Discuss for me Per abdomen examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching Images
abdominal examination inspection palpation percussion auscultation diagram
I now have rich content from multiple authoritative sources. Let me compile the comprehensive response:
Per Abdomen Examination
Per abdomen (PA) examination is a structured clinical assessment of the abdomen following the four classic steps: Inspection → Auscultation → Percussion → Palpation (IAPP). Auscultation is done before percussion/palpation to avoid altering bowel sounds.
Patient Positioning & Preparation
- Patient lies supine, legs extended, arms resting by the sides
- The entire abdomen must be exposed — from the nipple line to the inguinal ligaments (saphenous openings)
- Examination in good light, preferably daylight
- The patient should be relaxed; a pillow under the knees reduces abdominal wall tension
- The examiner stands to the right of the patient
- Inspect from the side, tangentially, and from each end of the bed
1. INSPECTION
Skin & Subcutaneous Tissue
- Scars: linear scars (healing by first intention) vs. broad/irregular scars (wound infection); note their location to infer previous surgeries
- Erythema: localized redness from hot-water bottle application — marks the site of pain
- Dilated veins:
- Periumbilical (caput medusae) → portal hypertension/obstruction
- Lateral flanks (upward flow) → inferior vena cava obstruction
- To determine direction of flow: compress vein with two index fingers, milk it empty, release one finger at a time — the vein fills rapidly from the direction of flow
- Subcutaneous nodules near umbilicus: may indicate intra-abdominal carcinoma (especially gastric)
- Striae, bruising (Cullen's sign at umbilicus, Grey Turner's sign at flanks in acute pancreatitis)
Umbilicus
- Normally located midway between xiphisternum and symphysis pubis
- Displaced upward → pelvic mass
- Displaced downward → ascites (Tanyol's sign)
- Everted → ascites or large mass
- Tucked in (inverted) → obesity
- Pushed to one side → mass on the contralateral side
Contour of the Abdomen
- Normal: neither retracted nor distended
- Generalised retraction: found in thin/cachectic individuals
- Symmetrical distension — the "5 Fs":
- Fat (obesity): umbilicus deeply inverted
- Fluid (ascites): umbilicus everted, flanks full
- Flatus (gaseous distension): tympanitic
- Faeces (obstruction/constipation)
- Foetus (pregnancy)
- Localised distension: upper abdomen (gastric/hepatic/pancreatic enlargement), lower abdomen (uterine/bladder/colonic mass), right iliac fossa (caecal distension in large bowel obstruction — better seen than felt)
- Visceroptosis: undue protrusion of the lower abdomen when the patient stands
Movement with Respiration
- Restricted or absent movement → peritonitis (the abdomen does not move freely with breathing)
- Visible peristalsis: dilated bowel loops may show visible peristaltic waves — significant of obstruction
- In thin patients, normal aortic pulsation may be visible in the epigastrium
Hernia Orifices
- Inspect the umbilical, epigastric, inguinal, and femoral regions for bulges, especially with coughing
2. AUSCULTATION
Performed before percussion and palpation to avoid disturbing the abdomen.
- Place the stethoscope lightly on the abdomen; listen in more than one quadrant
- Before declaring the abdomen silent, listen for at least 2 minutes
Bowel Sounds
| Character | Significance |
|---|---|
| Normal: intermittent, low-pitched gurgling | Normal intestinal motility |
| High-pitched, tinkling/churring | Mechanical small bowel obstruction (SBO) — peristalsis against a dilated, fluid-filled loop |
| Absent (silent abdomen) | Paralytic ileus, peritonitis |
| Hollow, distant | Toxic megacolon |
| Hyperactive, rushing | Early obstruction or gastroenteritis |
Note: bowel sounds alone are an unreliable sole criterion for obstruction — they must be interpreted alongside other findings.
