parkinson Disease
Motor Symptoms
- Rest tremor (4-6 Hz, "pill-rolling"), often the first symptom, typically asymmetric at onset
- Bradykinesia: micrographia, hypomimia (masked facies - often misinterpreted as depression by family), hypophonia, reduced arm swing
- Cogwheel or lead-pipe rigidity
- Festinant gait (shuffling, forward-leaning, small steps), difficulty turning, en-bloc turning
- Postural instability: late feature, cause of falls
Non-Motor Symptoms
Non-motor features can precede motor symptoms by years ("prodromal PD") and include:
-
Neuropsychiatric: depression, anxiety, apathy, hallucinations, impulse control disorders
-
Cognitive: MCI progressing to dementia (PDD) in up to 75%; >25% convert to MCI within 3 years
-
Sleep: REM sleep behavior disorder (RBD) - highly specific prodromal marker; excessive daytime sleepiness
-
Autonomic: orthostatic hypotension, constipation, urinary dysfunction, erectile dysfunction, sweating abnormalities
-
Sensory: hyposmia/anosmia (often very early), pain
-
Gastrointestinal: constipation, gastroparesis (dysphagia)
-
Bradley and Daroff's Neurology in Clinical Practice; Katzung's Basic and Clinical Pharmacology
Treatment
1. Levodopa (most effective)
Dopamine cannot cross the blood-brain barrier (BBB), but levodopa (its precursor) enters via the L-amino acid transporter and is decarboxylated to dopamine in the brain. It is almost always given combined with carbidopa (a peripheral DOPA decarboxylase inhibitor) to:
- Reduce peripheral conversion (and side effects like nausea, hypotension)
- Increase CNS bioavailability
Adverse effects of levodopa:
- Motor: Dyskinesias (choreoathetosis) in up to 80% after 10+ years; motor fluctuations ("wearing off," "on-off" phenomena)
- GI: Nausea, vomiting (reduced by combining with carbidopa)
- Cardiovascular: Postural hypotension, arrhythmias
- Behavioral: Hallucinations, confusion, dopamine dysregulation syndrome, impulse control disorder
2. Dopamine Agonists
Direct D2/D3 receptor agonists - useful as monotherapy in early PD or as adjuncts:
| Drug | Route | Notes |
|---|---|---|
| Pramipexole | Oral | D3-selective; renal excretion |
| Ropinirole | Oral | D2 agonist; CYP1A2 metabolism |
| Rotigotine | Transdermal patch | Continuous delivery |
| Bromocriptine | Oral | Ergot derivative |
Key risks: nausea, postural hypotension, somnolence, hallucinations, impulse control disorders (gambling, hypersexuality), peripheral edema. Cardiac valvulopathy with ergot derivatives (pergolide, bromocriptine).
Avoid in patients >70 years or with risk factors for impulse control disorders.
3. MAO-B Inhibitors
Selegiline, rasagiline - reduce dopamine breakdown in the striatum. Used as adjuncts or in early disease. Rasagiline may have a mild disease-modifying effect (uncertain).
4. COMT Inhibitors
Entacapone, tolcapone - inhibit catechol-O-methyltransferase, extending the plasma half-life of levodopa. Added when "wearing off" develops.
5. Istradefylline
Adenosine A2A receptor antagonist (caffeine analog) - reduces "off" periods. Oral, 20-40 mg/day.
6. Anticholinergics (Antimuscarinic drugs)
Trihexyphenidyl, benztropine, biperiden - improve tremor and rigidity but not bradykinesia. Poorly tolerated in elderly and cognitively impaired patients.
7. Amantadine
NMDA antagonist - mild antiparkinsonian effect; reduces dyskinesias. Adverse effects include livedo reticularis, peripheral edema, confusion, and hallucinations. Withdraw gradually (risk of acute confusional state on abrupt discontinuation).
8. Surgical Treatment
Deep Brain Stimulation (DBS) of the subthalamic nucleus (STN) or globus pallidus interna (GPi) has largely replaced ablative procedures. High-frequency stimulation is effective for motor fluctuations and dyskinesias.
Contraindications to DBS: secondary/atypical parkinsonism, dementia, failure to respond to levodopa.
Focused Ultrasound Thalamotomy - for medically refractory tremor-dominant parkinsonism in patients who decline surgery.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Drug-Induced Parkinsonism
The most common cause of secondary parkinsonism. Caused by drugs that block dopamine receptors or deplete dopamine:
- Typical antipsychotics (haloperidol, chlorpromazine)
- Atypical antipsychotics (risperidone > olanzapine > quetiapine)
- Antiemetics (metoclopramide, prochlorperazine)
- Reserpine, tetrabenazine, methyldopa
Management: withdraw the causative drug. Anticholinergics or amantadine may help while waiting for recovery.
Parkinsonism-Plus: Key Distinguishing Features
| Feature | PD | PSP | MSA | DLB |
|---|---|---|---|---|
| Tremor | Prominent | Mild | Mild | Variable |
| Symmetry | Asymmetric | Symmetric | Symmetric | Variable |
| Falls | Late | Early (backward) | Early | Variable |
| Autonomic failure | Mild | Mild | Prominent | Prominent |
| Eye movement | Normal | Vertical gaze palsy | Normal | Visual hallucinations |
| Response to L-dopa | Good | Poor | Moderate | Partial |
| Dementia | Late | Late | Rare | Early |
Recent Evidence (2024-2026)
- Exercise network meta-analysis (2025, PMID 39880702) - identifies optimal exercise types and doses for improving motor symptoms in PD
- Virtual reality + conventional therapy meta-analysis (2025, PMID 40142335) - VR combined with conventional therapy significantly improves balance in PD
- Research into α-synuclein seed amplification assays in CSF shows high sensitivity/specificity for diagnosing PD, potentially before motor symptoms develop - a promising biomarker
Sources: Bradley and Daroff's Neurology in Clinical Practice | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Goldman-Cecil Medicine | Adams and Victor's Principles of Neurology
This is a shared conversation. Sign in to Orris to start your own chat.