Lower back pain radiating to bilateral lower limbs … examination and theory
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
low back pain bilateral radiculopathy diagnosis management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Low Back Pain Radiating to Bilateral Lower Limbs
Why Bilateral?
Unilateral leg radiation (sciatica) is far more common. When symptoms radiate bilaterally, the clinician must think of conditions that involve the central canal or the cauda equina as a whole, rather than a single nerve root. The key causes are:
- Lumbar spinal stenosis (neurogenic claudication) - most common bilateral cause
- Large central/paracentral disc herniation compressing multiple roots
- Cauda equina syndrome - surgical emergency
- Spondylolisthesis with canal compromise
- Epidural abscess, haematoma, or tumour (red flags)
- Facet joint syndrome (bilateral referred pain, usually not below the knee)
PART 1 - PATHOPHYSIOLOGY AND THEORY
Anatomy Recap
The spinal cord ends at L1-L2 as the conus medullaris. Below this, the cauda equina (L2-S5 nerve roots) descends within the lumbar thecal sac. Any central pathology at L1 and below irritates or compresses multiple nerve roots simultaneously, producing bilateral symptoms.
The lumbar canal is bounded anteriorly by the disc and vertebral body, posteriorly by the ligamentum flavum and laminae, and laterally by the pedicles. The critical spaces are:
- Central canal - compression here causes bilateral neurogenic claudication or cauda equina syndrome
- Lateral recess - compression causes unilateral radiculopathy
- Neural foramen - foraminal stenosis causes unilateral radiculopathy
Cause 1 - Lumbar Spinal Stenosis (Most Common)
Degenerative spinal stenosis is the most frequent indication for spinal surgery in patients over 65. The pathological cascade:
- Intervertebral disc loses height and degenerates
- Ligamentum flavum buckles and hypertrophies posteriorly
- Disc herniation or bulge narrows the canal anteriorly
- Facet joint hypertrophy and osteophytes compress the lateral recess
- Spondylolisthesis compounds the narrowing
The most commonly affected level is L4-L5, also the most frequent site of degenerative spondylolisthesis.
Neurogenic claudication (pseudoclaudication) is the hallmark. Symptoms are usually bilateral but often asymmetric. The mechanism: neural compression worsens in extension (lordotic posture narrows the canal further) and improves with flexion (which opens the canal). - Firestein & Kelley's Textbook of Rheumatology
"Bilateral symptoms with >90% specificity for lumbar spinal stenosis" are produced by neurogenic claudication - Firestein & Kelley's
Congenital stenosis: short pedicles from birth; patients become symptomatic in the 3rd-5th decade when even mild superimposed degenerative changes tip them into symptomatic stenosis.
Cause 2 - Lumbar Disc Herniation (Central/Paracentral)
Disc herniation accounts for the majority of sciatica, typically at L4-L5 or L5-S1. A large central herniation can compress multiple roots bilaterally. Acute herniation may cause:
- Severe LBP with radiation to the dorsomedial foot (L5 involvement) or lateral foot/small toe (S1 involvement)
- If massive: cauda equina syndrome
Mechanism of pain: the herniated nucleus pulposus directly compresses and chemically irritates nerve roots (inflammatory cytokines from the nucleus pulposus sensitise root nociceptors). - Bradley and Daroff's Neurology in Clinical Practice
Cause 3 - Cauda Equina Syndrome (Surgical Emergency)
Caused by sudden massive disc herniation, haematoma, abscess, or tumour. Involves compression of the sacral nerve roots (S2-S4) controlling bladder, bowel, and sexual function.
Classic features:
- Bilateral leg pain and weakness
- Saddle anaesthesia (perineum, inner thighs, genitals)
- Bladder dysfunction (retention or incontinence)
- Bowel incontinence
- Reduced anal and bulbocavernosus reflexes
This is a neurosurgical emergency. Delayed decompression (>48 hours) is associated with permanent sphincter dysfunction.
