Epigenetics in obstetrics and gynecology - MS exam
Reading File
Finding Sources
Finding Sources
Searching the Web
epigenetics obstetrics gynecology MS exam review 2025
Searching PubMed
epigenetics obstetrics gynecology review
Reading File
Finding Sources
Finding Sources
Searching PubMed
epigenetics preeclampsia fetal programming
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have all the material needed. Here is the comprehensive MS exam answer:
Epigenetics in Obstetrics and Gynecology
1. Definition and Core Concept
Epigenetics is the study of heritable changes in gene function that cannot be explained by alterations in the DNA sequence itself. This classic definition has been expanded to include modifications such as histone acetylation and phosphorylation, where gene expression is impacted but the modifications are not necessarily inherited to all progeny.
The key distinction from classical genetics: the DNA sequence is unchanged, yet gene expression is altered.
Epigenetic marks are regulated by three classes of proteins:
| Class | Function | Example |
|---|---|---|
| Writers | Add epigenetic marks to DNA/histones | Histone acetyltransferases (HATs), DNA methyltransferases (DNMT1) |
| Readers | Recognize and bind epigenetic marks | MECP2, Polycomb repressive complex (CBX2), chromatin remodeling enzyme SMARCA4 |
| Erasers | Remove epigenetic marks | Histone deacetylases (HDACs), Histone demethylases (HDMs), TET1 |
2. The Four Mechanisms of Epigenetic Regulation
A. Histone Acetylation
- DNA is coiled around histone octamers (H2A, H2B, H3, H4) in units of ~140 bp called nucleosomes
- HATs (writers) add acetyl groups to histone tails → open, loosely packed chromatin → transcriptionally ACTIVE
- HDACs (erasers) remove acetyl groups → tightly packed chromatin → transcriptionally INACTIVE
- Reader proteins bind acetylated histones via a bromodomain (e.g., SMARCA4/BRG1)
- Phosphorylation of histones also opens chromatin structure and activates transcription
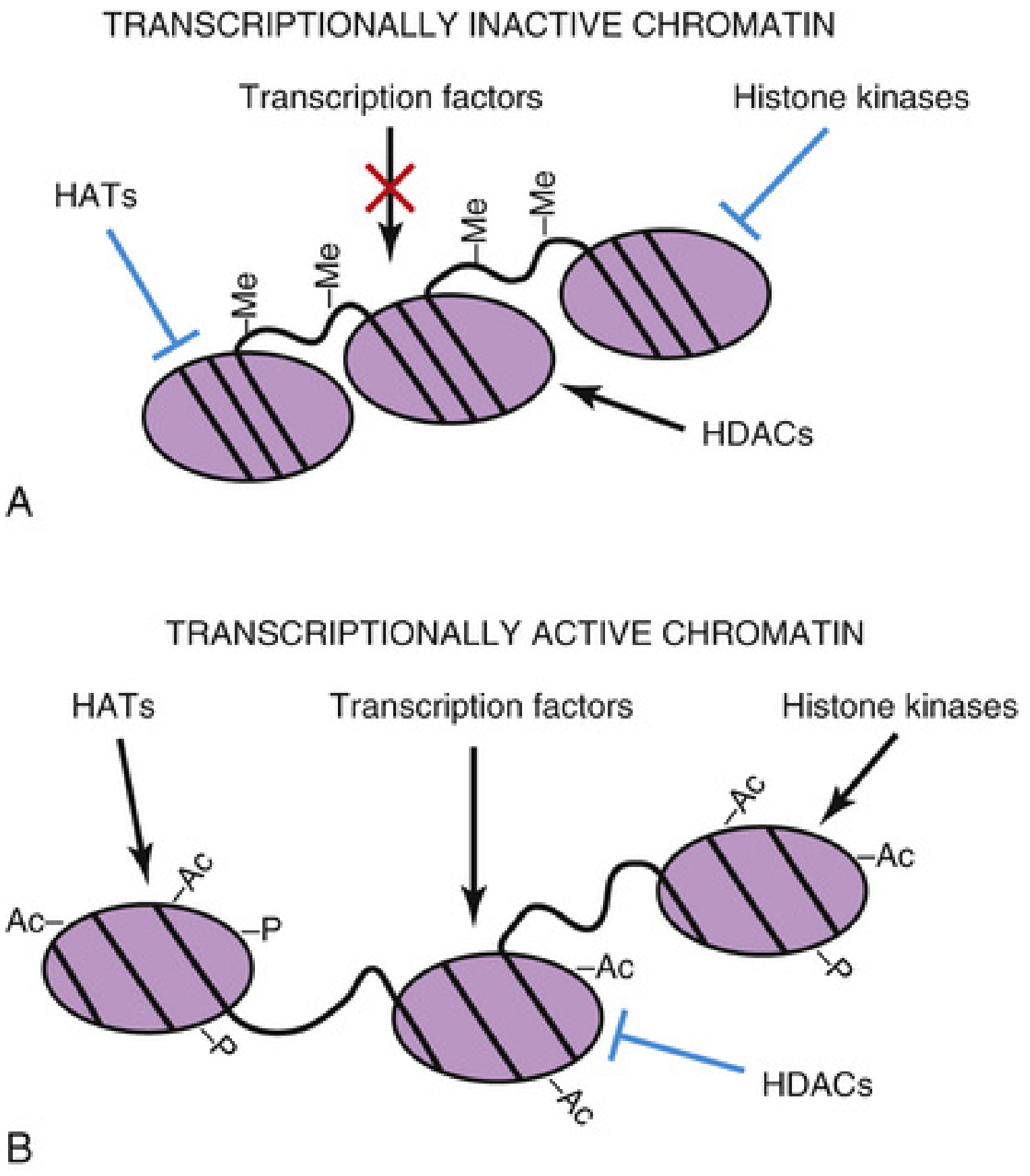
Fig. 21.10 from The Developing Human - Inactive chromatin (A): DNA tightly bound, methylated (-Me), HDACs active, HATs inhibited. Active chromatin (B): DNA loosely bound, unmethylated, histones acetylated (-Ac) and phosphorylated (-P), HATs and kinases active.
