Tripod fracture. From basic to clinical from standard ent text book including scott brown, cummings and baileys
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from all the major ENT textbooks. Let me compile the full, detailed response.
Tripod Fracture (Zygomaticomaxillary Complex Fracture) - A Comprehensive Review
Sourced from Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Cummings Otolaryngology, K.J. Lee's Essential Otolaryngology, Tintinalli's Emergency Medicine, and Rosen's Emergency Medicine
1. Nomenclature and Definition
The term "tripod fracture" historically described disruption of the three commonly recognized articulations of the zygoma:
- Frontozygomatic suture
- Infraorbital rim (zygomaticomaxillary)
- Zygomaticomaxillary buttress
"These injuries were originally termed 'tripod fracture' because of the disruption of the three commonly recognized articulations... In fact, there are two further articulations worthy of consideration: the zygomatic arch and the zygomaticosphenoid." — Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1
The modern preferred term is Zygomaticomaxillary Complex (ZMC) fracture or zygomatic complex fracture, because in reality there are five fracture lines:
- Frontozygomatic suture
- Infraorbital rim
- Zygomaticomaxillary buttress
- Zygomatic arch
- Zygomaticosphenoid suture (lateral orbital wall)
K.J. Lee also refers to it as an "orbitozygomatic fracture" and notes the historical development: Adams (1942) first described using wires for internal fixation, followed by the Swiss AO group introducing miniplate fixation.
2. Surgical Anatomy
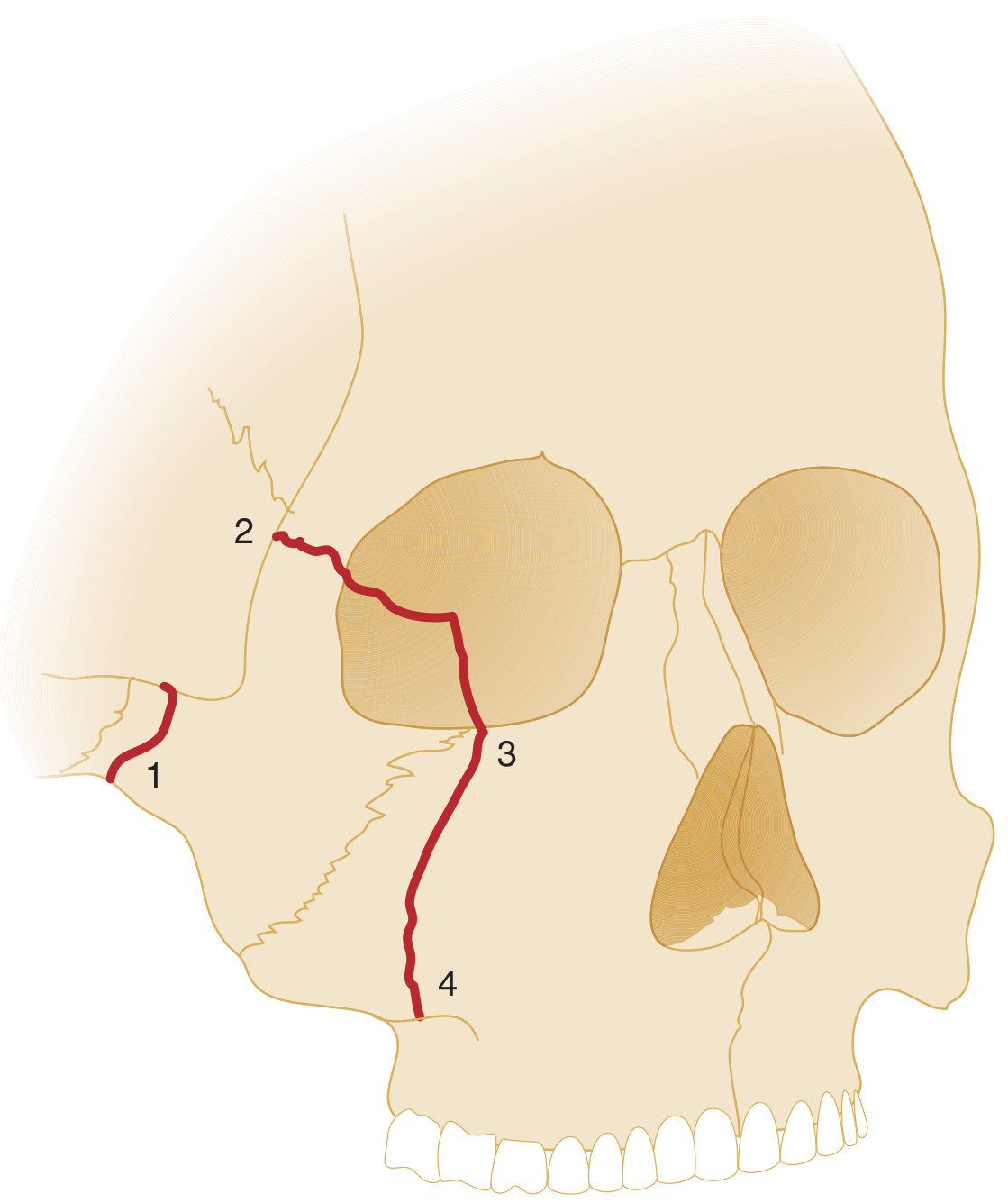
Fracture locations: 1 = zygomatic arch, 2 = frontozygomatic suture/lateral orbital rim, 3 = inferior orbital rim, 4 = zygomaticomaxillary buttress (Tintinalli's Emergency Medicine)
The zygoma forms the lateral cheek prominence and makes up:
- The lateral orbital wall and floor - protects the globe
- The zygomatic arch - articulates with the temporal bone
- The malar eminence - determines facial width and projection
The body and processes of the zygomatic bone make up the lateral middle third of the facial skeleton. It provides support and protection for the globe of the eye. Accurate anatomical reduction is important for:
- Facial appearance (malar projection)
- Optimum function of the eye
- Mouth opening (the zygoma lies close to the coronoid process of the mandible)
(Scott-Brown's, Vol 1)
Buttresses
