What happened when one of the twins dies in pregnancy?how to identify and how to treat
Reading File
Finding Sources
Finding Sources
Searching PubMed
"single fetal demise" AND "twin pregnancy" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer.
Death of One Twin During Pregnancy (Single Intrauterine Fetal Demise - sIUFD)
When one twin dies in utero, the consequences for the surviving fetus, the mother, and the management plan depend heavily on when the death occurs and, most critically, chorionicity (whether the twins share a placenta).
1. Terminology
| Term | Meaning |
|---|---|
| Vanishing twin syndrome | Spontaneous loss of one embryo/fetus in the first trimester; the lost twin "vanishes" without leaving visible remains |
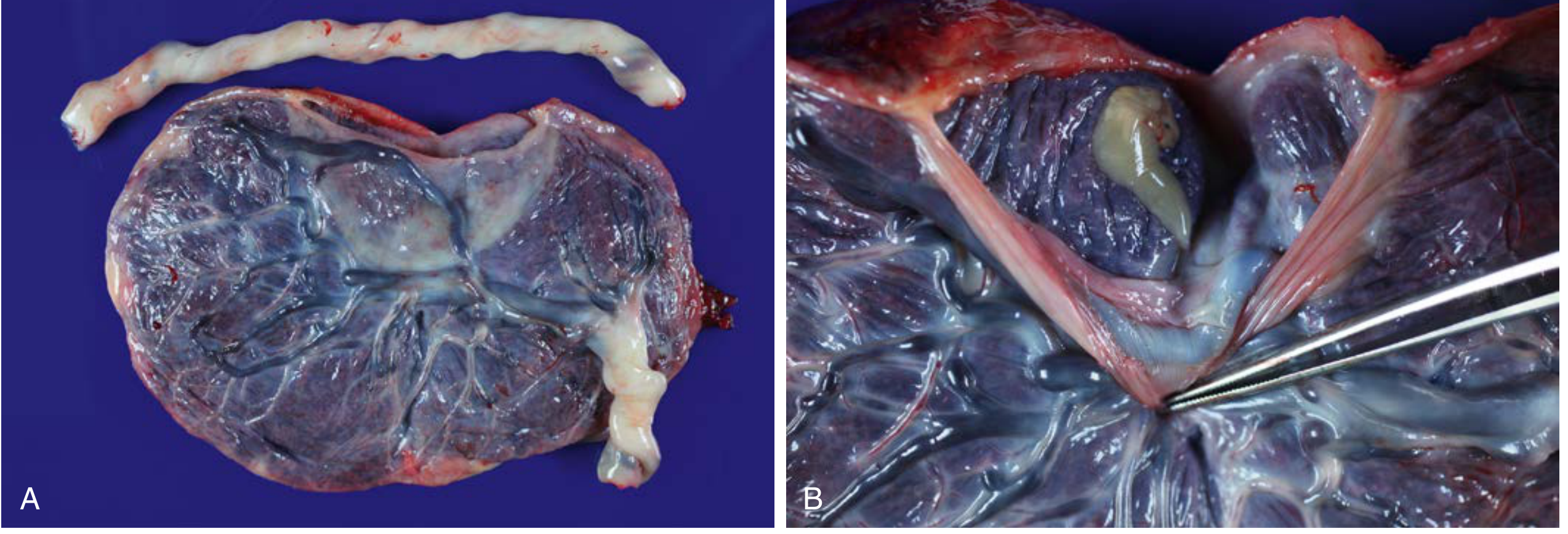
| Fetus papyraceus | A compressed, mummified fetal remnant from a twin that died between 12-20 weeks; progressively flattened by the growing co-twin |
| sIUFD | Single intrauterine fetal demise - death of one fetus in the 2nd or 3rd trimester |
2. How Common Is It?
- Vanishing twin in the first trimester: reported in ~21% of twin pregnancies
- sIUFD after 12 weeks: occurs in ~6% of all twin pregnancies overall
- Before 22 weeks: ~0.7% of dichorionic and ~0.9% of monochorionic-diamniotic twin pregnancies
3. Causes (Pathogenesis)
- Fetal causes: discordant infections, discordant structural anomalies, discordant fetal growth, abnormal fetoplacental blood flow
- Placental causes: uneven placental sharing, placental implantation anomalies, peripheral cord insertion
- Maternal causes: preeclampsia, thrombophilia, placental abruption
- Iatrogenic: after selective feticide, after laser therapy for twin-to-twin transfusion syndrome (TTTS)
4. Why Chorionicity is the Single Most Important Factor
Monochorionic (shared placenta) twins have vascular connections between them. When one twin dies:
- Blood acutely shifts from the surviving twin into the dead twin through these connections
- This causes sudden, severe hypotension and acute anemia in the survivor
- This is the primary mechanism of neurological injury - it happens at the moment of death, so obstetric intervention is often already too late to prevent it
Dichorionic (separate placentas): no vascular connections, so this acute hemorrhagic mechanism does not occur. Consequences are much milder.
