Glaucoma in detsil
Reading File
Finding Sources
Searching PubMed
glaucoma diagnosis treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have enough comprehensive information to write a detailed answer. Let me compile everything.
Glaucoma - Detailed Overview
Definition
Glaucoma is a group of conditions sharing a common final pathway: chronic progressive optic neuropathy resulting in characteristic morphological changes at the optic nerve head (ONH) and retinal nerve fibre layer (RNFL), progressive retinal ganglion cell death, and visual field loss. Intraocular pressure (IOP) is the key modifiable risk factor.
- Kanski's Clinical Ophthalmology, 10th ed.
Epidemiology
- Affects 2-3% of people over age 40, but up to 50% may be undiagnosed
- Second leading cause of blindness worldwide
- Primary open-angle glaucoma (POAG) is most common in White, Hispanic/Latino, and Black individuals (especially high prevalence in Black individuals)
- Primary angle-closure glaucoma (PACG) constitutes up to half of all cases globally and is most prevalent in people of Asian descent
- Without treatment, mean rate of progression in high-tension glaucoma (HTG): -1.31 dB/year; in normal-tension glaucoma (NTG): -0.36 dB/year; pseudoexfoliation glaucoma (PXEG): -3.13 dB/year
Aqueous Humor Dynamics (Pathophysiology Basis)
The following diagram from Robbins & Kumar illustrates normal aqueous flow and the two main mechanisms of glaucoma:
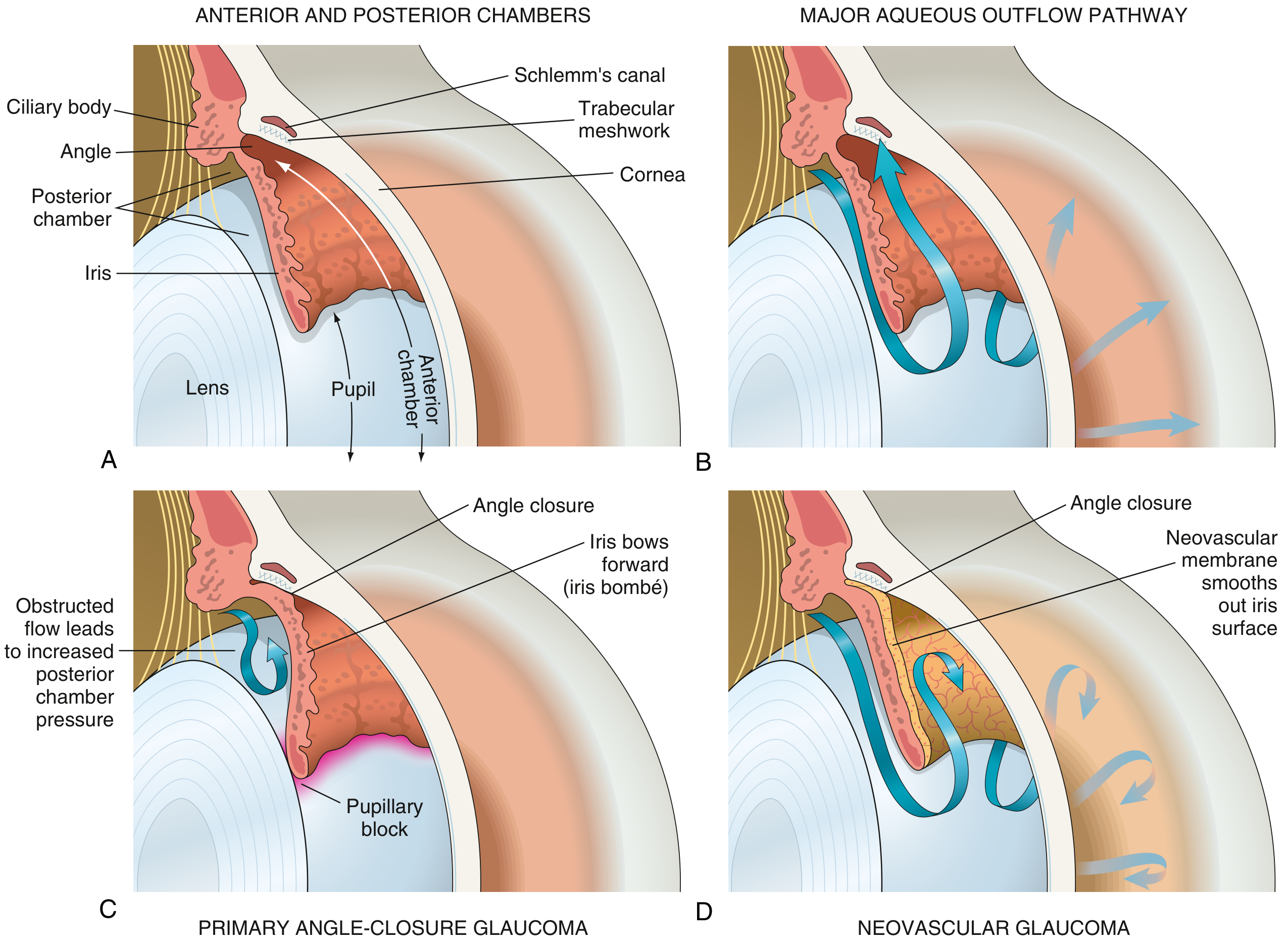
- Aqueous humor is produced by the ciliary body (posterior chamber)
- Flows through the pupil into the anterior chamber
