Latest management of coronary artery disease
Reading File
Finding Sources
Searching PubMed
"coronary artery disease" AND management
Searching the Web
coronary artery disease management guidelines 2024 2025
Finding Sources
Reading Article
PMID: 40014670
Reading Article
PMID: 39210710
Reading Web Page
https://touchcardio.com/cardiovascular-disease/conference-hu…
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, guideline-based overview of the latest management of coronary artery disease (CAD), covering both chronic coronary syndromes (CCS) and acute coronary syndromes (ACS), drawing from Fuster and Hurst's The Heart (15th ed.), the 2023 AHA/ACC Chronic Coronary Disease Guideline, the 2024 ESC Guidelines for CCS, and the 2025 ACC/AHA ACS Guideline.
Latest Management of Coronary Artery Disease
CAD encompasses a spectrum from stable/chronic disease to acute presentations (unstable angina, NSTEMI, STEMI). Management is goal-directed, aiming to: (1) prevent death and MI, and (2) reduce ischemic symptoms. The intensity of treatment is scaled to the magnitude of risk and ischemic burden.
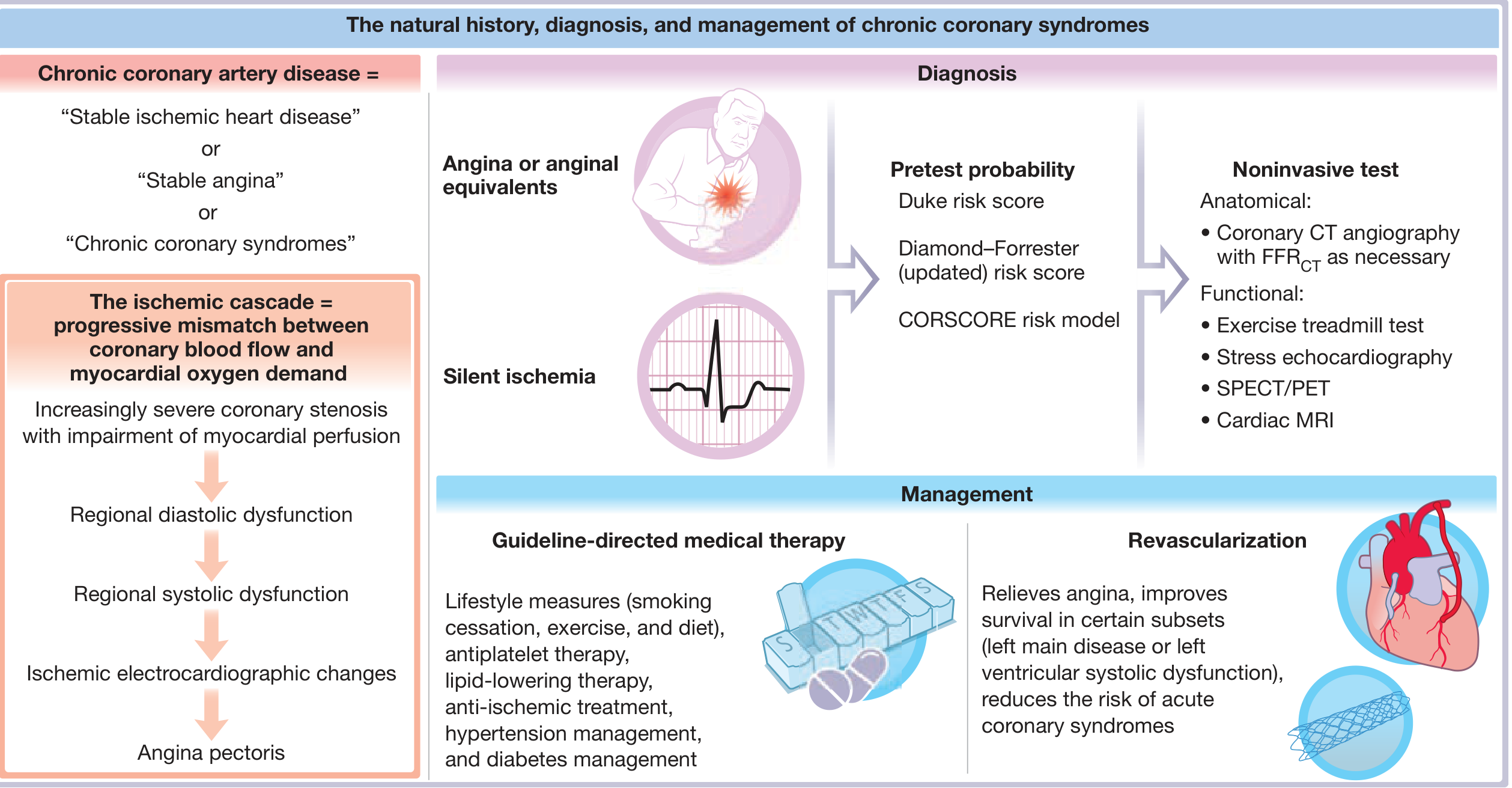
Part 1: Chronic Coronary Syndromes (CCS) / Stable CAD
1. Lifestyle Measures (Class I)
- Physical activity: 30-60 minutes of moderate-intensity aerobic exercise (e.g. brisk walking) 5-7 days/week. Cardiac rehabilitation reduces cardiovascular mortality by ~26% and hospital admissions by ~18% vs. usual care (meta-analysis of 63 RCTs, n=14,486).
- Diet: Replace saturated/trans fats with unsaturated fats; reduce dietary cholesterol; add plant stanols/sterols (2 g/day) and soluble fiber (>10 g/day).
- Smoking cessation: Mandatory - both non-pharmacological and pharmacological support.
