Define chronic bronchitis. Discuss its clinical features and investigation for chronic bronchitis.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Here is the complete response:
Chronic Bronchitis
Definition
Chronic bronchitis is defined clinically as a persistent productive cough lasting for at least 3 consecutive months in at least 2 consecutive years, in the absence of any other identifiable cause (e.g., bronchiectasis, tuberculosis, or cardiac failure). Unlike emphysema, which is defined anatomically, the definition of chronic bronchitis is entirely based on clinical symptoms. Daily cough with sputum production is the core qualifying criterion.
- Robbins & Kumar Basic Pathology, p. 449
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 637
Pathogenesis
The primary initiating factor is inhalation of noxious or irritating substances. Around 90% of affected patients are smokers. Other causes include air pollutants (sulfur dioxide, nitrogen dioxide), grain/cotton/silica dust, recurrent pulmonary infections, and familial factors.
Key pathogenic mechanisms:
- Mucus hypersecretion - The earliest and hallmark feature. Irritants stimulate hypertrophy of mucous glands in the trachea and bronchi, and an increase in goblet cells in bronchioles. Inflammatory mediators (IL-13, histamine) drive this process.
- Acquired CFTR dysfunction - Cigarette smoking causes acquired CFTR dysfunction, leading to abnormal, dehydrated mucus that worsens obstruction.
- Inflammation - Inhalants cause cellular damage, recruiting neutrophils, lymphocytes, and macrophages (notably, eosinophils are absent, unlike in asthma).
- Infection - Does not initiate chronic bronchitis but sustains it and triggers acute exacerbations. Cigarette smoke impairs mucociliary clearance, increasing infection risk.
- Small airway disease - Airflow obstruction results from chronic bronchiolitis: mucus plugging, bronchiolar wall inflammation, and fibrosis.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 637-638
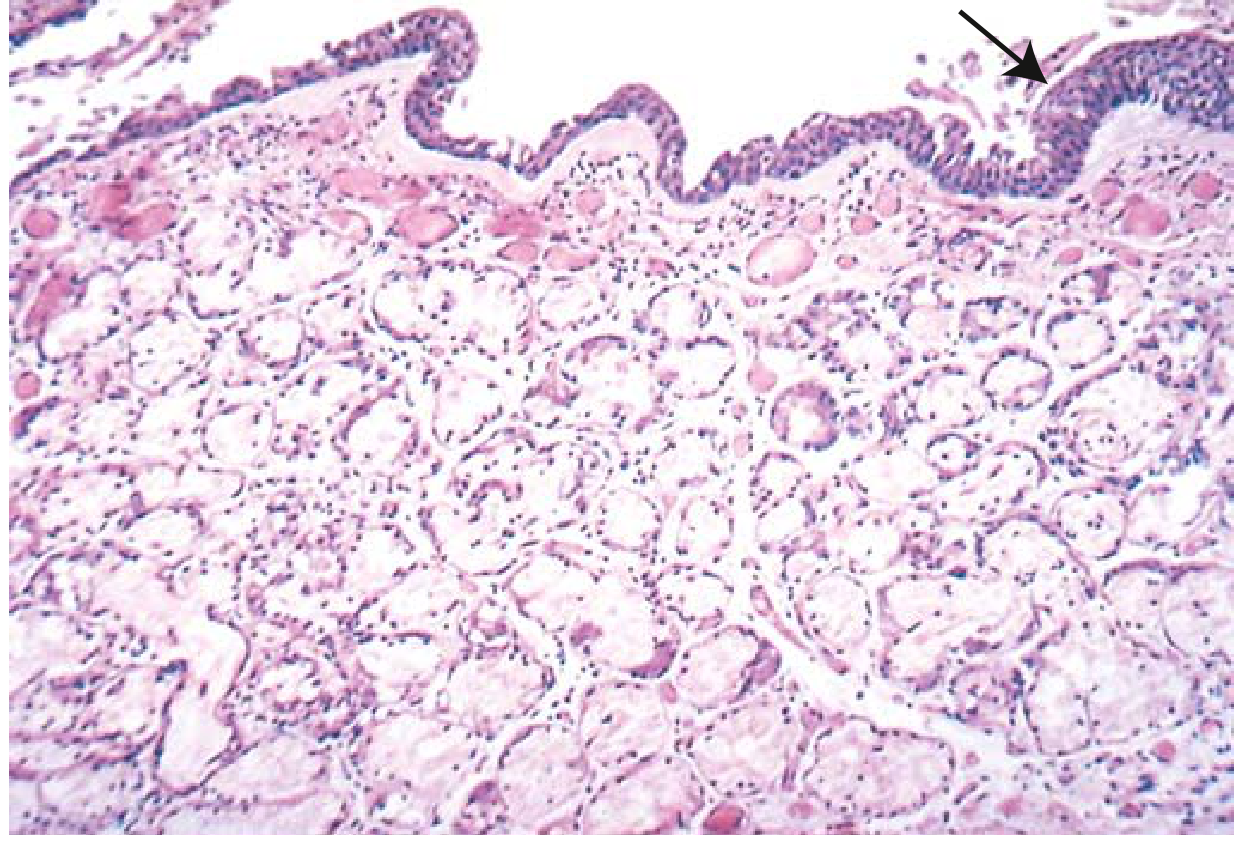
Morphology (Histopathology)
Gross: Hyperemia, swelling, and edema of bronchial mucosa with mucinous or mucopurulent secretions filling airways. Heavy casts of secretions may fill bronchi and bronchioles.
Microscopy:
- Enlargement of mucus-secreting submucosal glands - the diagnostic hallmark
- Reid index (ratio of mucous gland thickness to bronchial wall thickness between epithelium and cartilage): normally ≤0.4; increased in chronic bronchitis, proportional to severity and duration
- Goblet cell hyperplasia in small airways
- Chronic inflammatory infiltrate (lymphocytes and macrophages)
- Smooth muscle hypertrophy and peribronchial fibrosis
- In severe cases: bronchiolitis obliterans (complete obliteration of bronchiolar lumen by fibrosis)
- Robbins & Kumar Basic Pathology, p. 449-450
Clinical Features
Early Stage
- Productive cough - the cardinal symptom; typically worse in the morning and during winter months
- Mucoid sputum, slight at first, increasing over time
- No significant airflow obstruction initially