5. How to Identify / Diagnosis
First Trimester (Vanishing Twin)
- Ultrasound is the primary tool - a second gestational sac or embryo is seen early but absent on follow-up scan
- A collapsed/partially resorbed sac with embryonal remnants (vertebral column, ocular pigment) may be found
- Genetic evidence of a resorbed twin may appear as restricted placental chimerism
Second/Third Trimester
- Ultrasound: absence of fetal cardiac activity in one fetus; may show echogenic (compressed/macerated) fetal parts - fetus papyraceus
- MRI of the fetal brain: superior to ultrasound for detecting neurological injury in the surviving twin - detects brain abnormalities in 13% of monochorionic survivors; ultrasound under-calls severity in ~67% of these cases
- Neurosonography (fetal brain ultrasound): first-line imaging for the survivor's brain
- Look for: multicystic encephalomalacia, white matter lesions, cortical changes
- Maternal coagulation screen: disseminated intravascular coagulation (DIC) was historically feared (once estimated 25% risk), but modern data show clinical DIC is rare after spontaneous or selectively terminated twin demise
Placental pathology (post-delivery)
- Focal membrane thickening on the chorionic plate of an apparently singleton placenta
- Plaque-like thickening on one side of the placental disk (fetal side)
6. Risks to the Surviving Twin
Neurological Injury
| Placenta type | Co-twin death also | Abnormal neonatal brain imaging | Serious neurologic injury (e.g. multicystic encephalomalacia) |
|---|---|---|---|
| Monochorionic | ~15% | 34% | 26% |
| Dichorionic | ~3% | 16% | 2% |
- Risk of neurological injury at any gestational age in monochorionic twins - there is no safe early gestational cutoff; injury has been reported after co-twin death at as early as 12 weeks
- Risk is highest when sIUFD occurs between 28-33 weeks gestation in monochorionic pregnancies
- Surviving fetuses from vanishing twin pregnancies have increased risk of small for gestational age (inversely related to gestational age at time of co-twin death)
Preterm Birth
- Increased risk of medically indicated or spontaneous preterm birth
7. Management
General Principles
The cornerstone of management is chorionicity-guided decision-making.
First Trimester Vanishing Twin
- Usually requires no specific intervention
- Continue routine antenatal surveillance
- Be aware of increased SGA risk in the surviving twin
Second/Third Trimester sIUFD
Monochorionic Twins
- Neurological injury likely already occurred at moment of death - emergent delivery rarely helps the surviving twin's brain
- Fetal brain neuroimaging (neurosonography + fetal MRI) to assess the surviving twin
- If fetal demise has already occurred: close surveillance with serial ultrasound; delivery at 37 weeks is reasonable
- If one fetus appears premorbid (about to die): the 26% risk of profound neurological injury after co-twin death must be weighed against complications of prematurity - delivery may be considered depending on gestational age
Dichorionic Twins
- Risk to surviving twin is much lower (~2-3% co-death, 2% serious neurological injury)
- Expectant management is generally appropriate
- Serial surveillance with ultrasound
- Monitor maternal coagulation profile (DIC, although rare, is possible with prolonged retention)
- Delivery timing should balance gestational age against ongoing risks
Delayed-Interval Delivery (Special scenario: one twin delivers preterm)
When one twin delivers preterm (especially before 24 weeks) but the other remains in utero:
- Protocol: cord ligation of the delivered twin near the placenta, tocolysis, broad-spectrum antibiotics, anti-D prophylaxis (if Rh-negative), possible cerclage placement, serial amniocentesis to exclude infection
- Mean latency achieved: ~36 days (range 3-123 days)
- Survival rates for the remaining twin: 50% when initial delivery before 25 weeks
- Meta-analysis of 492 cases: delayed delivery significantly improved survival (OR 5.22; 95% CI 2.95-9.25)
- Serious maternal morbidity reported in 39% of cases with this approach - careful counseling is mandatory
Maternal Monitoring
- Maternal coagulation profile (PT, aPTT, fibrinogen, D-dimer) - especially important if demise is prolonged or suspected
- Anti-D immunoglobulin in Rh-negative mothers
- Grief counseling and psychological support
8. Summary Table
| Feature | First Trimester | Monochorionic (2nd/3rd trimester) | Dichorionic (2nd/3rd trimester) |
|---|---|---|---|
| Co-twin death risk | Low | ~15% | ~3% |
| Serious neuro injury risk | Low | ~26% | ~2% |
| Key diagnosis tool | Ultrasound | Ultrasound + fetal MRI | Ultrasound |
| Management | Expectant | Close surveillance; consider timing delivery; neuroimaging | Expectant; surveillance |
| DIC risk | Negligible | Low (historically overestimated) | Low |
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice - Chapter on Multiple Gestations, pp. 852-860
Recent evidence: A 2023 systematic review (PMID 37179347) on antenatal management of dichorionic-diamniotic twins confirms that chorionicity-based surveillance remains the standard approach in current guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.