- Drains primarily through the trabecular meshwork into Schlemm's canal
- A secondary uveoscleral pathway accounts for ~10-20% of drainage
Elevated IOP results when production exceeds drainage - either due to blocked outflow (most common) or rarely excess production.
Classification
1. Primary Open-Angle Glaucoma (POAG)
Definition: Chronic, progressive optic neuropathy of adult onset with:
- RNFL thinning
- Glaucomatous optic nerve damage
- Characteristic visual field loss
- Open anterior chamber angle
- No secondary cause
Risk Factors:
- Elevated IOP (most important modifiable risk)
- Family history
- Black/African heritage
- Increasing age
- Thin central corneal thickness (CCT < 555 μm)
- Myopia
- Disc haemorrhage
- Exfoliation syndrome
Subtypes:
- High-tension glaucoma (HTG): IOP consistently > 21 mmHg
- Normal-tension glaucoma (NTG): Glaucomatous damage with IOP within normal range (≤ 21 mmHg); often associated with vascular insufficiency, associated with nocturnal dips in BP
Ocular hypertension (OHT): IOP > 21 mmHg without glaucomatous damage. The OHTS showed untreated patients had a 9.5% cumulative 5-year risk of converting to POAG; treatment reduced this to 4.4%.
2. Primary Angle-Closure Glaucoma (PACG)
Anatomically predisposed eyes (short axial length, shallow anterior chamber, thick lens, plateau iris) develop pupillary block - the iris is pushed against the lens at the pupillary margin, blocking aqueous flow from posterior to anterior chamber. This bows the iris forward (iris bombé) and physically occludes the trabecular meshwork.