Vascular Sounds
- Bruit over the aorta (epigastric midline): aortic aneurysm or aortic stenosis
- Renal artery bruit (above the umbilicus, 2 cm lateral): renal artery stenosis (cause of renovascular hypertension)
- Hepatic bruit: hepatocellular carcinoma or alcoholic hepatitis
- Venous hum at the umbilicus (Cruveilhier–Baumgarten sign): portal hypertension with large paraumbilical varices
- Friction rub over the liver or spleen: hepatic/splenic infarction, perihepatitis (Fitz-Hugh–Curtis syndrome)
Stethoscope as a Tender-Detector
A useful technique: while auscultating, gently press the stethoscope head over different areas while watching the patient's face — if tenderness is present, the patient will wince before guarding occurs.
3. PERCUSSION
- Begin with cursory light percussion across all four quadrants to map areas of dullness and tympany
- Dullness = solid/fluid; Tympany = gas
Liver Percussion
- Percuss the upper border of liver dullness (normally at the 5th intercostal space in the midclavicular line)
- Percuss the lower border in the midclavicular line (normally at the right costal margin)
- Normal liver span: 6–12 cm in the midclavicular line
- Loss of liver dullness: free gas under the diaphragm (perforated viscus) — a surgical emergency
Splenic Percussion
- Percuss at the 10th rib posterior to the midaxillary line — splenic dullness is distinct from gastric or colonic tympany
- Traube's space (9th–11th ribs in midaxillary line): normally tympanitic; dullness suggests splenomegaly
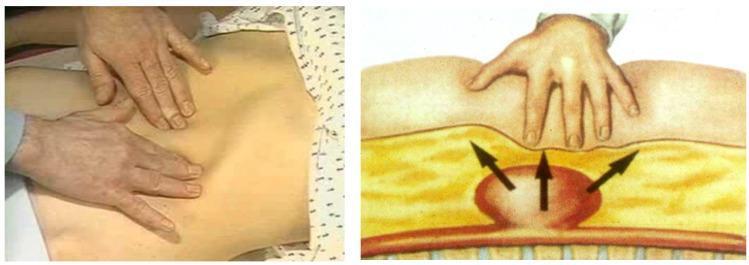
Ascites Detection by Percussion
- Flank dullness: percuss from the umbilicus laterally toward the flank — the note changes from tympany to dullness when fluid is reached; mark the level
- Shifting dullness (most sensitive clinical test): roll the patient to the lateral decubitus position — the dull note shifts downward and the flank becomes resonant (fluid shifts with gravity)
- Fluid thrill (large ascites): place one hand flat on one flank, flick the other flank — a transmitted fluid impulse is felt; ask an assistant to press a hand edge along the midline to block transmission through the abdominal wall fat
Bladder Percussion
- A distended bladder produces dullness in the suprapubic region, obliterating the normal transverse skin crease
Percussion of Masses
- Dull = solid or cystic (no gas)
- Central/umbilical dullness with resonance in flanks = solid mass
- Flanks dull with central tympany = ascites (gas-containing bowel floats centrally)
4. PALPATION
Principles
- Warm hands, short fingernails
- Patient must be relaxed; examiner kneels to the level of the bed
- Begin in the quadrant farthest from the pain and work toward it last