B. Histone Methylation
- Histone methyltransferases (HMTs/writers) add methyl groups to lysine residues on histone tails
- Unlike acetylation, methylation can activate OR repress transcription depending on which residue is modified:
- H3K9me3 and H3K27me3 (trimethylation of lysine 9 or 27 on Histone 3) → gene repression
- H3K4me3 (trimethylation of lysine 4 on Histone 3) → gene activation
- Removed by histone demethylases (HDMs/erasers)
C. DNA Methylation
- Cytosine residues are methylated at CpG dinucleotides after embryo implantation by DNA methyltransferases (DNMT1)
- CpG methylation → long-term, stable gene silencing/repression
- During embryonic development, pluripotency genes are repressed by methylation as cells differentiate
- The methylation state is erased in primordial germ cells to enable re-expression of pluripotency genes
- Viral genomes integrated into our DNA are silenced via methylation (repressive marks NOT reset in primordial germ cells - inherited by progeny)
- MECP2 (reader) binds methylated DNA → mutation causes Rett syndrome
- Clinical epigenetic therapies: 5-azacytidine, decitabine (DNA demethylating agents); valproic acid (HDAC inhibitor)
D. MicroRNAs (miRNAs)
- Short (~22 nucleotide), highly conserved, noncoding RNAs that act post-transcriptionally to silence RNA
- Target >50% of all genes expressed during development; each miRNA targets hundreds of genes
- Biogenesis pathway:
- RNA polymerase II/III converts DNA → pri-miRNA (nucleus)
- Drosha + DGCR8 microprocessor complex cleaves pri-miRNA → pre-miRNA (nucleus)
- Exportin-5 exports pre-miRNA to cytoplasm
- Dicer (RNase III endoribonuclease) processes hairpin → miRNA duplexes (cytoplasm)
- RISC complex converts duplexes → mature miRNA
- Mature miRNA → repression of translation OR mRNA degradation → decreased protein function
- Oncomirs: miRNAs dysregulated in cancer
- Germline mutations of DICER1 → familial tumor predisposition syndrome (pleuropulmonary blastoma, cystic nephroma, medulloepithelioma)
3. Epigenetics in Obstetrics
A. Epigenetic Regulation of Placental Development
Source: Creasy & Resnik's Maternal-Fetal Medicine
The expression of developmental genes in the placenta is regulated in a nonrandom, parent-of-origin-dependent manner via genomic imprinting - a critical epigenetic process.