Cause 4 - Discogenic Pain
Disc degeneration accounts for 26-42% of axial LBP. Discogenic pain is more likely to be bilateral than facet or SI joint pain, and frequently radiates into the upper and sometimes lower leg in a non-dermatomal distribution. Pain worsens with sitting or forward bending. - Harrison's Principles of Internal Medicine 22E
Cause 5 - Facet Joint Syndrome
Found in up to 35% of patients with LBP. Pain may radiate bilaterally into the back or front of the thigh but only up to the knee - it does not typically radiate below the knee. Back extension and lateral rotation toward the painful side worsen pain. Straight leg raise (SLR) is negative. - Bradley and Daroff's Neurology in Clinical Practice
Cause 6 - Conus Medullaris Syndrome
Spinal stenosis between T12 and L2 produces a mixed UMN + LMN picture (unlike cauda equina which is pure LMN). Bowel and bladder dysfunction is common. Both require urgent surgical consultation. - Firestein & Kelley's Textbook of Rheumatology
PART 2 - CLINICAL EXAMINATION
Step 1 - Inspection
Standing:
- Observe spinal alignment: loss of lumbar lordosis suggests muscle spasm; exaggerated lordosis suggests spondylolisthesis
- Sciatic scoliosis (antalgic lean): with herniation lateral to the root, the patient leans away from the lesion; medial to the root, they lean toward it
- Pelvic tilt / Trendelenburg sign - suggests hip or gluteal muscle involvement
- Sagging gluteal fold - suggests S1 root involvement
- Observe for flexed posture of the affected leg (reduces sciatic nerve tension)
Gait:
- Limp, shortened step, knee slightly flexed with weight bearing on the ball of the foot
- Foot drop / steppage gait - L4-L5 lesion (peroneal division of sciatic nerve, tibialis anterior)
- Waddle - bilateral hip girdle weakness
- Pain going up/down stairs is characteristic of sciatica
"Observation of gait can suggest nonspinal pathology (e.g., propulsive gait = Parkinson's; spastic gait = central lesion; steppage gait = peroneal neuropathy or large herniated disc)" - Harrison's Principles of Internal Medicine 22E
Step 2 - Range of Motion
| Movement | Significance |
|---|---|
| Decreased extension | Suggests spinal stenosis or spondylolisthesis |
| Decreased forward flexion | Suggests discogenic pain |
| Lateral bending to opposite side causing pain | Suggests ligamentous/muscular strain |
| Rising from seated position painful | Suggests SI joint involvement |
| Spine forward bend: normally reverses lumbar lordosis; failure to do so | Suggests disc or facet pathology |
In the sitting position, lumbar flexion can usually be performed more freely even in sciatica patients, because flexing the knees relaxes hamstrings and reduces stretch on the sciatic nerve. - Adams and Victor's Principles of Neurology, 12th Ed
Step 3 - Palpation
- Paraspinal tenderness and muscle spasm over erector spinae - disc herniation, facet joint disease
- Facet joint tenderness (2 cm lateral to the midline at each level)
- Midline tenderness - suggests ligamentous injury, vertebral fracture, infection
- SI joint tenderness (over the posterior SI joint)
- Points of Valleix: pressure along the course of the sciatic nerve - sciatic notch, retrotrochaneric gutter, posterior thigh, head of fibula - reproduces radicular pain in root compression
Step 4 - Special Tests for Nerve Root Tension
Straight Leg Raise (SLR) / Lasègue Sign
- With the patient supine, the examiner raises the straight leg by flexing the hip
- Positive: reproduces radicular (not just hamstring tightness) pain radiating below the knee at 30-70° of elevation
- Sensitive (but low specificity) for L5-S1 nerve root compression (the most commonly affected levels)
- Dorsiflexion of the ankle while holding the leg up amplifies pain (Bragard sign)
- Dorsiflexion of the great toe instead amplifies pain (Sicard sign)
- With the patient standing: forward trunk bending causes knee flexion on the affected side (Neri sign)
- Sciatica provoked by coughing, sneezing, Valsalva, or bilateral jugular vein compression = Naffziger sign (increased intraspinal pressure)