- Light palpation precedes deep palpation
Light Palpation
- Entire abdomen surveyed gently (1–2 cm depth) with fingers together
- Detects:
- Superficial tenderness: the patient winces or tenses
- Guarding (voluntary): patient voluntarily tightens the muscles
- Guarding (involuntary/rigidity): persistent board-like rigidity despite distraction — indicates peritoneal irritation
- Superficial masses: hernias, lipomas, subcutaneous hematomas, lymph nodes
Deep Palpation
- Applies 4–6 cm pressure to palpate deep organs
- The four quadrants are systematically examined
- Identifies: hepatomegaly, splenomegaly, renal masses, abdominal aorta, masses (neoplasm, abscess, lymph nodes)
- Neoplasms (liver, gallbladder, pancreas, stomach, intestine, kidney), abscesses (appendicitis, diverticulitis, Crohn disease), and aortic aneurysms may present as deep masses
Signs of Peritoneal Irritation
| Sign | Technique | Significance |
|---|---|---|
| Rebound tenderness (Blumberg's sign) | Press slowly, release suddenly — pain on release > pressure | Peritonitis |
| Rovsing's sign | Palpate LIF → pain in RIF | Appendicitis |
| Heel-tap / Jar test | Jar the patient's bed or tap the heel | Peritonitis |
| Percussion tenderness | Percussion over a tender area | More specific than rebound for peritonitis |
Palpation of Specific Organs
Liver
- Begin at the right iliac fossa, move toward the costal margin with each inspiration
- Liver edge descends during deep inspiration — felt as a ridge under the fingers
- Note: size (cm below costal margin in MCL), surface texture (smooth vs nodular), edge (sharp vs rounded), consistency (soft, firm, hard), tenderness
- Causes of hepatomegaly: CCF, viral hepatitis, cirrhosis (early), hepatocellular carcinoma, secondaries, malaria, leukaemia, lymphoma
Spleen
- Begin at the RIF (as massive splenomegaly reaches to the RIF)
- Palpate diagonally toward the left costal margin with each inspiration
- Support the left costal margin with the left hand; palpate below the costal margin with the right
- Cannot get above the splenic edge (differentiates from renal mass); has a notch on the medial border; dull to percussion
- Causes of splenomegaly: malaria, portal hypertension, haematological malignancies, infections (EBV, typhoid), haemolytic anaemias
Kidneys (Bimanual)
- Right kidney: right hand in the right loin posteriorly, left hand anteriorly in the right flank
- Can "ballot" the kidney between both hands — ballottement is characteristic of a renal mass
- Key features distinguishing kidney from spleen: can get above the renal mass, resonant to percussion (bowel in front), ballottable, moves with respiration but descends vertically (not diagonally)
Gallbladder