Key principle: Paternal genes largely control placental development; maternal genes are more active in embryonic development.
Classic Example - IGF-II (Insulin-like Growth Factor II):
- IGF-II is an important growth factor in early development
- The maternal allele is hypermethylated (imprinted) = silenced
- IGF-II is therefore expressed only from the paternal allele
- The placenta expresses abundant paternally-inherited/maternally-imprinted IGF-II
- This is a major regulator of placental growth and function
- Insufficient IGF-II expression (e.g., from maternal isodomy) → fetal growth restriction (FGR)
- This has been explained by the "kinship theory": paternal genes promote growth, maternal genes regulate/restrain growth
"Kinship Theory" of Imprinting (Exam Point):
- Evolutionary concept: paternally expressed genes promote fetal/placental growth
- Maternally expressed genes moderate/limit growth
- Conflict between maternal and paternal genomes in controlling resource allocation to the fetus
B. Genomic Imprinting and Clinical Disorders
| Imprinting Abnormality | Clinical Result |
|---|---|
| Complete Hydatidiform Mole | All nuclear DNA is paternal (androgenetic origin) → excessive trophoblast/placental proliferation, no embryo |
| Loss of p57KIP2 (normally expressed from maternal allele in cytotrophoblast/villous stroma) | Abnormally large chorionic villi, concentric trophoblast proliferation in complete moles |
| Beckwith-Wiedemann syndrome | Loss of maternal imprinting at 11p15 → overgrowth syndrome, macroglossia, omphalocele, organomegaly, hypoglycemia |
| Silver-Russell syndrome | Aberrant imprinting → growth restriction, body asymmetry |
| Prader-Willi syndrome | Loss of paternal 15q11-q13 expression (or maternal UPD15) → hypotonia, obesity, hypogonadism |
| Angelman syndrome | Loss of maternal 15q11-q13 expression (or paternal UPD15) → intellectual disability, seizures, inappropriate laughter |
| Placental imprinting defect | Fetal growth restriction due to placental insufficiency |
p57KIP2 (CDKN1C) - Exam High-Yield:
- Tumor suppressor gene
- Expressed exclusively from the maternal allele in cytotrophoblast and villous stromal cells
- Absent in complete hydatidiform mole (all paternal DNA)
- Useful immunohistochemical marker to distinguish complete from partial mole
C. Placental DNA Methylation and Pregnancy Complications
- Differential methylation profiles exist in early human development based on parental allele inheritance
- Placental DNA methylation at specific sites is associated with insulin sensitivity in late pregnancy (important in gestational diabetes)
- The placenta can shed fetal cell-free DNA (cffDNA) into the maternal circulation; placenta-specific methylation signatures are used in non-invasive prenatal testing (NIPT) to identify fetal DNA
D. Preeclampsia and Epigenetics
- Circulating miRNAs are altered in preeclampsia and act from the time of implantation
- miRNA dysregulation affects trophoblast invasion and spiral artery remodeling
- DNA methylation changes in placental genes are associated with preeclampsia risk
- Older first-trimester epigenetic age (GrimAge2) is associated with a composite of pregnancy complications (2025 data, PMID 40638919)
E. X-Chromosome Inactivation (Lyon Hypothesis) - Epigenetic in Females
- In females with 2 X chromosomes, one X in each cell is randomly inactivated early in development (lyonization)