Crossed SLR (Fajersztajn Sign)
- Raising the unaffected leg reproduces radicular pain on the affected side
- Lower sensitivity than ipsilateral SLR but higher specificity (>85%) for disc herniation
- Particularly important in bilateral presentations: a positive contralateral SLR implies a large central herniation compressing roots on both sides
Femoral Stretch Test (Reverse SLR)
- Patient prone; knee passively flexed to buttock while hip is gently extended
- Reproduces anterior thigh radicular pain
- Tests L2, L3, L4 nerve roots (upper lumbar herniations) - Harrison's 22E
"The most important physical examination findings for lumbar disc herniation in patients with sciatica are ipsilateral straight leg raising causing pain, contralateral straight leg raising causing pain, and ankle or knee reflex loss" - Goldman-Cecil Medicine
Patrick's Test (FABER)
- Flexion, Abduction, External Rotation of the hip - reproduces SI joint pain
- An array of at least three positive SI provocation tests (Patrick, Gaenslen, compression, distraction) is associated with accurate identification of SI joint as the pain generator - Harrison's 22E
Romberg Test
- Abnormal in some patients with spinal stenosis (dorsal column proprioceptive compromise)
- Positive Romberg has strong predictive value for lumbosacral stenosis
Treadmill Test
- Decrease in ambulatory capacity and increase in pain with progressively greater grades of inclination
- Strong predictive value for lumbosacral stenosis - Harrison's 22E
Step 5 - Neurological Examination
This is the most important part in bilateral leg radiation. Assess systematically:
Dermatomal Sensory Testing (Pinprick and Light Touch)
| Root | Dermatome |
|---|---|
| L1 | Inguinal ligament, upper anterior thigh |
| L2 | Anterior mid-thigh |
| L3 | Medial knee and lower medial thigh |
| L4 | Medial foot, medial malleolus |
| L5 | Dorsum of foot, 1st web space, dorsomedial toes |
| S1 | Lateral foot, small toe, lateral malleolus, posterior calf |
| S2-S4 | Perianal, perineal, saddle region |
Always test S2-S4 (saddle sensation) in any bilateral presentation to screen for cauda equina syndrome.
Motor Testing
| Root | Key Muscle | Test |
|---|---|---|
| L2-L3 | Iliopsoas | Hip flexion against resistance |
| L3-L4 | Quadriceps | Knee extension; squat and rise |
| L4 | Tibialis anterior | Heel walking; foot dorsiflexion |
| L5 | Extensor hallucis longus | Great toe extension |
| L5-S1 | Peroneus longus/brevis | Foot eversion |
| S1 | Gastrocnemius/soleus | Toe walking; plantar flexion |
| S2-S4 | Sphincters | Enquire; test anal tone if indicated |
Acute disc herniation causing L5 involvement may show mild weakness of tibialis anterior; S1 involvement may show weakness of peroneus longus and brevis. - Bradley and Daroff's Neurology
Reflex Testing
| Root | Reflex |
|---|---|
| L3-L4 | Knee jerk (patellar) |
| S1 | Ankle jerk (Achilles) |
| S2-S4 | Bulbocavernosus, anal wink |
In lumbar spinal stenosis: absent ankle jerks in 40%, absent knee jerks in 10% of patients - Rheumatology (Elsevier, 2022)
In spinal stenosis, deep tendon reflexes and vibration sense may be reduced; mild diffuse lower extremity weakness is common. The SLR is usually negative in stenosis (unlike disc herniation). - Firestein & Kelley's Textbook of Rheumatology
Step 6 - Red Flag Screening (Mandatory in All LBP Patients)
Indications for urgent imaging (MRI):
- Objective signs of radiculopathy or cauda equina lesion (weakness, sensory loss, reflex loss in radicular distribution, sphincter abnormalities)
- Progressively worsening pain
- Pain aggravated by Valsalva
- Pain worse in recumbent position (worse at night - tumour)
- Back pain after trauma
- Fever + spinal tenderness (infection)
- Back pain in a patient with known cancer
- Bilateral leg radiation itself - Bradley and Daroff's Neurology in Clinical Practice
Step 7 - Differentiating Neurogenic vs Vascular Claudication
This distinction is critical because both present with bilateral leg symptoms worsened by walking.