Forms:
| Form | Features |
|---|---|
| Acute PACG | Rapid IOP rise, severe ocular pain, nausea/vomiting, blurred vision, halos around lights, fixed mid-dilated pupil, corneal edema |
| Sub-acute (intermittent) | Recurrent mild attacks, spontaneous resolution |
| Chronic | Insidious progression, peripheral anterior synechiae |
Precipitants of acute attack: Dim lighting, emotional stress, mydriatic drugs, reading
Emergency management of acute PACG:
- IV acetazolamide 500 mg
- Topical timolol, pilocarpine, apraclonidine
- Systemic hyperosmotic agents (mannitol) if needed
- Laser peripheral iridotomy (LPI) - definitive treatment; prophylactic LPI to fellow eye
3. Secondary Glaucomas
| Type | Mechanism |
|---|---|
| Pseudoexfoliation (PXF) glaucoma | Exfoliation material clogs trabecular meshwork; highest conversion risk from OHT; responds well to laser treatment |
| Pigmentary glaucoma | Pigment dispersion from iris rubbing against lens zonules; young myopic males |
| Neovascular glaucoma | NV membrane on iris (rubeosis iridis) and angle; caused by ischemia - diabetic retinopathy, CRVO, CRAO |
| Inflammatory (uveitic) glaucoma | Trabecular obstruction by cells/debris, peripheral anterior synechiae (PAS) |
| Steroid-induced glaucoma | Steroids increase trabecular meshwork resistance |
| Phacolytic glaucoma | Lens protein leakage in hypermature cataract |
| Phacomorphic glaucoma | Intumescent (swelling) lens causes pupillary block |
| Traumatic glaucoma | Angle recession, ghost cell glaucoma |
4. Developmental (Congenital) Glaucoma
- Primary congenital glaucoma (PCG): Trabeculodysgenesis; presents with the triad of epiphora, photophobia, blepharospasm; buphthalmos (bull's eye appearance from enlarged globe)
- Sturge-Weber syndrome: Glaucoma in ~30%; ipsilateral to facial haemangioma; mechanism is trabeculodysgenesis (early onset) or raised episcleral venous pressure (later)
- Aniridia: Associated with glaucoma in up to 50-75% of patients; treated with drainage devices
Optic Disc Changes in Glaucoma
Glaucomatous damage results in characteristic changes at three levels:
A. Optic Nerve Head (ONH)
- Pathological cupping - increased cup:disc (C:D) ratio (>0.6 or asymmetry >0.2 between eyes is suspicious)
- Neuroretinal rim (NRR) thinning - follows the ISNT rule normally (Inferior > Superior > Nasal > Temporal); violation = suspicious
- Vertical elongation of cup - often an early sign
- Notching of NRR (most commonly inferior or superior poles)
- Bayoneting of vessels (vessels appear to bend sharply at disc margin)
- Disc haemorrhages (Drance haemorrhages) - splinter-shaped, most common inferotemporal; important risk factor for progression
B. Morphological Disc Subtypes
| Pattern | Features |
|---|---|
| Focal ischaemic | Superior/inferior notching, localized field defects, early fixation threat |
| Myopic glaucoma | Tilted disc, temporal parapapillary atrophy (PPA), dense scotomas |
| Sclerotic | Shallow saucerized cup, sloping NRR, older patients, vascular association |
| Concentrically enlarging | Uniform NRR thinning, diffuse field loss, high IOP |
C. RNFL Changes
- Diffuse loss or localized wedge defects (most commonly superotemporal or inferotemporal)
- Precede visual field defects by months to years
D. Parapapillary Changes
- Alpha zone: Mottled hypopigmentation (not specific)
- Beta zone: Scleral crescent, absent RPE/choriocapillaris (more specific)
- Beta-zone peripapillary atrophy (PPA) is more common and larger in glaucoma
Visual Field Defects
Characteristic visual field losses in glaucoma (central 30° most important):
| Stage | Visual Field Change |
|---|---|
| Early | Isolated paracentral scotoma, nasal step |
| Moderate | Arcuate (Bjerrum) scotoma - arching from blind spot |
| Advanced | Ring scotoma, altitudinal defect |
| Late | Tubular (tunnel) vision with only small central or temporal island remaining |
Goldmann perimetry - kinetic, useful in advanced/non-cooperative patients
Humphrey automated perimetry - static, standard is 24-2 program; 10-2 used for central monitoring in advanced disease
Investigations / Diagnostic Workup
IOP Measurement
- Goldmann applanation tonometry (GAT) - gold standard
- Normal IOP: 10-21 mmHg (mean 15.5 ± 2.5 mmHg)
- IOP is not diagnostic by itself; glaucoma can occur at any IOP
Central corneal thickness (CCT): Thick corneas falsely elevate GAT readings, thin corneas falsely lower them.