Progressive Disease
Symptoms wax and wane but are generally progressive:
| Feature | Chronic Bronchitis | Emphysema |
|---|---|---|
| Age (years) | 40-45 | 50-75 |
| Cough | Frequent, early | With exertion, late |
| Sputum | Copious, mucopurulent | Scanty |
| Dyspnea | Mild, late onset | Severe, early onset |
| Infections | Common | Occasional |
| Cor pulmonale | Common (early) | Uncommon (end-stage) |
| Appearance | Cyanotic ("blue bloater") | Well-oxygenated ("pink puffer") |
| Chest X-ray | Prominent vessels, large heart | Hyperinflation, normal heart |
| Airway resistance | Increased | Normal to slightly increased |
| Elastic recoil | Normal | Low |
Table 15.4 - Robbins, Cotran & Kumar Pathologic Basis of Disease; Table 24-2 - Morgan & Mikhail's Clinical Anesthesiology
The "Blue Bloater" Syndrome
The classic presentation of pure chronic bronchitis is the "blue bloater":
- Persistent productive cough with copious sputum
- Hypercapnia (PaCO2 often >40 mm Hg) and hypoxemia
- Mild cyanosis due to V/Q mismatch and intrapulmonary shunting
- Elevated hematocrit (secondary polycythemia from chronic hypoxemia)
- Pulmonary hypertension and cor pulmonale (right ventricular failure) - develops early relative to emphysema
- Edema and ascites when right heart failure supervenes
- Patients are often overweight or obese, which can further impair ventilation, especially during sleep
- Respiratory drive becomes less sensitive to CO2; oxygen therapy can depress ventilation (hypoxic drive dependency)
Complications
-
Recurrent pulmonary infections (viral and bacterial), often with bronchospasm ("asthmatic bronchitis")
-
Acute exacerbations triggered by upper respiratory infections, viral/bacterial pathogens, or environmental pollutant exposure
-
Progressive COPD with irreversible airflow obstruction
-
Pulmonary hypertension and cor pulmonale
-
Respiratory failure
-
Increased risk of lung cancer (especially in smokers: change in cough character or hemoptysis mandates investigation)
-
Obstructive sleep apnea (10-30% of patients)
-
Robbins & Kumar Basic Pathology, p. 450; Morgan and Mikhail's Clinical Anesthesiology 7e, pp. 994-995
Investigations
1. Spirometry (Lung Function Tests) - Most Important
- Diagnostic test of choice for confirming airflow obstruction
- Shows FEV1/FVC ratio < 0.7 (post-bronchodilator) - confirms obstructive pattern
- FEV1 reduced with normal or near-normal FVC
- As disease progresses, the percentage predicted FEV1 is the best measure of severity
- Residual Volume (RV) is increased; Total Lung Capacity (TLC) is often normal (contrast with emphysema where TLC is markedly elevated)
2. Chest X-Ray
- May be normal in early disease - chronic bronchitis is not radiographically apparent unless bronchiectasis is present
- When abnormal: increased bronchovascular (lung) markings, prominent pulmonary vasculature
- Large heart size (right ventricular enlargement from cor pulmonale)
- No significant hyperinflation (contrast with emphysema)
- A chest X-ray is mandatory when there is a change in cough character (e.g., hemoptysis) to exclude lung cancer