The zygoma sits at the intersection of key facial buttresses. The zygomaticomaxillary buttress accepts and transmits masticatory forces from the maxilla to the skull base. The masseter muscle has a powerful attachment to the zygomatic arch and body - its action tends to pull fracture fragments inferomedially, making stabilization difficult.
From Cummings: "The zygoma forms an important attachment for the powerful masseter muscle. To support the function of this muscle, the bone needs to be solidly attached; yet in order to crumple and protect the orbit from injury, the bone must be weaker at specific areas."
Biomechanics (KJ Lee)
- Masseter and temporalis exert dominant dynamic forces that must be overcome at the fracture site for stabilization
- Callous bone formation occurs with movement at the fracture site (fibroblastic response → bone)
- Primary healing occurs with immobilization (direct ossification via Haversian canal alignment) - this is the stronger union
- Bone resorption occurs with inadequate reduction/stabilization, contributing to enophthalmos
3. Mechanism of Injury
- Classic mechanism: High-energy deceleration injury, direct blow to the malar eminence (assault, road traffic accident, sports)
- Tintinalli: "The less common zygomaticomaxillary (or 'tripod') fracture results classically from a high-energy deceleration injury with disruption of the zygomaticfrontal suture, zygomaticotemporal junction, and infraorbital rim."
- The direction of impact determines the pattern of displacement
4. Classification
Knight and North Classification (KJ Lee)
| Type | Description | Mechanism |
|---|---|---|
| Type I | No significant displacement; attached at all sutures | - |
| Type II | Incomplete downward and lateral displacement; ZM suture hinge, ZF suture intact | Blunt force lateral to inferior orbital rim |
| Type IIa | Incomplete displacement; hinged on ZM suture, ZF suture detached | Blunt injury directed inferiorly from above |
| Type IIIb | Incomplete supero-posterior displacement; hinged at ZM suture, ZF suture detached | Blunt force directed superiorly from below |
| Type IV | Complete fracture displaced inferiorly; internal rotation of inferior orbital rim and medial displacement | Direct blow to zygomatic arch |
(KJ Lee's Essential Otolaryngology, p. 1125)
Cummings adds: Manson's energy-based severity classification - the amount of displacement and comminution reflects the energy transmitted at the time of injury, and this guides the extent of surgical exposure and fixation needed.