- The inactive X condenses to form the Barr body (sex chromatin, visible in interphase nucleus as a dark mass against the nuclear membrane)
- The process involves the X-inactivation center (Xic) and the XIST gene which coats the inactive X
- This is dosage compensation - ensures equivalent X-linked gene expression in males (XY) and females (XX)
- All daughter cells maintain the same inactive X (clonal)
- Clinically relevant in:
- Carriers of X-linked recessive disorders (variable expression due to skewed X-inactivation)
- Turner syndrome (45,X): no Barr body
- Klinefelter syndrome (47,XXY): 1 Barr body
4. Fetal Programming / DOHaD Hypothesis (Barker Hypothesis)
Developmental Origins of Health and Disease (DOHaD)
- Environmental stresses during pregnancy cause epigenetic changes that affect the fetus and translate into disease in adult life
- Epigenetic modification of the genome is widespread, occurs primarily during fetal development but extends into adulthood
- Allows the fetus to respond in utero to environmental cues (nutrition, stress, toxins)
Key Evidence:
- Dutch Hunger Winter (1944-1945): Severe maternal undernutrition → offspring developed hypertension, type 2 diabetes, obesity decades later
- Low birthweight → increased risk for hypertension, diabetes, metabolic syndrome, renal disease in adult life
- Placental insufficiency → most common cause of FGR in the Western world → programs chronic disease in offspring
- Glucocorticoid receptor (GR) promoter methylation in response to early adverse environments → alters HPA axis programming
Mechanism: Intrauterine stress → epigenetic marks (especially DNA methylation of metabolic gene promoters) → permanently altered gene expression → disease susceptibility
5. Epigenetics in Gynecology
A. Gynecologic Cancers
DNA methylation of tumor suppressor gene promoters is a common mechanism of oncogenesis in gynecologic cancers:
| Cancer | Epigenetic Mechanism |
|---|---|
| Endometrial cancer | Hypermethylation of MLH1 (mismatch repair gene) → MSI pathway; HDAC dysregulation |
| Cervical cancer | HPV-induced epigenetic silencing of host tumor suppressors; miRNA dysregulation |
| Ovarian cancer | BRCA1 promoter methylation; EZH2 (histone methyltransferase) overexpression; miRNA oncomirs |
| Choriocarcinoma/GTD | Aberrant imprinting; abnormal methylation patterns from androgenetic (complete mole) or digynic (partial mole) origins |
Chromatin remodeling disorder examples:
- Rett syndrome (MECP2 mutation)
- Rubinstein-Taybi syndrome (EP300/CBP - histone acetyltransferase mutations)
- α-thalassemia/X-linked mental retardation (ATRX mutations)
B. PCOS and Epigenetics
- Adipose tissue dysfunction in PCOS involves epigenetic dysregulation
- Androgen excess may program epigenetic changes affecting metabolic function in future generations
- miRNA profiles are altered in granulosa cells of PCOS patients
C. Endometriosis
- Aberrant DNA methylation of steroidogenic genes (e.g., aromatase/CYP19A1 promoter hypomethylation in ectopic endometrium → excess local estrogen production)
- Progesterone resistance in endometriosis linked to epigenetic silencing of progesterone receptor isoforms
- HDAC inhibitors are being explored therapeutically
6. Epigenetic Clocks and Pregnancy Aging
- Epigenetic clocks (e.g., GrimAge2) measure biological age via DNA methylation patterns