- Weight management: Avoid excessive weight fluctuations, which are independently harmful in CAD.
- Alcohol: Moderate consumption; avoid marijuana and air pollution.
- Depression screening: Escitalopram treatment after recent ACS with depression reduced MACE in a randomized trial.
- Fuster and Hurst's The Heart, 15th Edition
2. Pharmacological Therapy - Secondary Prevention
Antiplatelet Therapy
- Aspirin 75-162 mg/day: Class I for all CCS patients. Reduces major vascular events, MI (RR 0.69), and stroke (RR 0.81) vs. placebo (16 RCTs, ~17,000 patients).
- Dual antiplatelet therapy (DAPT): Low-dose aspirin + P2Y12 inhibitor maintained after PCI. Duration varies: typically 6-12 months post-PCI; may be shortened for high bleeding risk or extended for high ischemic risk.
- Newer P2Y12 inhibitors (ticagrelor, prasugrel) are preferred over clopidogrel in high-risk settings (Class I, 2025 ACC/AHA ACS Guideline).
Lipid-Lowering Therapy
- High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg): Class I for all CCS patients, regardless of baseline LDL. Target LDL-C <55 mg/dL (1.4 mmol/L) with ≥50% reduction from baseline (2024 ESC CCS Guideline).
- Add-on non-statin therapy (2025 ACC/AHA ACS update, Class I): If LDL-C remains ≥70 mg/dL on maximally tolerated statin:
- Ezetimibe (Class I)
- PCSK9 inhibitors (evolocumab, alirocumab) - Class I for very high risk with inadequate LDL control on statin + ezetimibe
- Inclisiran (siRNA, newer agent) - emerging option
Beta-Blockers
- Class I for all patients with prior MI or LV systolic dysfunction (EF ≤40%). Reduce heart rate, myocardial oxygen demand, and arrhythmia risk.
- In CCS without prior MI or LV dysfunction: primarily used for symptom control of angina.
- Target resting heart rate 55-60 bpm in angina.