| Feature | Neurogenic Claudication (Spinal Stenosis) | Vascular Claudication |
|---|---|---|
| Pain location | Buttocks, thighs, calves (often bilateral) | Calves primarily |
| Provoked by | Walking AND standing erect | Walking only |
| Relieved by | Flexing the spine (leaning forward, sitting, bicycle) | Rest (standing still) |
| Pedal pulses | Preserved | Reduced or absent |
| SLR | Usually negative | Negative |
| Ankle-brachial index | Normal | Abnormal (<0.9) |
| Romberg | May be abnormal | Normal |
| Relief position | Stooped or sitting | Any rest position |
"Factors that favor neurogenic claudication: preservation of pedal pulses, provocation by standing erect just as readily as by walking, relief with spinal flexion, maximal discomfort in thighs rather than calves, and a normal ankle-brachial index" - Firestein & Kelley's Textbook of Rheumatology
PART 3 - INVESTIGATIONS
Imaging
- MRI lumbar spine - modality of choice for disc herniation, stenosis, cauda equina, tumour, infection
- Canal diameter <10 mm = absolute stenosis; 10-13 mm = relative stenosis
- Sagittal T2 shows thecal sac compression; axial T2 shows central vs lateral stenosis
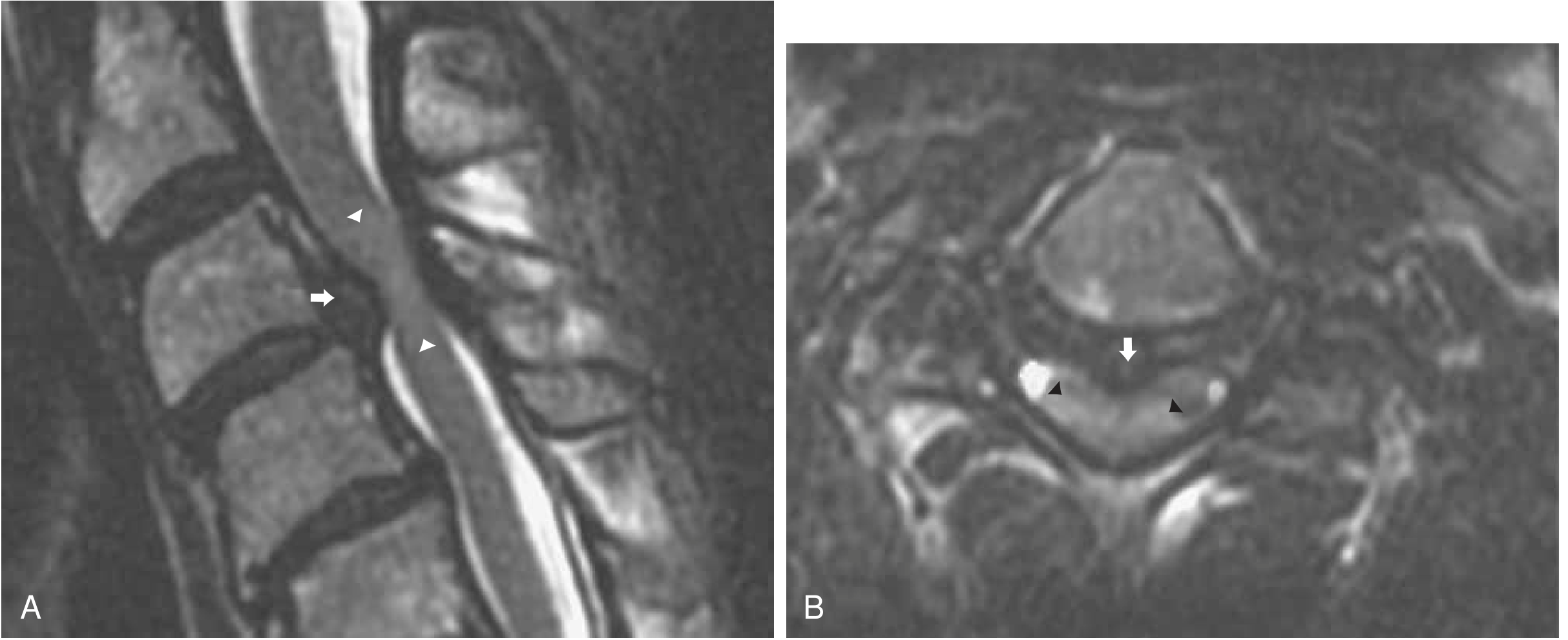
Fig: Disk herniation on MRI - sagittal T2 (left) shows disc herniation with cord compression; axial T2 (right) shows central herniation component - Bradley and Daroff's Neurology in Clinical Practice
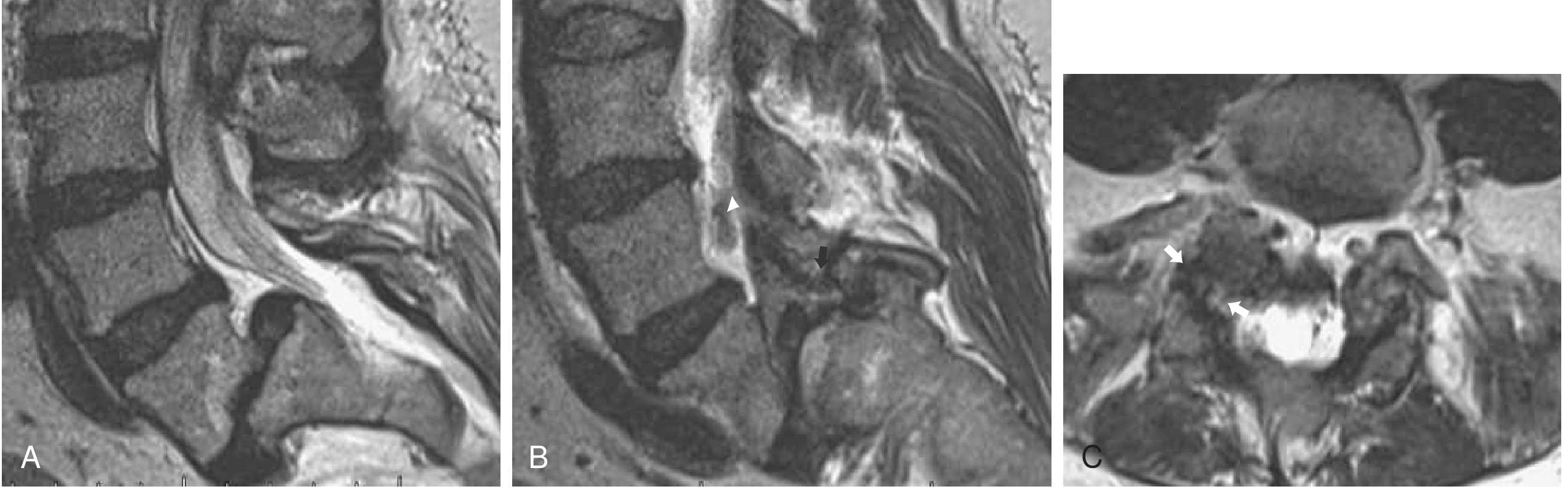
Fig: Lumbar spondylolisthesis - sagittal MRI showing multilevel degenerative disease; axial image shows bilateral foraminal stenosis - Bradley and Daroff's Neurology in Clinical Practice
- CT scan - better for bony anatomy, spondylolysis, osteophytes
