Hello
Hello! I'm Orris. How can I help you today?
Make notes on scapula
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here are comprehensive notes on the scapula, sourced from Gray's Anatomy for Students:
Scapula - Anatomy Notes
Overview
The scapula (shoulder blade) is a large, flat, triangular bone that forms the posterior part of the pectoral girdle. It lies on the posterolateral aspect of the thoracic wall, overlying ribs II-VII.
Basic Structure
The scapula has:
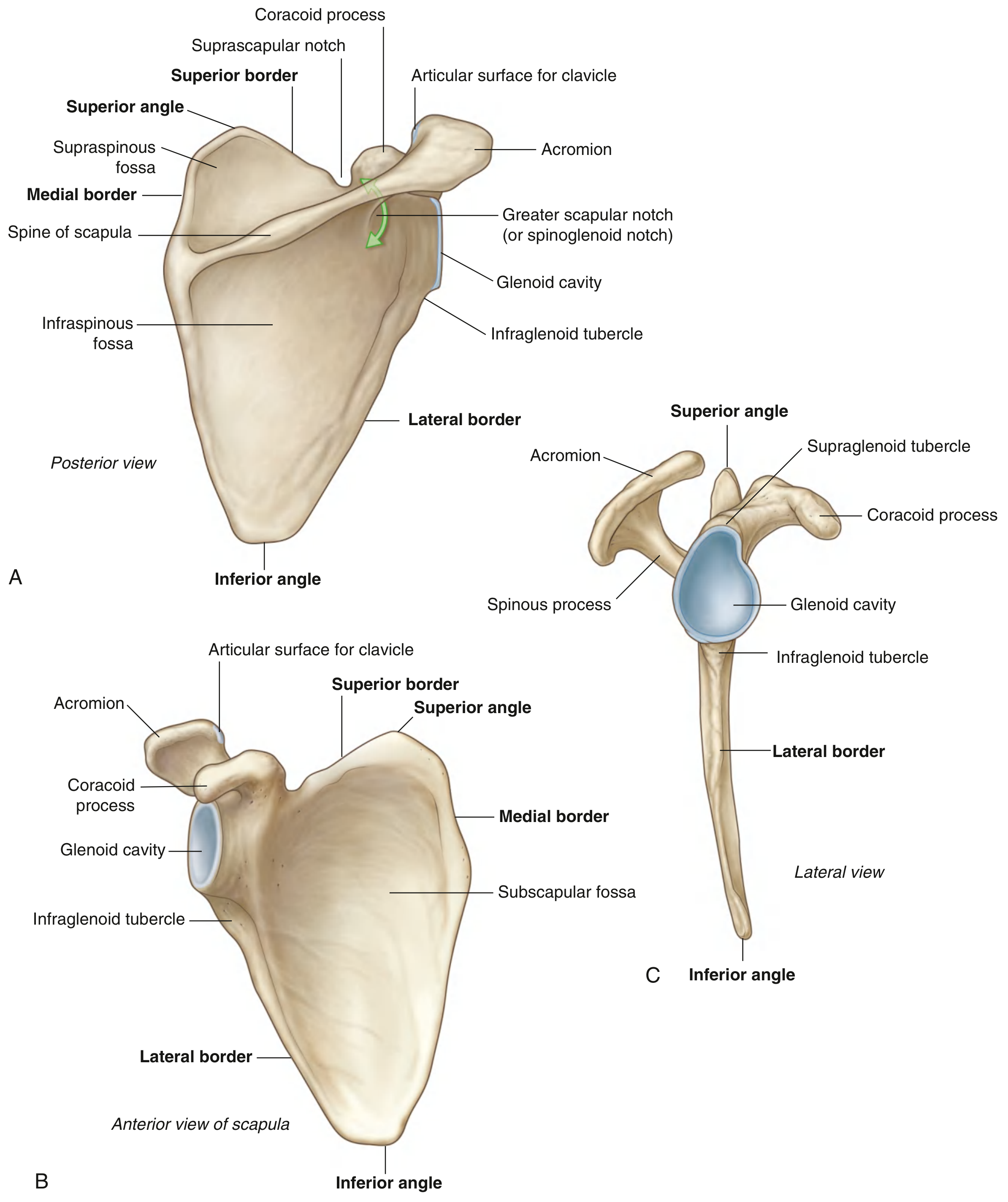
- 3 Angles: lateral, superior, inferior
- 3 Borders: superior, lateral (axillary), medial (vertebral)
- 2 Surfaces: costal (anterior) and posterior
- 3 Processes: acromion, spine, coracoid process
Borders
| Border | Description |
|---|---|
| Lateral (axillary) | Strong and thick - for muscle attachment |
| Medial (vertebral) | Thin and sharp |
| Superior | Thin; marked laterally by the suprascapular notch and the root of the coracoid process |
Angles
- Lateral angle - Marked by the glenoid cavity (shallow, comma-shaped), which articulates with the head of the humerus to form the glenohumeral joint
- Superior angle - At the junction of the medial and superior borders
- Inferior angle - Easily palpable; moves forward during arm elevation (used clinically to assess scapular rotation)
Surfaces
Posterior Surface
- Divided by the prominent spine of the scapula into:
- Supraspinous fossa (small, superior) - contains supraspinatus
- Infraspinous fossa (large, inferior) - contains infraspinatus
- The greater scapular notch (spinoglenoid notch) lies between the lateral angle and the attachment of the spine
Costal (Anterior) Surface
- Characterized by the large concave subscapular fossa
- Moves freely over the thoracic wall (on the subscapularis muscle)
Processes
Spine
- Prominent ridge on the posterior surface
- Projects laterally to become the acromion
- Both trapezius and deltoid attach to opposing surfaces of the spine
Acromion
- Anterolateral projection of the spine
- Arches over the glenohumeral joint
- Articulates with the clavicle via a small oval facet - forming the acromioclavicular (AC) joint
- Easily palpable
Coracoid Process
- Hook-like structure on the superior border
- Projects anterolaterally, lying directly inferior to the lateral part of the clavicle
- Site of attachment for:
- Pectoralis minor
- Short head of biceps brachii
- Coracobrachialis
Tubercles and Notches
| Feature | Location | Significance |
|---|---|---|
| Infraglenoid tubercle | Inferior to glenoid cavity | Attachment of long head of triceps brachii |
| Supraglenoid tubercle | Superior to glenoid cavity | Attachment of long head of biceps brachii |
| Suprascapular notch | Superior border, medial to coracoid | Suprascapular nerve passes through; suprascapular artery passes over the ligament |
Muscles Attached to the Scapula
Muscles Connecting Scapula to the Trunk
| Muscle | Origin | Insertion on Scapula | Action | Nerve |
|---|---|---|---|---|
| Trapezius | Occiput, nuchal line, spinous processes C7-T12 | Spine, acromion | Elevates, retracts, rotates scapula | Accessory (CN XI) |
| Serratus anterior | Lateral surfaces ribs 1-9 | Costal surface, medial border | Protracts, rotates scapula; keeps it against thorax | Long thoracic nerve (C5, C6, C7) |
| Levator scapulae | Transverse processes C1-C4 | Medial border, superior angle to root of spine | Elevates scapula | Dorsal scapular nerve + C3, C4 |