5. Clinical Features
Symptoms
- Malar flattening / loss of cheek projection (may be masked early by swelling)
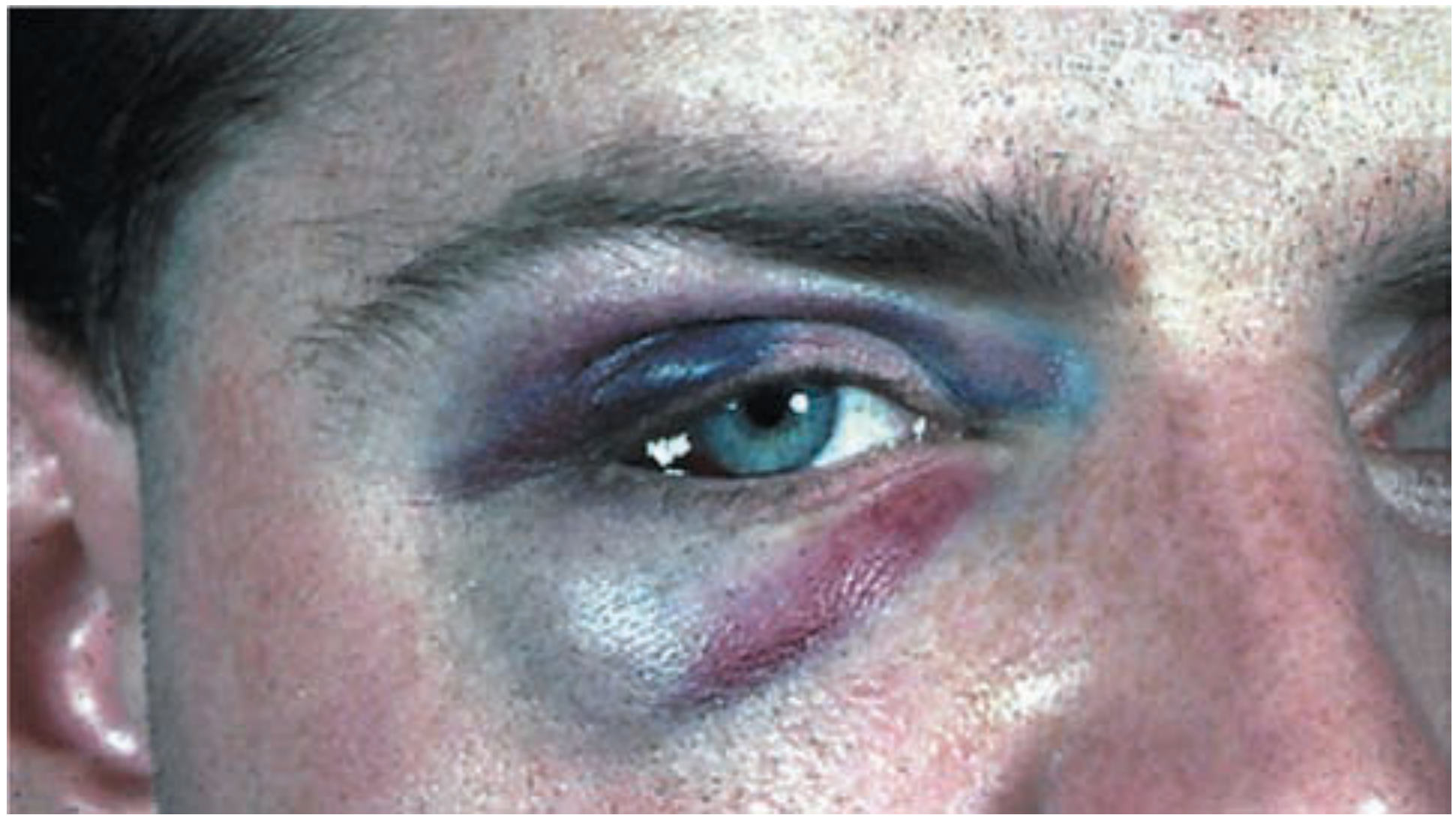
- Periorbital swelling and ecchymosis
- Diplopia - especially on upward gaze (orbital floor blow-out component, inferior rectus/oblique entrapment)
- Infraorbital nerve hypoesthesia/anaesthesia - cheek, upper lip, ipsilateral teeth (zygomaticocotemporal and zygomaticobuccal nerves)
- Trismus / restricted mouth opening - due to impingement of the depressed zygomatic arch on the coronoid process of the mandible
- Epistaxis - hemosinus
Signs
On examination:
- Best examined from front, above, and behind the patient
- Subconjunctival hemorrhage - almost invariably present in fractures of the zygomatic body
- Tenderness at the frontozygomatic suture
- Step deformity of the infraorbital margin (palpable)
- Reduced malar projection (once swelling resolves)
- Restricted upward gaze (orbital floor dehiscence)
- Palpable depression of the zygomatic arch
- Altered cheek sensation (infraorbital nerve distribution)
6. Investigations
Imaging
Plain Radiographs:
- Occipitomental (Waters') view at 15° and 30° shows most fractures
- Scott-Brown notes: "Whilst most fractures are visible on 15 and 30° occipitomental X-rays, CT scanning is increasingly becoming standard of care particularly if there are signs of diminished ocular motility."