- CCT < 555 μm = thin (underestimation of true IOP)
- CCT > 588 μm = thick (overestimation)
- Measure with pachymetry
Gonioscopy
- Essential to classify glaucoma as open-angle vs. angle-closure
- Uses a Goldmann lens or Zeiss 4-mirror lens
- Grades the angle using Shaffer or Spaeth classification
- Identifies peripheral anterior synechiae (PAS), neovascularization, pigment deposition
Optic Disc & RNFL Imaging
| Modality | Details |
|---|---|
| OCT (Optical coherence tomography) | Gold standard for RNFL and ONH analysis; compares to normative database; detects pre-perimetric change |
| HRT (Heidelberg Retinal Tomograph) | 3D ONH imaging; Moorfields regression analysis |
| GDx (Scanning laser polarimetry) | RNFL thickness via birefringence; largely superseded by OCT |
| Fundus photography | Serial stereo disc photos for progression monitoring |
Medical Treatment of Glaucoma
Goal: Reduce IOP to a "target IOP" - a level at which progression is halted or significantly slowed.
Drug Classes (in order of typical use)
| Drug Class | Examples | Mechanism | IOP Reduction | Key Side Effects |
|---|---|---|---|---|
| Prostaglandin analogues (PGA) - 1st line | Latanoprost, travoprost, bimatoprost, tafluprost | Increase uveoscleral outflow via FP receptors | 25-35% | Iris/periorbital hyperpigmentation, hypertrichosis, cystoid macular edema; once daily |
| Beta-blockers | Timolol (non-selective), betaxolol (β1-selective) | Reduce aqueous production via β2 receptor blockade | 20-27% | Bradycardia, bronchospasm, depression; contraindicated in asthma/COPD |
| Alpha-2 agonists | Brimonidine, apraclonidine | Reduce aqueous production + increase uveoscleral outflow | 18-27% | Allergic follicular conjunctivitis, drowsiness, dry mouth |
| Carbonic anhydrase inhibitors (CAI) - Topical | Dorzolamide, brinzolamide | Block CA-II in ciliary epithelium → reduce aqueous secretion | 15-20% | Burning/stinging/metallic taste; brinzolamide better tolerated |
| CAI - Systemic | Acetazolamide (IV/oral), methazolamide | Same mechanism | Significant | Paresthesias, hypokalemia, kidney stones, aplastic anemia (rare) |
| Miotics (cholinergics) | Pilocarpine, echothiophate | Increase trabecular outflow via ciliary muscle contraction | 20-25% | Miosis, brow ache, myopia, cataract; used in PACG |
| Rho kinase inhibitors | Netarsudil | Increase trabecular outflow via Schlemm's canal | 20-25% | Conjunctival hyperemia, cornea verticillata |
| Nitric oxide donors | Latanoprostene bunod | Dual mechanism: PGA + NO-mediated TM relaxation | 25-30% | Similar to PGA |
Step-wise approach:
- Start with PGA once daily (most efficacious, fewest systemic effects)
- Add topical beta-blocker (timolol) if target not met
- Add topical CAI or alpha-2 agonist as third agent
- Consider fixed combinations (e.g., dorzolamide/timolol) to improve adherence
Laser Treatment
| Procedure | Indication | Mechanism |
|---|---|---|
| Selective Laser Trabeculoplasty (SLT) | POAG/OHT, first-line alternative to drops | Q-switched Nd:YAG, selectively targets pigmented TM cells; repeatable |
| Argon Laser Trabeculoplasty (ALT) | POAG | Thermal coagulation of TM; not repeatable |
| Laser Peripheral Iridotomy (LPI) | Angle-closure, prophylaxis in fellow eye | Creates hole in iris, relieves pupillary block |
| Diode laser cycloablation (cyclophotocoagulation, CPC) | Refractory glaucoma | Destroys ciliary body to reduce aqueous production |
| Laser iridoplasty (ALPI) | Plateau iris syndrome | Contracts peripheral iris stroma, opens angle |
Evidence update (2024): A systematic review and meta-analysis of SLT vs. medical therapy for open-angle glaucoma/OHT (J Glaucoma, 2024) found SLT to be a comparable first-line option with equivalent or superior IOP control in many patients (PMID 39018052).