- Pregnancy accelerates within-person epigenetic aging by up to 5.3 years
- Older first-trimester GrimAge2 (biological age older than chronological age) is associated with adverse pregnancy outcomes
- Non-pregnant controls show less epigenetic aging over the same time interval
- These findings suggest gestation influences biological aging and epigenetic age may be a marker of pregnancy health
7. Summary Table for Quick Revision
| Topic | Exam Takeaway |
|---|---|
| Epigenetics definition | Heritable gene expression changes WITHOUT DNA sequence change |
| 4 mechanisms | Histone acetylation, histone methylation, DNA methylation, miRNA |
| HATs vs HDACs | HATs → open chromatin → active; HDACs → compact chromatin → silent |
| DNA methylation | CpG methylation → gene SILENCING; DNMT1 writes; TET1 erases |
| Genomic imprinting | Parent-of-origin gene expression; IGF-II = paternal only |
| Complete mole | All paternal DNA → excessive placenta, no embryo; no p57KIP2 |
| Kinship theory | Paternal genes promote growth; maternal genes restrain growth |
| X-inactivation | Lyon hypothesis; random; Barr body = inactive X; XIST gene |
| Barker/DOHaD | Intrauterine environment → epigenetic programming → adult disease |
| Endometriosis | Aromatase promoter hypomethylation → excess local estrogen |
| Therapeutic targets | 5-azacytidine (demethylating); valproic acid/HDAC inhibitors |
| miRNA | 22-nt noncoding RNA; RISC complex; Dicer enzyme; oncomirs |
| Beckwith-Wiedemann | Loss of maternal imprinting at 11p15 |
| Silver-Russell | Aberrant imprinting → FGR, asymmetry |
| Pregnancy epigenetic aging | Pregnancy ages biological clock up to 5.3 years (2025 data) |
Sources:
- The Developing Human: Clinically Oriented Embryology, Chapter 21 (Epigenetics, pp. 1335-1344)
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice - Epigenetic Regulation of Placental Development, p. 81
- Thompson & Thompson Genetics and Genomics in Medicine, 9th ed. - X Chromosome Inactivation, Imprinting
- Robbins & Cotran Pathologic Basis of Disease - Cytogenetic Disorders involving Sex Chromosomes
- Panelli et al., "Longitudinal Epigenetic Aging in Pregnancy," Obstet Gynecol 2025 (PMID 40638919)
- Giannubilo et al., "Circulating miRNAs and Preeclampsia: From Implantation to Epigenetics," Int J Mol Sci 2024 (PMID 38338700)
Epigenetics and ART short note
Finding Sources
Finding Sources
Searching PubMed
epigenetics assisted reproductive technology imprinting disorders
Searching the Web
epigenetics ART assisted reproductive technology imprinting IVF ICSI risks 2024 2025
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I now have all the material needed for a comprehensive, exam-focused short note. Here it is:
Epigenetics and Assisted Reproductive Technology (ART)
Why ART and Epigenetics Are Inextricably Linked
ART procedures (IVF, ICSI, ovarian stimulation, embryo culture, cryopreservation) are performed during the most epigenetically vulnerable window in human development - the periconceptional and preimplantation period. This is precisely when two critical waves of epigenetic reprogramming occur:
- Erasure of parental imprints in primordial germ cells
- Re-establishment and maintenance of genomic imprints during oocyte maturation and after fertilization
Any external interference during these phases can disrupt epigenetic programming permanently.