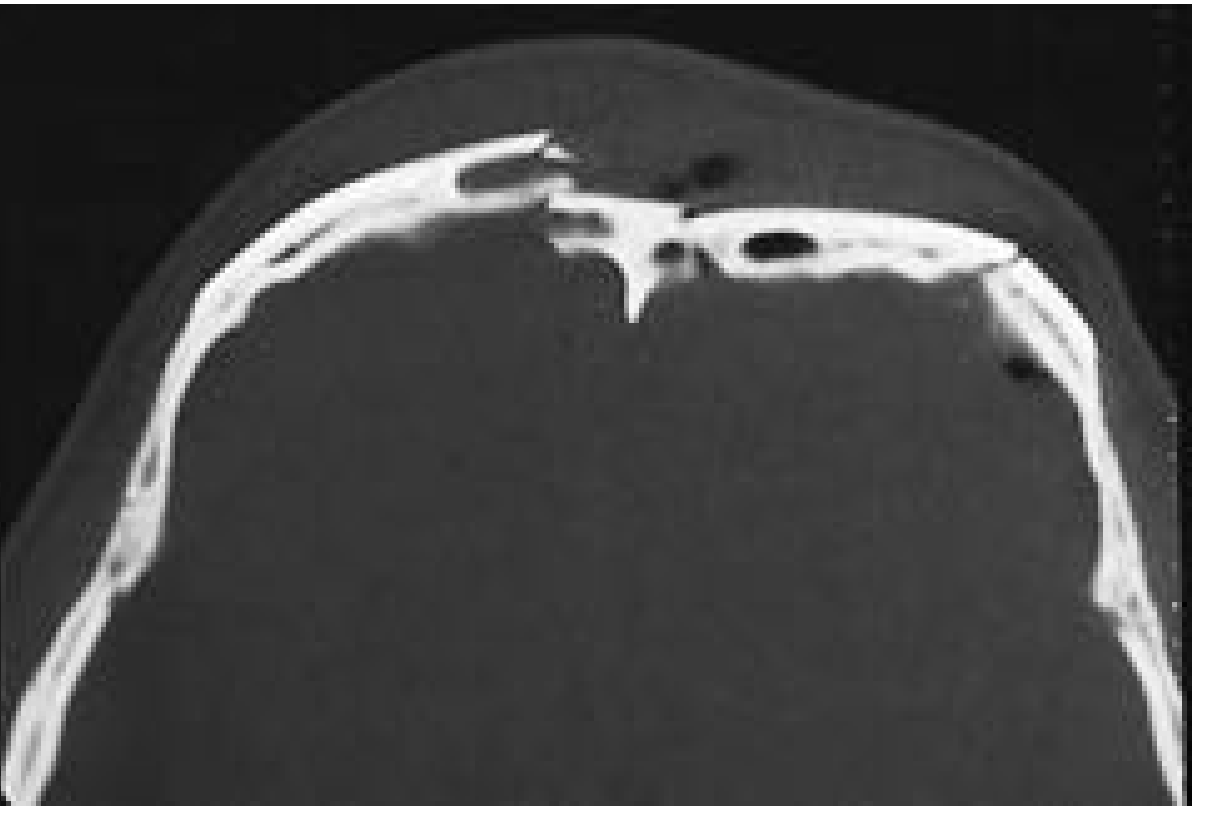
CT Scan (Gold Standard):
- Axial + coronal + sagittal reformatting = best standard of care
- Axial CT best for: zygomatic arches, vertical orbital walls
- Coronal CT best for: orbital floor and roof, pterygoid plates
- 3D reconstruction useful for surgical planning (scans must be <1.5 mm slice thickness for reliable 3D reconstruction - Cummings)
Ophthalmological Assessment (Scott-Brown Best Practice)
- Visual acuity - mandatory; retrobulbar hemorrhage causing vision loss is rare but treatable
- Hess charting - assesses extraocular muscle function; post-operative comparison
- Hertel exophthalmometry - objective measurement of globe position (limited value acutely)
7. Management
Conservative (Non-operative)
- Non-displaced / minimally displaced fractures: conservative management
- Soft diet, malar protection, close follow-up at 10 days (once swelling has resolved, to confirm no active intervention needed)
- Instructions not to blow the nose for 2-3 weeks (prevents orbital emphysema)
- (Scott-Brown's, KJ Lee)
Surgical - Indications
- Displaced fracture
- Cosmetic deformity (malar flattening)
- Functional deficits: diplopia, enophthalmos, restricted mouth opening
- Infraorbital nerve deficit (relative indication)
- High-energy fractures with comminution
Reduction Techniques
The method depends on the surgeon's preference and fracture configuration. Each has advocates and specific advantages:
| Approach | Indication | Advantage | Disadvantage |
|---|---|---|---|
| Gillies temporal | Medially displaced body, arch fractures | Elevating site distant from fixation | Skin incision, visible in bald patients |
| Dingman | Medially displaced body | Common incision with frontozygomatic access | Difficult to plate and elevate simultaneously |
| Poswillo hook | Posteriorly displaced; NOT arch fractures | Good mechanical advantage, quick | Hook point on lateral cheek, may be noticeable |
| Keen (intra-oral) | Medially displaced, arch fractures | Avoids cutaneous scars | Doesn't address ZF suture; oral contamination risk |
| Coronal | Laterally displaced arch fractures | Only approach for this rare fracture | Extensive surgical exposure |
(Scott-Brown's Table 107.2)
Gillies Temporal Approach (detailed)
- Shave hair just anterior to the ear; infiltrate local anaesthetic with adrenaline
- Small incision down to superficial temporal fascia
- Fascia incised; elevator passed down on the temporalis muscle (deep to temporalis fascia / superficial to muscle)