- Palpated below the liver edge at the tip of the 9th costal cartilage (lateral to the MCL)
- Murphy's sign: press under the right costal margin in the MCL; ask patient to inspire deeply — sharp arrest of inspiration due to pain as the inflamed gallbladder descends onto the examining fingers → positive in acute cholecystitis
- Courvoisier's law: a palpable, non-tender gallbladder with jaundice suggests malignant biliary obstruction (not gallstones, which cause a fibrotic, non-distensible gallbladder)
Aorta
- Palpated in the epigastric/para-umbilical region
- Normal aortic pulsation is palpable but narrow
- An expansile pulsatile mass (pulsation in all directions) suggests aortic aneurysm (>3 cm)
- Transmitted pulsation (e.g., from a mass overlying the aorta) pulsates only in one direction
Urinary Bladder
- A distended bladder is a smooth, rounded, dull, midline swelling arising from the pelvis
- May be palpable up to the umbilicus or beyond in chronic retention
5. SPECIAL EXAMINATION
Inguinal/Femoral Regions
- Inspect and palpate the inguinal canal and femoral ring for hernias (ask the patient to cough)
- Examine the external genitalia in males: scrotum, testes, epididymis, vas deferens
Rectal/Pelvic Examination
- Digital rectal examination (DRE) is part of a complete abdominal exam when indicated
- Allows palpation of rectal masses, cervix, pouch of Douglas, prostate, and stool character
- Inspect perianal region: fissures, fistulas, hemorrhoids, skin tags
External Genitalia
- Examine in all patients with acute abdominal pain or urological symptoms
Summary: Sequence of Findings and Their Clinical Significance
| Finding | Interpretation |
|---|---|
| Board-like rigidity | Peritonitis (perforated viscus, ruptured aneurysm) |
| Shifting dullness | Ascites |
| Caput medusae + splenomegaly | Portal hypertension |
| Murphy's sign | Acute cholecystitis |
| Courvoisier's gallbladder | Malignant biliary obstruction |
| Expansile aortic pulsation | Abdominal aortic aneurysm |
| Absent bowel sounds | Paralytic ileus or peritonitis |
| Rovsing's sign | Appendicitis |
| Visible peristalsis | Bowel obstruction |
| Sister Mary Joseph nodule | Intra-abdominal malignancy (umbilical metastasis) |
Illustrative Images
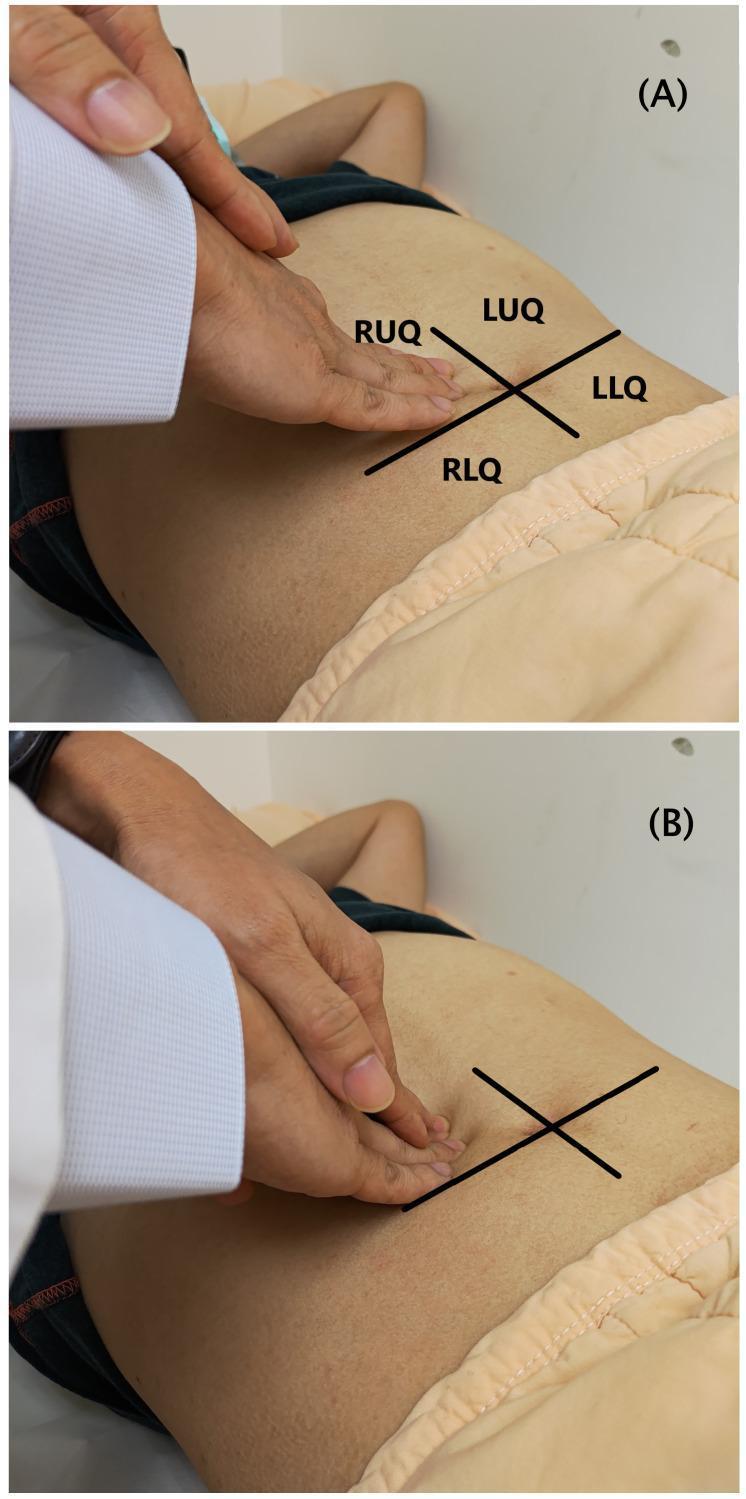
Light palpation (A) vs deep palpation (B) — note the four-quadrant scheme and hand positions
Percussion technique for shifting dullness in suspected ascites
Bimanual palpation in the mesogastrium for expansile pulsation of an abdominal aortic aneurysm
Sources: S Das: A Manual on Clinical Surgery, 13th Ed.; Goldman-Cecil Medicine, International Ed.; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Bailey & Love's Short Practice of Surgery, 28th Ed.