The Two Critical Vulnerable Periods
| Period | Epigenetic Event | ART Interference |
|---|---|---|
| Oocyte maturation | Establishment of maternal imprints; completion of epigenetic reprogramming | Ovarian hyperstimulation recruits immature oocytes not yet fully reprogrammed |
| Preimplantation embryo (fertilization to blastocyst) | Genome-wide demethylation of paternal genome, then de novo methylation; maintenance of imprint marks | IVF culture conditions, ICSI, embryo freezing/thawing all occur here |
ART Procedures and Their Specific Epigenetic Risks
1. Ovarian Hyperstimulation (Superovulation)
- Gonadotropins recruit a cohort of follicles, including those that are immature and not yet fully epigenetically reprogrammed
- Oocytes may have incomplete maternal imprint establishment at imprinting control regions (ICRs)
- This is the most implicated single factor in ART-related imprinting errors
- May also affect DNA methylation at non-imprinted loci
2. In Vitro Fertilization (IVF)
- Gametes and embryos are exposed to artificial culture media with suboptimal nutrient composition compared to the fallopian tube environment
- Culture media composition (amino acids, glucose, oxygen tension, growth factors) can alter histone modifications and DNA methylation
- Increased risk of imprinting disorders: BWS risk rises from 1/13,000 (general population) to approximately 1/2,500 after IVF (several-fold increase)
- Associated with low birthweight, preterm birth, and abnormal placentation
3. ICSI (Intracytoplasmic Sperm Injection)
- Bypasses natural sperm selection processes
- Men needing ICSI often have oligospermia/azoospermia with underlying genetic/epigenetic sperm abnormalities (genome-wide alterations in histone modifications and DNA methylation)
- Sperm from infertile men show abnormal genome packaging and DNA methylation compared to fertile men
- ICSI has been more consistently linked to multilocus imprinting disturbances (MLID) than conventional IVF
- Placentas from ICSI children show global H3K4me3 (histone methylation) differences compared to naturally conceived children
- Concern about overuse of ICSI beyond strict male-factor infertility
4. Embryo Culture Conditions
- Culture medium composition directly influences the epigenome of the pre-implantation embryo
- High glucose, suboptimal amino acids, non-physiological O₂ tension → aberrant de novo methylation
- Different culture media brands have been associated with different birthweight outcomes in animal and human studies
5. Cryopreservation (Embryo/Oocyte Freezing)
- The freeze-thaw process may induce epigenetic changes
- Paradoxically, frozen embryo transfer (FET) is associated with higher birthweights than fresh transfer (possibly due to absence of supraphysiologic hormone levels from stimulation)
- Risk of epigenetic disturbance from cryoprotectants and osmotic stress during freezing is under investigation
ART-Associated Imprinting Disorders
Meta-analysis data: frequency of imprinting disorders in ART-born babies is 3.44 to 3.67-fold higher than naturally conceived children.
| Imprinting Disorder | Chromosome | Mechanism | ART Risk |
|---|---|---|---|
| Beckwith-Wiedemann syndrome (BWS) | 11p15 | Loss of methylation at IC2 (maternal); hypermethylation IC1 → excess IGF2 → overgrowth | 3-9x increased; risk ~1/2,500 vs 1/13,000 in general population |
| Russell-Silver syndrome (RSS/SRS) | 11p15, 7 | Hypomethylation of IC1 → reduced IGF2 → undergrowth; mirror image of BWS | Increased with ART |
| Angelman syndrome (AS) | 15q11-q13 | Loss of maternal UBE3A expression; loss of methylation at maternal allele | Increased with ART (6 cases with AS after ICSI reported with imprinting defect) |
| Prader-Willi syndrome (PWS) | 15q11-q13 | Loss of paternal expression | Increased with ART |
Key molecular detail for BWS (Exam High-Yield):
- The 11p15 region has two imprinting domains:
- IC1 (telomeric): Contains IGF2 (paternal, growth-promoting) and H19 (maternal). IC1 normally methylated on paternal allele → IGF2 expressed, H19 silenced.
- IC2 (centromeric): Contains CDKN1C (p57KIP2), KCNQ1, KCNQ1OT1. IC2 normally methylated on maternal allele → CDKN1C expressed (growth suppressor), KCNQ1OT1 silenced.