- Tip of elevator positioned just under the fracture
- Bone elevated (both infraorbital margins exposed for comparison)
KJ Lee - Gillies Procedure for Isolated Arch Fracture:
- 2-3 cm incision in temporal hairline
- Dissection continued deep to temporalis fascia
- Dingman elevator used to elevate arch
- If stable after reduction: no further intervention
- If unstable: two options:
- ORIF through transcranial incision
- Stenting with spinal needle passed transcutaneously beneath the arch (left 10 days)
Open Reduction and Internal Fixation (ORIF)
Indications: Diastasis at the frontozygomatic suture, high-energy fractures, unstable after closed reduction
Surgical access for orbitozygomatic fractures (3 incisions - KJ Lee):
- Lateral upper lid crease incision (frontozygomatic access)
- Gingivobuccal sulcus incision (zygomaticomaxillary buttress)
- Lower eyelid incision - transconjunctival with "swinging" eyelid OR subciliary
Orbital access incisions (Scott-Brown Table 107.1):
| Incision | Advantage | Disadvantage |
|---|---|---|
| Transconjunctival | Good exposure, aesthetic | Slight risk of entropion |
| Transconjunctival with cantholysis | Excellent exposure | Risk of lid malposition |
| Transconjunctival + transcaruncular | Excellent for medial orbital wall | Technically difficult |
| Lower eyelid (subciliary) | Straightforward | Risk of ectropion, visible scar |
| Infraorbital | Rapid | Poor cosmesis |
Fixation hardware (KJ Lee / Cummings):
- Miniplate at the zygomaticomaxillary buttress - to counteract the action of masseter (dominant force)
- Microplate at infraorbital rim and frontozygomatic suture (except high-energy fractures which require miniplates everywhere)
- Combination of microplate + miniplate is best tolerated and provides optimal rigid stabilization
- Screws: typically 1.3-1.5 mm low-profile miniplates along the buttresses
Fracture reduction technique (KJ Lee):
- Carol Gerard screw placed in zygomatic body through lower eyelid incision (after periosteal elevation)
- Alternatively, Dingman elevator beneath zygomatic arch through upper lid crease
- Key principle: Must directly visualize reduction at ALL fracture sites before fixation - anatomical reduction at one site may be accompanied by malalignment at another
The zygomatic arch is the key to proper repair (KJ Lee). Cummings emphasizes that alignment of the zygoma with the greater wing of the sphenoid in the lateral orbit is a dependable landmark for proper bony reduction.