Renin-Angiotensin-Aldosterone System (RAAS) Inhibitors
- ACE inhibitors (or ARBs if ACE-I intolerant): Class I for all CCS patients with LV EF ≤40%, hypertension, or diabetes.
- Perindopril, ramipril, and lisinopril have the strongest evidence in CAD.
Nitrates
- Sublingual nitroglycerin: Immediate relief of acute angina attacks (Class I).
- Long-acting nitrates: For angina prophylaxis; tolerance develops - nitrate-free intervals required.
Calcium Channel Blockers (CCBs)
- Amlodipine or diltiazem: First-line anti-anginal when beta-blockers are contraindicated or insufficient. Vasospastic (Prinzmetal) angina: CCBs are the cornerstone treatment.
Ranolazine
- Late sodium channel blocker; reduces anginal episodes when standard anti-anginals are inadequate. Does not affect heart rate or blood pressure. Particularly useful in patients where HR-lowering agents are not tolerated.
Ivabradine
- Selectively reduces heart rate via If channel inhibition. Used in CCS with EF ≤35% who remain symptomatic on maximally tolerated beta-blockers (Class IIa).
Influenza Vaccination
- Recommended annually in all CCS patients (Class I, 2023 AHA/ACC CCD Guideline) - reduces risk of cardiovascular events.
3. Revascularization in Stable CAD
| Indication | Preferred Strategy |
|---|---|
| Left main disease (SYNTAX ≤22) | PCI or CABG (equivalent outcomes) |
| Left main disease (SYNTAX ≥33) | CABG preferred |
| 3-vessel CAD with complex anatomy (high SYNTAX) | CABG preferred (survival benefit) |
| 3-vessel CAD with low SYNTAX score | PCI is reasonable |
| LV dysfunction (EF <35%) + multivessel CAD | CABG preferred |
| Single/double vessel CAD, proximal LAD | PCI or CABG |
Key principle: In stable CAD, revascularization (PCI or CABG) relieves angina and reduces the risk of future ACS, but does not confer a survival advantage over optimal medical therapy (OMT) in most stable patients without high-risk anatomy (ISCHEMIA trial). Intracoronary imaging (IVUS or OCT) is now a Class I recommendation for left main and complex PCI lesions (2025 ACC/AHA ACS Guideline; also Class I in 2024 ESC Guidelines).
Part 2: Acute Coronary Syndromes (ACS) - 2025 ACC/AHA Updates
The 2025 ACC/AHA/ACEP/NAEMSP/SCAI ACS Guideline (PMID 40014670) - published in Circulation, April 2025 - is the most current unified guideline covering both STEMI and NSTEMI/UA in a single document, replacing guidelines dating back to 2013-2014.
Initial Evaluation and Risk Stratification
- 12-lead ECG within 10 minutes of first medical contact.
- High-sensitivity troponin for rapid rule-in/rule-out (0h/1h or 0h/2h algorithms).
- Risk scores: TIMI, GRACE for NSTEMI; guides invasive timing.
Antiplatelet and Antithrombotic Therapy (ACS)
| Agent | Recommendation |
|---|---|
| Aspirin (162-325 mg loading, then 81 mg/day) | Class I for all ACS |
| Ticagrelor (180 mg load, 90 mg BID) | Class I - preferred over clopidogrel for PCI |
| Prasugrel (60 mg load, 10 mg/day) | Class I - preferred over clopidogrel for PCI |
| Clopidogrel | Class I when newer agents unavailable/contraindicated |
| Upstream clopidogrel or ticagrelor | Class IIb - if angiography anticipated >24h for NSTEMI |
| Anticoagulation (UFH, bivalirudin, enoxaparin, fondaparinux) | Class I - type guided by strategy and bleeding risk |
Reperfusion for STEMI
- Primary PCI: Preferred if door-to-balloon ≤90 min (or ≤120 min if transferred). Class I.
- Fibrinolysis: When PCI unavailable within 120 min of first medical contact. Immediate transfer for rescue PCI if fibrinolysis fails.