- In ART-associated BWS: predominantly IC2 hypomethylation (loss of maternal methylation) → KCNQ1OT1 expressed, CDKN1C silenced → overgrowth
- BWS and RSS are clinical and molecular mirror images of each other at 11p15
Multilocus Imprinting Disorder (MLID)
A particularly important ART-specific epigenetic complication:
- Normal imprinting disorders affect one locus (e.g., BWS affects 11p15)
- In ART conceptions, DNA methylation alterations occur not only at specific loci but at multiple imprinted loci simultaneously
- This is called MLID (Multilocus Imprinting Disorder)
- Children with MLID may present with features of a single known imprinting disorder, or overlapping features of multiple imprinting disorders
- MLID can result from:
- ART processes themselves (hormone therapy, culture medium)
- Primary subfertility of the couple (poor oocyte/sperm quality)
- Pathogenic variants in maternal effect genes (NLRP5, PADI6, ZFP57) that impact imprinted loci in trans
Epigenetic Sperm Abnormalities and Paternal ART Risk
- Sperm from infertile men (required for ICSI) exhibit genome-wide alterations in:
- Histone modifications (genome packaging)
- DNA methylation patterns
- Compared to fertile men's sperm on chip microarray analysis
- Epigenetic changes in sperm may be acquired transgenerationally or from conditions such as obesity
- Episona test: commercial test for sperm epigenetic assessment (though limited clinical utility currently)
- Weight loss in obese men may reverse/ameliorate epigenetic sperm changes through chromatin remodeling
- The underlying male factor infertility (not just ICSI procedure itself) contributes to epigenetic risk
Transgenerational Epigenetic Inheritance
- Concern that epigenetic errors introduced by ART may not just affect the child conceived, but potentially future generations (grandchildren)
- ART bypasses natural epigenetic checkpoints of reproduction
- Sperm or oocyte epigenetic abnormalities can be transmitted to offspring and may persist
Clinical Outcomes in ART Pregnancies (Epigenetic Basis)
| Outcome | Epigenetic Contribution |
|---|---|
| Low birthweight (fresh ET) | Placental imprinting disruption; IGF2 dysregulation |
| Large-for-gestational age (frozen ET) | Avoidance of supraphysiologic estrogens; different imprinting patterns |
| Increased BWS incidence | IC2 hypomethylation (predominantly maternal) |
| Abnormal placentation (previa, abruption) | Trophoblast epigenetic dysregulation |
| Increased congenital malformations | Broad epigenetic reprogramming errors |
Summary: Key Exam Points
| Point | Detail |
|---|---|
| Most vulnerable window | Periconceptional period - oocyte maturation + preimplantation |
| Biggest single risk factor | Ovarian hyperstimulation (immature oocytes) |
| Most studied disorder | Beckwith-Wiedemann syndrome (BWS) - IC2 loss of methylation |
| Risk of BWS after IVF | ~1/2,500 vs 1/13,000 in natural conception |
| Overall imprinting disorder risk with ART | 3.44 to 3.67-fold higher than natural conception |
| Mechanism | Disruption of imprint establishment, maintenance, or reprogramming |
| MLID | Multiple imprinted loci affected simultaneously - ART-specific pattern |
| ICSI-specific | More linked to MLID; sperm from infertile men have intrinsic epigenetic defects |
| Maternal effect genes | NLRP5, PADI6, ZFP57 - variants cause ART-independent MLID |
| ART accounts for | >1% of all births in many countries - public health significance |
Sources:
- Thompson & Thompson Genetics and Genomics in Medicine, 9th ed. - "The Environment Interacts with the Epigenome" + "BWS and ART" (pp. 157-161)
- Berek & Novak's Gynecology - "Epigenetic Sperm DNA Assessment" + "Risks of ICSI"
- Emery's Elements of Medical Genetics and Genomics - In Vitro Fertilization
- Kagami et al., "Association between imprinting disorders and ART," Epigenomics 2025 (PMID 40033833)
- Zhang et al., "ART and imprinting errors: analyzing underlying mechanisms," Hum Fertil 2023 (PMID 37929309)
- Sciorio & El Hajj, "Epigenetic Risks of Medically Assisted Reproduction," J Clin Med 2022 (PMID 35456243)
This is a shared conversation. Sign in to Orris to start your own chat.