8. Orbital Floor Component
ZMC fractures frequently disrupt the orbital floor. Scott-Brown summarizes this separately:
Signs of orbital floor fracture:
- Enophthalmos and hypoglobus (depressed pupillary level) - cardinal signs
- Supratarsal hollowing, narrowing of palpebral fissure width
- Infraorbital nerve deficit
- Trap-door phenomenon: entrapment of orbital fat or inferior oblique muscle → diplopia on upward gaze
Management:
- Significant orbital floor injury requires exploration and repair
- All soft-tissue components must be mobilized and supported by a graft
- Materials: polydimethylsiloxane (PDS) sheets for smaller defects; titanium alloplasts (prefabricated or CAD-CAM custom) for complex defects
9. Post-operative Care and Complications
Immediate Post-operative Instructions (Scott-Brown)
- No nose blowing
- First 12 hours: close observation for retrobulbar hemorrhage
Retrobulbar Hemorrhage (Emergency - Scott-Brown Key Points)
An ophthalmic emergency requiring urgent action:
- Symptoms: Increasing pain, proptosis, ophthalmoplegia, diminishing visual acuity, palpable increase in ocular pressure
- Management:
- Dexamethasone 4 mg/kg bolus, then 2 mg/kg 6-hourly
- Acetazolamide 500 mg IV
- Mannitol 20%, 200 mL
- Remove sutures and consider lateral canthotomy (surgical decompression)
Long-term Complications
- Malunion / secondary deformity - most important long-term complication
- Persistent enophthalmos (bone resorption from inadequate reduction)
- Diplopia (persistent EOM restriction)
- Infraorbital nerve hypoesthesia
- Malar flattening
- Trismus
Scott-Brown emphasizes: "It is important to realize that early accurate anatomical reduction provides the best results. Secondary reconstruction is difficult because of bony remodelling and fibrosis in the overlying soft tissues."
10. Summary Table
| Feature | Detail |
|---|---|
| Eponym | Tripod / trimalar / zygomaticomaxillary complex (ZMC) fracture |
| Fracture lines | 5 (arch, frontozygomatic, infraorbital rim, ZM buttress, zygomaticosphenoid) |
| Classic mechanism | High-energy direct blow to malar eminence |
| Hallmark sign | Subconjunctival hemorrhage + malar flattening |
| Nerve at risk | Infraorbital nerve (V2 branch) |
| Muscle causing displacement | Masseter (pulls fragment inferiorly and medially) |
| Imaging gold standard | CT axial + coronal + sagittal reconstruction |
| Conservative Rx | Non-displaced: soft diet, no nose blowing, review at 10 days |
| Closed reduction | Gillies temporal, Poswillo hook, Keen (intra-oral) |
| ORIF | 3-incision approach; miniplate at ZM buttress + microplate at rim/ZF |
| Emergency complication | Retrobulbar hemorrhage → lateral canthotomy |
| Late complication | Malunion, enophthalmos, persistent diplopia |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1 - Chapter 107 (Facial Fractures)
- Cummings Otolaryngology Head and Neck Surgery - Chapter 20 (Facial Trauma)
- K.J. Lee's Essential Otolaryngology - Chapter on Lateral Wall/Orbitozygomatic Fractures
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Chapter 259 (Zygoma Fractures)
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Chapter on Midface Fractures
This is a shared conversation. Sign in to Orris to start your own chat.