Surgical Treatment
Trabeculectomy (Filtering Surgery)
- Gold standard for surgical IOP reduction
- Creates a controlled fistula (bleb) from anterior chamber to subconjunctival space
- Mitomycin-C (MMC) or 5-FU used to prevent bleb scarring
- Target IOP post-op: 8-12 mmHg
- Complications: Bleb leak, hypotony, infection (blebitis/endophthalmitis), cataract, failure
Glaucoma Drainage Devices (GDDs / Tube Shunts)
- Molteno, Baerveldt, Ahmed valve implants
- Route aqueous to equatorial plate via silicone tube
- Used when trabeculectomy fails or is high-risk
- PreserFlo MicroShunt vs. trabeculectomy was recently reviewed; meta-analysis (2025, Graefes Arch) showed comparable IOP reduction with a favorable safety profile (PMID 39394492)
Minimally Invasive Glaucoma Surgery (MIGS)
- Lower-risk procedures targeting specific outflow pathways
- Examples: iStent (trabecular bypass), Hydrus microstent, GATT (gonioscopy-assisted transluminal trabeculotomy), XEN gel stent, Cypass (withdrawn)
- Best for mild-to-moderate glaucoma; often combined with cataract surgery
- Lower IOP reduction than trabeculectomy but safer profile
Non-penetrating Surgeries
- Deep sclerectomy and Viscocanalostomy - leave thin Descemet membrane window; lower complication rate than trabeculectomy
Normal-Tension Glaucoma (NTG)
- IOP consistently ≤ 21 mmHg, yet characteristic glaucomatous damage occurs
- Pathogenesis: Vascular insufficiency at ONH, impaired autoregulation, mechanical factors, systemic hypotension (especially nocturnal)
- Associations: Raynaud phenomenon, migraines, sleep apnea, cardiovascular disease, disc haemorrhages more common
- Slower progression than HTG (mean -0.36 dB/year)
- Target IOP: 30% reduction below baseline IOP
- Neuroprotection remains experimental
Special Considerations
Glaucoma in Pregnancy
- Most topical drops cross placenta; beta-blockers (risk of neonatal bradycardia/growth restriction), CAIs (teratogenic in animals), alpha-2 agonists (fetal CNS depression)
- Preferred: Topical PGAs should be avoided (uterotonic effects); beta-blockers with caution; laser SLT is preferred non-pharmacological option
Pediatric Glaucoma
- Primary congenital glaucoma: Goniotomy or trabeculotomy as primary surgery; medical treatment usually insufficient
- Buphthalmos: enlarged corneal diameter >13 mm in infant = emergency
Target IOP and Monitoring
- Target IOP is individualized based on baseline IOP, severity of damage, age, and life expectancy
- Example targets: Early disease - reduce by 20-25%; advanced disease - reduce by 30-40%; NTG - reduce by 30%
- Monitoring schedule: Optic disc assessment + VF testing every 6-12 months; OCT RNFL; IOP at each visit
- Pre-perimetric glaucoma: Structural damage (OCT, disc) detectable before VF loss; treat to prevent conversion
Key Mnemonics and Clinical Pearls
- ISNT rule - Normal NRR thickness: Inferior > Superior > Nasal > Temporal; violation is suspicious
- Disc haemorrhage = risk factor for progression; look for it at every slit-lamp exam
- POAG is bilateral but often asymmetric - always compare both eyes
- Glaucoma can progress at normal IOP; IOP is necessary but not sufficient for diagnosis
- "Cupping follows field" - structural damage (RNFL loss) precedes functional loss (VF defect)
- A cup:disc ratio >0.6 or >0.2 asymmetry between eyes warrants further investigation
- Pilocarpine not used in acute PACG until IOP is lowered first (too inflamed iris to respond)
- Always perform gonioscopy before prescribing mydriatics in undiagnosed patients
Sources: Kanski's Clinical Ophthalmology 10th ed. | Robbins & Kumar Basic Pathology | Goodman & Gilman's Pharmacological Basis of Therapeutics 14th ed. | Textbook of Family Medicine | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.