- Complete revascularization: Now Class I - treat significant non-culprit stenoses (can be same procedure or staged). Single-procedure multivessel PCI is slightly preferred for STEMI.
- Manual aspiration thrombectomy: Class III (no benefit - should NOT be performed routinely).
Cardiogenic Shock
- Emergency PCI of the culprit vessel: Class I.
- Routine PCI of non-infarct arteries at time of primary PCI in cardiogenic shock: Class III (not recommended).
- Mechanical circulatory support (MCS): Guidance updated; intra-aortic balloon pump, Impella, VA-ECMO considered based on patient hemodynamics.
NSTEMI - Invasive Strategy Timing
- Immediate invasive (<2h): Refractory angina, hemodynamic instability, electrical instability.
- Early invasive (<24h): GRACE score >140, troponin rise, dynamic ST changes.
- Elective invasive (24-72h): Intermediate risk NSTEMI.
- Conservative strategy: Elderly, high bleeding risk, stable low-risk NSTEMI.
Long-Term/Discharge Therapies After ACS
| Drug Class | Recommendation |
|---|---|
| Aspirin 81 mg lifelong | Class I |
| P2Y12 inhibitor (ticagrelor or prasugrel) x 12 months | Class I post-PCI |
| High-intensity statin | Class I |
| Add ezetimibe if LDL ≥70 mg/dL on statin | Class I (new 2025 ACS update) |
| Add PCSK9 inhibitor if LDL still ≥70 mg/dL | Class I |
| Beta-blocker (EF ≤40% or prior MI) | Class I |
| ACE inhibitor/ARB (EF ≤40%, HTN, DM) | Class I |
| Aldosterone antagonist (EF ≤35% + HF or DM) | Class I |
| Colchicine 0.5 mg/day | Class IIa (anti-inflammatory; LoDoCo2 trial) |
Part 3: Special Populations
| Population | Key Considerations |
|---|---|
| Diabetes | SGLT2 inhibitors (empagliflozin, dapagliflozin) and GLP-1 agonists (semaglutide, liraglutide) reduce MACE and are now integral to CAD management with T2DM |
| CKD | Dose-adjust antiplatelet and anticoagulant therapy; ezetimibe preferred over statins for GFR <30; avoid NSAIDs |
| Elderly | Weigh bleeding vs. ischemic risk; shorter DAPT; radial artery access for PCI |
| Women | INOCA (ischemia with no obstructive CAD) more common; consider coronary vasomotion testing |
Summary of Key 2024-2025 Guideline Updates
- Unified STEMI+NSTEMI guideline - first time both ACS types in a single ACC/AHA document (2025).
- Intracoronary imaging (IVUS/OCT) upgraded to Class I for left main and complex PCI lesions.
- LDL targets more aggressive: Statin + ezetimibe (Class I) if LDL ≥70 on statin; PCSK9i if still elevated.
- Complete revascularization in STEMI/NSTEMI now Class I.
- Ticagrelor/prasugrel preferred over clopidogrel (Class I) for PCI.
- SGLT2 inhibitors and GLP-1 agonists are integral to CAD management in diabetics.
- Colchicine (anti-inflammatory therapy) has Class IIa evidence post-MI.
- Aspiration thrombectomy remains Class III - no benefit.
Key References:
- 2025 ACC/AHA ACS Guideline (Rao et al., Circulation 2025 - PMID 40014670)
- 2024 ESC Guidelines for Chronic Coronary Syndromes (Vrints et al., Eur Heart J 2024 - PMID 39210710)
- 2023 AHA/ACC Guideline for Chronic Coronary Disease (Virani et al., Circulation 2023 - PMID 37471501)
- Fuster and Hurst's The Heart, 15th Edition - Chapter 21 (Stable Ischemic Heart Disease)
This is a shared conversation. Sign in to Orris to start your own chat.