3. CT Chest (High-Resolution CT)
- Not routinely needed for diagnosis but useful when CXR is equivocal
- Shows bronchial wall thickening, mucus plugging, and small airway disease
- Distinguishes bronchiectasis (which can look like chronic bronchitis clinically)
- Best method to confirm coexisting emphysema
4. Arterial Blood Gas (ABG) Analysis
- Typically shows type 2 respiratory failure in advanced disease: hypoxemia (low PaO2) + hypercapnia (elevated PaCO2)
- PaO2 < 55 mmHg and/or SaO2 < 88% at rest indicates need for long-term oxygen therapy
- ABG also guides assessment of ventilatory drive
5. Sputum Examination
- Macroscopy: Mucoid (early) to mucopurulent (during exacerbations)
- Microscopy: Neutrophils predominate (eosinophils absent, distinguishing it from asthma)
- Culture and sensitivity: To identify bacterial pathogens in acute exacerbations (common organisms: Haemophilus influenzae, Streptococcus pneumoniae, Moraxella catarrhalis)
6. Complete Blood Count (CBC)
- Polycythemia (elevated hematocrit/red cell mass) - secondary to chronic hypoxemia
- May show leukocytosis during infective exacerbations
7. ECG and Echocardiography
- ECG: May show right ventricular hypertrophy, right axis deviation, P pulmonale (peaked P waves in inferior leads); also detects dysrhythmias
- Echo: Evaluates pulmonary hypertension and right ventricular function (cor pulmonale)
8. B-type Natriuretic Peptide (BNP)
- Useful to differentiate COPD/chronic bronchitis exacerbation from acute left heart failure
- BNP < 100 pg/mL supports COPD as the cause
- BNP > 500 pg/mL suggests acute heart failure
9. Alpha-1 Antitrypsin Level
- Indicated in younger patients (<45 years), non-smokers, or with family history
- Low levels suggest hereditary deficiency (more associated with emphysema, but relevant in the COPD workup)
10. Pulse Oximetry
- Non-invasive continuous monitoring of oxygen saturation
- Useful for identifying hypoxemia and guiding oxygen supplementation
- SaO2 during 6-minute walk test can evaluate exercise-induced desaturation
Summary
Chronic bronchitis is a clinically defined condition (productive cough for 3 months/year for 2 consecutive years) driven primarily by cigarette smoking. Its hallmark pathologic feature is enlargement of mucous glands measured by the Reid index (>0.4). Clinically, the "blue bloater" profile (cyanosis, hypercapnia, cor pulmonale, polycythemia) distinguishes it from emphysema. The most important investigation is spirometry, which confirms obstruction (FEV1/FVC < 0.7); a chest X-ray, ABG, sputum analysis, and CBC complement the workup, with CT chest reserved for complex cases.
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), pp. 449-450
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 637-639
- Morgan and Mikhail's Clinical Anesthesiology, 7e, pp. 994-996
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter on Chronic Bronchitis/COPD
- Tintinalli's Emergency Medicine: A Comprehensive Study, pp. 508-509
Can I get source from... API medicine textbook. Or... Das.
