Pulled elbow
Reading File
Finding Sources
Searching PubMed
"pulled elbow" OR "nursemaid's elbow" radial head subluxation reduction
Finding Sources
Searching PubMed
"radial head subluxation" child reduction technique
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of pulled elbow (nursemaid's elbow / radial head subluxation), compiled from Roberts & Hedges' Clinical Procedures in Emergency Medicine, Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, and Miller's Review of Orthopaedics.
Pulled Elbow (Nursemaid's Elbow / Radial Head Subluxation)
Definition & Epidemiology
Pulled elbow is a partial dislocation (subluxation) of the radial head in young children. It accounts for more than 20% of all upper extremity injuries in children.
- Peak age: 1-4 years (mean ~2 years); rare under 6 months or over 6-7 years
- Sex predilection: Girls slightly more than boys
- Side: Left arm more commonly affected than right (dominant arm is more commonly grabbed)
Pathophysiology
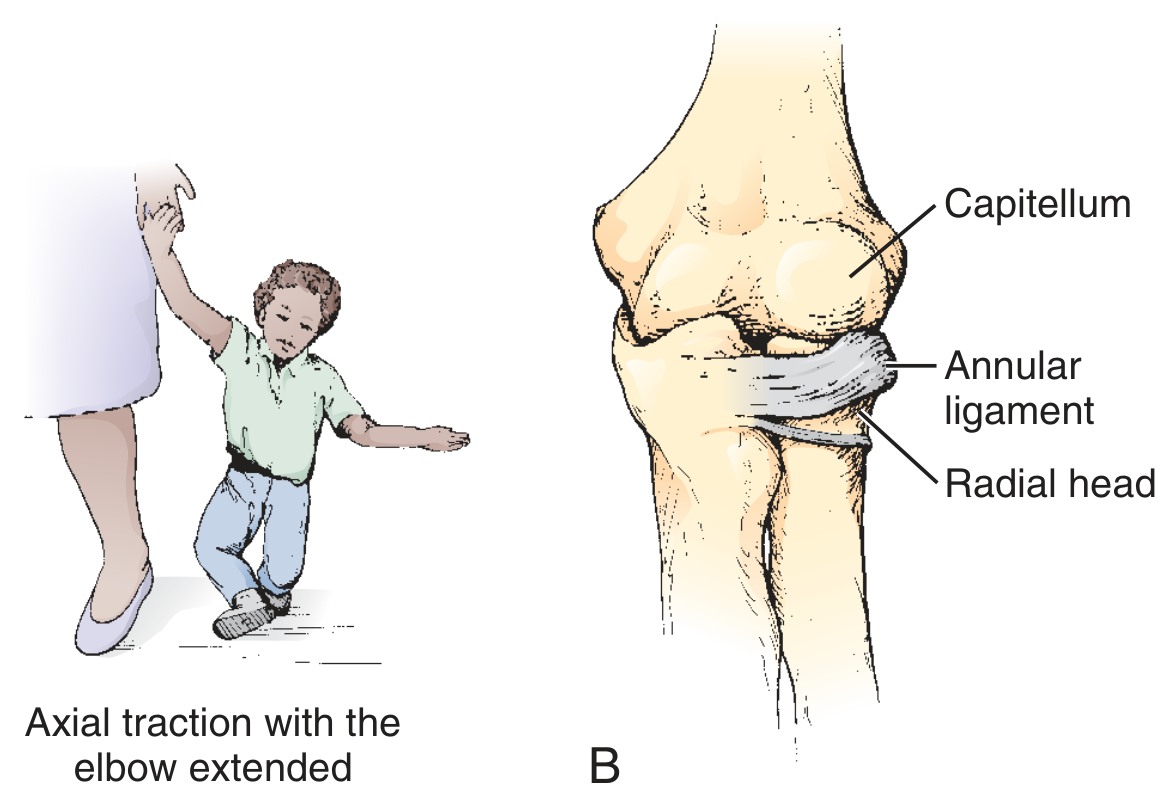
The injury results from longitudinal (axial) traction on a pronated, extended forearm - classically when an adult lifts or swings a child by the wrist or hand. The annular ligament (which encircles the radial neck) tears at its periosteal attachment and a detached portion becomes entrapped between the radial head and the capitellum of the humerus.