Discuss necrotizing fascitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
necrotizing fasciitis clinical appearance skin necrosis gangrene
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full discussion:
Necrotizing Fasciitis
Definition
Necrotizing fasciitis (NF) is a rare, rapidly progressive, life-threatening infection of the deep subcutaneous tissues and fascia, characterized by extensive and rapidly spreading necrosis (gangrene) of the skin and underlying structures. It tracks down to and spreads rapidly along the fascial plane, with secondary ischemia of the overlying skin. Without prompt diagnosis and intervention, it carries high mortality.
The term was introduced by Wilson (1951–52) to encompass both gas-forming and non-gas-forming necrotizing soft-tissue infections along the fascial plane. Earlier names included "hospital gangrene" (Joseph Jones, 1871), "streptococcal gangrene," and "hemolytic streptococcal gangrene."
Epidemiology
- In the US: approximately 3,800–5,800 admissions/year for necrotizing soft-tissue infections
- Incidence: ~59–76 cases per million patient-years
- Deaths from NF (US, 2003–2013): ~4.8 deaths per million patient-years
- Higher mortality in Black, Hispanic, and Native American individuals
- Pediatric prevalence: ~0.8 per million patient-years (worldwide, 2010–2015)
- Peaks in the neonatal period and in children aged 1–2 years (truncal, often monomicrobial)
Etiology & Pathogenesis
Portal of Entry
- Most cases are community-acquired via breaks in the skin: cuts, scrapes, minor trauma, insect bites, animal bites, IV drug injection sites, prior surgical sites, varicella lesions, burns
- In ~50% of cases, no portal of entry is identified ("cryptic" NF) — infection begins in deep tissues at sites of muscle strain, bruise, or nonpenetrating trauma
- In tropical climates: snake bites (notably Naja atra)
Microbial Mechanism
Once bacteria are introduced, they exploit devitalized tissue to proliferate along the fascial plane — a plane with relatively poor blood supply and immune surveillance. Two processes drive the destruction:
- Polymicrobial synergy: Facultative gram-negative organisms lower the oxidation-reduction potential of tissue, enabling anaerobic growth. Anaerobes, in turn, impede phagocyte function and favour aerobic proliferation.
- Toxin-mediated injury: Clostridial alpha-toxin causes tissue necrosis and cardiovascular collapse. S. aureus and streptococci produce exotoxins triggering TNF and cytokine release → SIRS → septic shock → multi-organ failure.
Thrombosis of the capillary beds feeding the overlying skin occurs as the infection spreads, causing ischemia and necrosis. Because thrombosis must occur before skin changes appear, early infection has little overlying skin change — explaining the frequently delayed diagnosis.
Classification
Microbiologic Types
| Type | Organisms | Features |
|---|---|---|
| Type I (Polymicrobial) | ≥1 anaerobic species + facultative anaerobic streptococci (non-Group A) + Enterobacteriaceae | Most common (~60%); typically occurs in diabetics, immunocompromised, post-surgical patients |
| Type II (Monomicrobial) | Group A Streptococcus (S. pyogenes) ± Staphylococcus aureus | ~40%; any age; healthy individuals; associated with streptococcal toxic shock syndrome |
| Type III | Vibrio spp. (V. vulnificus) | Marine exposure; puncture wounds from fish/marine organisms; increased in Asia/Australia; fulminant course |
| Type IV | Candida spp. | Very rare; immunocompromised hosts |
The simpler classification — polymicrobial vs. monomicrobial — is most widely used in current literature.