Finding Sources
Finding Sources
Unfortunately, neither the API Textbook of Medicine (by the Association of Physicians of India) nor Das's medicine textbook is currently available in the library. Here's what we do have that's closest:
Available internal medicine / medicine textbooks:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - the gold standard international medicine reference
- Goldman-Cecil Medicine, International Edition (2 volumes) - another major comprehensive medicine text
- Frameworks for Internal Medicine
Also available (already used):
- Robbins & Kumar Basic Pathology
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Murray & Nadel's Textbook of Respiratory Medicine
Would you like me to pull the chronic bronchitis content from Harrison's and/or Goldman-Cecil instead? Those are both highly authoritative medicine textbooks and would give you a clinical perspective very similar to what API Medicine or Das would cover.
Pull chronic bronchitis from Harrison's Internal Medicine (22e)
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the content needed from Harrison's 22e. Here is the complete, sourced response:
Chronic Bronchitis - Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Definition
Chronic bronchitis is a clinically defined condition with chronic cough and phlegm (sputum production). It is one of the three components of COPD, alongside emphysema (anatomically defined by alveolar destruction) and small airway disease (small bronchioles narrowed and reduced in number). Patients with a history of cigarette smoking who have chronic bronchitis but no fixed airflow obstruction on spirometry are not included within the classic COPD definition, but may have identical disease processes.
"COPD includes emphysema, an anatomically defined condition characterized by destruction of the lung alveoli with air space enlargement; chronic bronchitis, a clinically defined condition with chronic cough and phlegm; and/or small airway disease."
- Harrison's, Chapter 303
Pathogenesis and Pathology (Harrison's)
Large Airway Disease (the basis of chronic bronchitis)
Cigarette smoking causes:
- Mucus gland enlargement and goblet cell hyperplasia in large airways - leading to the cough and mucus production that define chronic bronchitis
- Goblet cells increase in number and extend further down the bronchial tree
- Squamous metaplasia of bronchial epithelium - predisposes to carcinogenesis and disrupts mucociliary clearance
- Bronchial hyperreactivity in some patients (though less prominent than in asthma)
- Neutrophil elastase - one of the most potent secretagogues identified; associated with purulent sputum during respiratory tract infections
- Mucus plugs are frequently observed on chest CT scans of COPD patients and have been recently associated with increased mortality risk
Inflammation and Disease Mechanisms
- Cigarette smoke activates alveolar macrophages to release IL-8 and TNF-α, recruiting neutrophils
- CD8+ T cells release IP-10 (CXCL-7), driving macrophage production of MMP-12 (macrophage elastase)
- Matrix metalloproteinases and serine proteinases (notably neutrophil elastase) degrade each other's inhibitors - a destructive positive feedback loop
- Autoimmune mechanisms may promote progression: lymphoid follicles (B + T cells) around airways, IgG autoantibodies against pulmonary epithelium
- Long after smoking cessation, chronic inflammation persists in end-stage disease - suggesting cigarette smoke both initiates and establishes a self-sustaining process
Clinical Presentation (Harrison's)
History - Symptoms
The three most common symptoms in COPD with chronic bronchitis are:
- Cough - often the first symptom; patients usually have symptoms for months or years before seeking medical attention
- Sputum production - mucoid initially, becoming mucopurulent with infections
- Exertional dyspnea - insidious in onset; described as increased effort to breathe, heaviness, air hunger, or gasping
Key points on history:
- Many patients date onset to an acute illness/exacerbation, but a careful history reveals prior chronic respiratory symptoms
- Activities involving arm work at or above shoulder level are particularly difficult
- Activities allowing the patient to brace the arms (e.g., pushing a shopping cart, walking on a treadmill) are better tolerated - use of accessory muscles
- As disease advances: dyspnea on exertion progresses to breathlessness at rest and during basic activities of daily living
- Common comorbidities to screen for: cardiovascular disease, GERD, osteoporosis, frailty, depression, and anxiety
- Validated questionnaires used: COPD Assessment Test (CAT) and Modified Medical Research Council (mMRC) Dyspnea Scale
Physical Examination
Early COPD: Physical examination is entirely normal in early stages.