After age 5, the annular ligament becomes thicker and stronger, making this injury much less likely.
Other mechanisms (less classic): fall, rolling over in bed (infants), twisting of the arm.
Clinical Features
| Feature | Detail |
|---|---|
| Arm position | Held in slight elbow flexion + forearm pronation ("nursemaid's position") |
| Pain | Acute onset; child refuses to use the arm |
| Swelling/bruising | Absent (distinguishes from fracture) |
| Tenderness | Minimal or none at the elbow; some tenderness directly over the radial head |
| Point child identifies | Older children often point to the dorsal distal forearm (can mislead toward a buckle fracture) |
The classic pulling history is only present in about 50% of cases - absence of a typical history should not exclude the diagnosis.
Diagnosis
This is a clinical diagnosis. Imaging is generally not indicated when:
- History and examination are typical
- Arm is held in the nursemaid's position
- No swelling, bruising, or focal bony tenderness
When to X-ray:
- Swelling, ecchymosis, or deformity present
- Atypical history or mechanism
- Concern for non-accidental injury
- Child does not resume use of arm 24 hours after presumed reduction
- Bony tenderness on palpation away from the elbow (clavicle, wrist)
Ultrasound ("hook sign"): the hyperechoic J-shaped supinator muscle above the displaced radial head is reported to be 100% sensitive for radial head subluxation. Useful to exclude posterior fat pad (supracondylar fracture) and spare radiation exposure. - Roberts & Hedges', p. 1151-1152
Reduction Techniques
No analgesia is typically required before reduction. Two methods are commonly used:
1. Hyperpronation (Preferred)
- Support the elbow and place moderate pressure on the radial head with your thumb
- Grasp the child's distal forearm as if shaking hands
- Rapidly hyperpronation the forearm while the elbow remains flexed
- A palpable or audible "click" is felt at the radial head = successful reduction
- Evidence: A 2012 Cochrane review and a 2017 meta-analysis both concluded hyperpronation has higher first-attempt success and is less painful than supination-flexion. - Tintinalli's Emergency Medicine, p. 955; Rosen's Emergency Medicine, p. 639
2. Supination-Flexion (Traditional)
- Stabilize the humerus; place thumb over the radial head
- Grasp the child's wrist; supinate the forearm (slight traction can be applied first)
- In one continuous motion, flex the elbow while maintaining supination
- A click signifies reduction
If one method fails, switch to the other. Up to 30% of patients require two or more attempts to produce the click.
Post-Reduction Assessment
- Child typically cries briefly, then settles
- Full arm use should return within 10-15 minutes (up to 30 minutes in some)
- Leave the room and allow the parent to distract the child to demonstrate normal function
- 90% of children regain full arm use within 30 minutes
- If no improvement after 30 minutes: repeat reduction attempt
- If still no improvement after reasonable attempts: obtain radiographs; consider 24-hour follow-up
No immobilization is needed after successful reduction in a straightforward first episode. A sling or splint may be used if the child has prolonged discomfort (e.g., delayed presentation) or recurrent subluxations.
Recurrence & Prognosis
- Recurrence rate: approximately 20% - Rosen's Emergency Medicine, p. 639
- Uncommon after age 5 as the annular ligament strengthens
- Parents and caregivers should be counseled to avoid pulling or swinging the child by the wrist or hands
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Radial head/neck fracture | Focal bony tenderness; swelling; mechanism is direct trauma or FOOSH |
| Supracondylar fracture | Swelling, deformity; posterior fat pad on X-ray |
| Distal radius buckle fracture | Wrist tenderness and swelling |
| Lateral condyle fracture | Lateral elbow swelling and tenderness |
| Septic arthritis / osteomyelitis | Fever, systemic illness, diffuse warmth |
Sources: Tintinalli's Emergency Medicine (p. 953-955), Rosen's Emergency Medicine (p. 639), Roberts & Hedges' Clinical Procedures in Emergency Medicine (p. 1151-1153), Miller's Review of Orthopaedics 9th ed. (p. 940)
This is a shared conversation. Sign in to Orris to start your own chat.