Anatomic Variants
- Cervicofacial/Craniofacial NF: spread from odontogenic infections, peritonsillar abscesses — high mortality given proximity to airway
- Perineal/Genital (Fournier's Gangrene): NF of the perineum, scrotum, and penis; urological/colorectal source; polymicrobial; extremely destructive
- Truncal NF: includes abdominal wall; neonatal NF most frequently involves the abdominal wall and has higher mortality than adult NF
- Limb NF: extremities are most commonly involved; amputation may be required
Clinical Features
Early Signs
- Pain out of proportion to clinical findings — the most important early clue; tenderness extends beyond the area of visible erythema
- Erythema, swelling, warmth, and tenderness spreading rapidly both proximally and distally within 24 hours
- Brawny (woody) oedema of the skin
- Systemic: low-grade fever, tachycardia out of proportion to fever, anxiety, diaphoresis
Progression (24–96 hours)
- Erythema darkens from red → purple → blue
- Appearance of blisters and bullae containing clear yellow or later dark purple/haemorrhagic fluid
- Crepitus (surgical emphysema): caused by gas-producing organisms — present in only 13–31% of patients; its absence does NOT rule out NF
- Skin anaesthesia: characteristic — results from thrombosis of cutaneous nerves and vessels; a dangerous sign of deep necrosis
- Bacteraemia with possible metastatic abscesses
Late Signs (Day 4–5 onwards)
- Frank gangrene of affected skin — black necrotic eschars
- Malodorous serosanguineous ("dishwater") discharge
- Extensive sloughing of skin
- Systemic: septic shock, cardiovascular collapse (especially with V. vulnificus and streptococcal TSS), multi-organ failure, confusion, rapid deterioration of consciousness
Key early warning triad: (1) pain out of proportion, (2) swelling/erythema with brawny oedema, (3) systemic toxicity.
Clinical Photograph

Necrotizing soft-tissue infection: central pale necrosis with surrounding hyperaemia and oedema. Rapid tissue loss mandates emergency surgical intervention.

Fournier's gangrene: perineal and scrotal NF with areas of frank necrosis, slough, and surrounding inflammation — a urological emergency.

Large haemorrhagic bullae on the leg — a late sign of necrotizing fasciitis indicating vascular compromise of the overlying skin.
Diagnosis
Diagnosis is primarily clinical. One or more "hard" signs (crepitus, skin necrosis, bullae, hypotension, gas on plain X-ray) are present in fewer than half of patients at presentation, making early diagnosis challenging.
Bedside Test (Finger Test)
Infiltrate the site with local anaesthetic, make a 2-cm incision down to the fascia, and probe with a finger:
- Lack of bleeding
- Murky "dishwater" discharge
- No resistance to probing (tissue planes dissect easily — the fascial layer separates without resistance)
These three findings are ominous and diagnostic of NF. A biopsy from normal-appearing tissue at the necrotic zone edge should be taken.
Laboratory: LRINEC Score
The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) helps distinguish NF from other severe soft-tissue infections:
| Parameter | Range | Points |
|---|---|---|
| CRP | ≥150 mg/L | 4 |
| WBC | 15–25 × 10³/µL | 1 |
| >25 × 10³/µL | 2 | |
| Haemoglobin | 11–13.5 g/dL | 1 |
| <11 g/dL | 2 | |
| Sodium | <135 mEq/L | 2 |
| Creatinine | >1.6 mg/dL | 2 |
| Glucose | >180 mg/dL | 1 |
Interpretation:
- ≤5: low risk (<50%)
- 6–7: intermediate — raises suspicion
- ≥8: high risk (>75% probability)
⚠️ Important limitation: The LRINEC score ≥6 misses many cases, especially Vibrio infections and cervical NF. Clinical suspicion must always override a low LRINEC score. The score is a screening aid, not a diagnostic criterion.
Imaging
| Modality | Findings | Notes |
|---|---|---|
| Plain X-ray | Gas tracking along fascial planes | Present only ~25–50% of cases |
| CT scan | Fascial thickening, asymmetric fascial enhancement, gas in soft tissues, fluid tracking along fascial planes | Fast, widely available; good for extent |
| MRI | Most definitive non-invasive test; shows fluid and inflammation along fascial planes with T2 hyperintensity | Best for soft-tissue detail; time-consuming |
Crucially, even MRI and CT do not definitively exclude NF — a normal imaging study does not rule out the diagnosis if clinical suspicion is high. Surgical exploration remains the gold standard.