Advanced disease:
- Prolonged expiratory phase - hallmark auscultatory finding
- Expiratory wheezing
- Signs of hyperinflation: barrel chest, enlarged lung volumes, poor diaphragmatic excursion on percussion
- Use of accessory muscles - sternocleidomastoid, scalene, intercostal muscles; characteristic "tripod" position
- Cyanosis - visible in lips and nail beds (the "blue bloater" phenotype)
- Cachexia - significant weight loss and diffuse loss of subcutaneous adipose tissue; associated with elevated inflammatory cytokines (TNF-α); an independent poor prognostic factor
- Signs of cor pulmonale (right heart failure): lower limb edema - relatively infrequent now with supplemental oxygen therapy, but pulmonary hypertension should be considered with persistent exertion limitations or leg edema
Important: Clubbing of the digits is NOT a sign of COPD. Its presence should prompt investigation for other causes - in a COPD patient, newly developed clubbing most likely indicates lung cancer.
Investigations / Laboratory Findings (Harrison's)
1. Spirometry (Pulmonary Function Tests) - The Hallmark Investigation
- FEV1/FVC < 0.7 (post-bronchodilator) confirms airflow obstruction - the classic COPD diagnostic criterion
- FEV1 reduction indicates severity
- With worsening disease: increased TLC, FRC, and RV (hyperinflation)
- In emphysema-predominant disease: reduced diffusing capacity (DLCO) reflecting alveolar destruction
- Degree of airflow obstruction is an important prognostic factor
GOLD Severity Grading (post-bronchodilator FEV1/FVC < 0.7):
| GOLD Grade | Severity | FEV1 (% predicted) |
|---|---|---|
| GOLD 1 | Mild | ≥ 80% |
| GOLD 2 | Moderate | 50-79% |
| GOLD 3 | Severe | 30-49% |
| GOLD 4 | Very Severe | < 30% |
BODE Index - a better predictor of mortality than FEV1 alone, incorporating:
- Body mass index
- Obstruction (FEV1)
- Dyspnea (mMRC scale)
- Exercise capacity (6-minute walk distance)
2. Arterial Blood Gas (ABG) Analysis
- May show resting or exertional hypoxemia
- Provides information on alveolar ventilation, acid-base status (PaCO2 and pH)
- Hypercapnia (elevated PaCO2) indicates ventilatory failure in advanced disease
- Guides need for long-term oxygen therapy
3. Chest X-Ray
- Chronic bronchitis is not radiographically apparent unless bronchiectasis is present
- May show increased bronchovascular markings, prominent pulmonary vasculature
- In COPD with emphysema: hyperinflation, flat diaphragms, increased lung lucency
4. CT Chest
- Mucus plugs are frequently observed on chest CT and are associated with increased mortality
- Identifies airway wall thickening, airway disease, and extent of emphysema
- Better characterization than plain X-ray for assessing coexisting emphysema or bronchiectasis
5. Pulse Oximetry and Oxygen Assessment
- Non-invasive assessment of resting and exertional hypoxemia
- 6-minute walk test with oximetry quantifies exercise capacity and exercise-induced desaturation
- Guides supplemental oxygen therapy decisions
6. Alpha-1 Antitrypsin (α1-AT) Level
- Indicated especially in patients presenting at younger age, non-smokers, or with family history
- Serum α1-AT level < 11 μM (~55 mg/dL) qualifies for augmentation therapy (relevant primarily in emphysema-predominant disease)
Natural History (Harrison's)
- Most individuals track on quantiles of pulmonary function based on genetics and environment
- COPD can result from:
- Reduced pulmonary function growth during childhood/adolescence followed by normal rate of decline
- Early initiation of decline after normal growth
- Accelerated decline after normal growth (classic pattern)
- Pre-COPD: Substantial CT changes (emphysema, airway wall thickening) can be present with normal FEV1/FVC - these patients are at high risk of progression
- The rate of FEV1 decline is modified by smoking cessation - earlier cessation is more beneficial
- Risk of mortality closely associated with reduced FEV1 and presence of emphysema
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill Medical), Chapter 303 - Chronic Obstructive Pulmonary Disease (Craig P. Hersh, Edwin K. Silverman, Dawn DeMeo)
This is a shared conversation. Sign in to Orris to start your own chat.