| Rhomboid minor | Lower ligamentum nuchae, spinous processes C7-T1 | Medial border at root of spine | Elevates and retracts scapula | Dorsal scapular nerve (C5) |
| Rhomboid major | Spinous processes T2-T5 | Medial border from spine to inferior angle | Elevates and retracts scapula | Dorsal scapular nerve (C4, C5) |
Muscles of the Posterior Scapular Region (Rotator Cuff + Others)
| Muscle | Origin (Scapula) | Insertion (Humerus) | Action | Nerve |
|---|---|---|---|---|
| Supraspinatus | Medial 2/3 supraspinous fossa | Superior facet of greater tubercle | Abduction + stabilization | Suprascapular nerve (C6) |
| Infraspinatus | Medial 2/3 infraspinous fossa | Middle facet of greater tubercle | Lateral rotation + stabilization | Suprascapular nerve (C6) |
| Teres minor | Upper 2/3, lateral border (posterior) | Inferior facet of greater tubercle | Lateral rotation + stabilization | Axillary nerve (C6, C7) |
| Teres major | Posterior surface of inferior angle | Medial lip of intertubercular sulcus | Medial rotation, adduction, extension | Lower subscapular nerve (C6, C7) |
| Subscapularis | Subscapular fossa | Lesser tubercle | Medial rotation + stabilization | Upper + lower subscapular nerves (C5, C6) |
Movements of the Scapula
| Movement | Prime Movers |
|---|---|
| Elevation | Trapezius (upper), levator scapulae, rhomboids |
| Depression | Trapezius (lower), serratus anterior (lower) |
| Protraction (forward) | Serratus anterior |
| Retraction | Rhomboids, trapezius (middle) |
| Upward rotation (glenoid tilts up) | Trapezius + serratus anterior |
| Downward rotation | Rhomboids, levator scapulae |
Scapulothoracic Joint
- Not a true synovial joint - it is a physiological joint (soft tissue articulation)
- The costal surface of the scapula glides over the thoracic wall on a "cushion" of serratus anterior and subscapularis
- Allows the wide range of scapular movements described above
Neurovascular Supply
| Structure | Detail |
|---|---|
| Suprascapular nerve | From upper trunk of brachial plexus (C5, C6); passes through suprascapular notch; supplies supraspinatus and infraspinatus |
| Suprascapular artery | Branch of thyrocervical trunk; passes over the transverse scapular ligament (not through the notch) |
| Dorsal scapular nerve | C5 root; supplies rhomboids and levator scapulae |
| Long thoracic nerve | C5, C6, C7; runs on the external surface of serratus anterior - very vulnerable to injury |
Clinical Correlates
Winged Scapula
- Caused by damage to the long thoracic nerve (e.g., during axillary surgery, mastectomy, or lateral thoracotomy)
- Results in paralysis of serratus anterior
- The medial border and inferior angle of the scapula lift away from the thorax posteriorly
- Winging is accentuated when the patient pushes against a wall or elevates the arm
- Normal arm elevation is no longer possible above horizontal
Suprascapular Nerve Entrapment
- Nerve can be compressed at the suprascapular notch
- Causes weakness and wasting of supraspinatus and infraspinatus
- Presents as shoulder pain and weakness of abduction and lateral rotation
Scapular Fractures
- Uncommon due to protective surrounding musculature
- When they do occur, they imply a significant force and associated injuries (neurovascular, thoracic) must be actively sought
Sources: Gray's Anatomy for Students, Chapter 7 (Upper Limb); pp. corresponding to scapula section and posterior scapular region.
This is a shared conversation. Sign in to Orris to start your own chat.