Histopathology (Biopsy/Frozen Section)
- Necrosis of fascia and subcutaneous fat
- Polymorphonuclear infiltrate
- Thrombosis of vessels in the subcutaneous tissue
- Gram stain of aspirated fluid: chains of gram-positive cocci with few or no WBCs (in Group A Strep cryptic NF)
Differential Diagnosis
- Severe cellulitis (no fascial involvement, no systemic toxicity)
- Gas gangrene / clostridial myonecrosis (muscle involved, crepitus marked)
- Pyomyositis (abscess in muscle belly, fascia usually spared)
- Trauma with haematoma formation
- Neutrophilic dermatoses (Sweet's syndrome)
- Deep vein thrombosis / phlebitis
- Bursitis
Management
Resuscitation
- Aggressive IV fluid resuscitation — NF lesions drain large volumes
- Close monitoring of vitals, electrolytes, urine output
- ICU admission for haemodynamically unstable patients
1. Surgical Debridement — The Cornerstone
- Radical surgical debridement is the mainstay of treatment — antibiotics alone are insufficient
- Surgical intervention within 24 hours of onset is strongly associated with improved outcomes; delays beyond 24 hours significantly increase mortality
- Debridement must be staged and daily — a single debridement rarely achieves full clearance; daily returns to theatre until no further necrotic tissue is found on surgical exploration
- Amputation may be necessary for severe limb disease; risk is higher in diabetic patients
- Wound closure after final debridement: vacuum-assisted closure (VAC) devices then split-thickness skin grafting
2. Antibiotics (Adjunctive but Crucial)
Broad-spectrum empirical therapy while awaiting cultures; narrow based on tissue culture from biopsy or surgical debridement.
IDSA 2014 Guidelines (empirical):
- Anti-MRSA agent: Vancomycin OR Linezolid OR Daptomycin
- PLUS one of:
- Piperacillin-tazobactam
- Carbapenem (imipenem/meropenem)
- Ceftriaxone + metronidazole
- Fluoroquinolone + metronidazole
For confirmed Group A Strep (Type II):
- Penicillin G + Clindamycin (clindamycin suppresses toxin production via ribosomal inhibition even at static doses)
Continue antibiotics until:
- Final surgical debridement completed
- Afebrile for 48–72 hours
- Clinical stabilization
3. Supportive Care
- Aggressive resuscitation, vasopressors if required
- Blood products for coagulopathy / severe anaemia
- Nutritional support (high protein for wound healing)
4. Hyperbaric Oxygen (HBO)
- Insufficient evidence to support routine use
- Some studies suggest potential benefit; research ongoing — not recommended as first-line
5. IV Immunoglobulin (IVIG)
- Early studies showed some benefit, particularly in streptococcal TSS complicating NF
- No strong evidence to support routine use in NF
Prognosis & Prognostic Factors
Mortality: 20–40% even in optimal circumstances (some studies quote up to 70% with delayed treatment).
Poor prognostic factors:
- Age >50 years
- Underlying diabetes mellitus or atherosclerosis
- Delay in diagnosis and surgical intervention >7 days
- Infection involving the trunk (vs. extremities)
- Haemodynamic instability / septic shock at presentation
- Vibrio vulnificus or polymicrobial infection
- Neonatal NF (higher mortality than adult)
Morbidity:
- Amputation (common with limb disease, especially in diabetics)
- Prolonged hospital course with repeated operations
- Extensive skin grafting requirements
- Long, laborious recovery process following discharge
Summary Table
| Feature | Key Point |
|---|---|
| Pathology | Rapid necrosis tracking along fascial plane; thrombosis of dermal vessels → skin ischemia |
| Commonest type | Type I (polymicrobial, ~60%) |
| Most dangerous | Type II (Group A Strep + TSS) and Type III (Vibrio) |
| Earliest clue | Pain out of proportion to findings |
| Pathognomonic sign | Finger test: no bleeding, dishwater fluid, no tissue resistance |
| Best imaging | MRI (but don't let imaging delay surgery) |
| Lab score | LRINEC (use cautiously — low sensitivity) |
| Treatment principle | Surgery first, antibiotics second |
| Antibiotic backbone | Anti-MRSA + piperacillin-tazobactam/carbapenem |
| Mortality | ~20–40%; greatly reduced with surgery <24 h |
Sources: Fitzpatrick's Dermatology, 9th Ed.; Andrews' Diseases of the Skin, Clinical Dermatology; Goldman-Cecil Medicine, International Ed.; Tintinalli's Emergency Medicine: A Comprehensive Study; Dermatology 2-Volume Set, 5th Ed.
Discuss appendicitis
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.