- Plain X-rays - limited; useful for alignment, fractures, spondylolisthesis grading
- SPECT - more specific for facet joint arthropathy than MRI or CT
Electrodiagnostics
- EMG/NCV - may detect chronic radiculopathy (denervation, reduced SNAP, prolonged F-waves), but can be negative in acute presentations
- Useful to distinguish radiculopathy from peripheral neuropathy (which can also cause bilateral lower limb symptoms)
Lab Tests (when red flags present)
- ESR, CRP, FBC - infection, malignancy, inflammatory arthritis
- PSA - prostate cancer metastasis
- Serum calcium, alkaline phosphatase - metabolic bone disease
- Bence Jones protein / protein electrophoresis - myeloma
PART 4 - MANAGEMENT OVERVIEW
Conservative (First-line for most)
- NSAIDs - first-line pharmacotherapy for both disc herniation and stenosis
- Muscle relaxants - for acute muscle spasm
- Physical therapy - core strengthening, stretching, aerobic conditioning (especially flexion-based exercises for stenosis, e.g., cycling)
- Heat, massage, cognitive-behavioral therapy - evidence-based for chronic LBP
- Lumbar corsets (slight flexion) - limited hours/day to avoid paraspinal atrophy
- Acetaminophen - no longer recommended as first-line (insufficient evidence for LBP)
- Gabapentinoids - insufficient evidence for radicular or axial back pain
- Opioids - no long-term benefit; may be considered short-term for severe acute pain only; avoid combining with benzodiazepines
"Approximately 60-80% of the US population will experience back pain during life; most acute cases resolve within 6 weeks" - Bradley and Daroff's Neurology
Interventional
- Lumbar epidural steroid injections (LESI) - may provide short-term relief in disc herniation with radiculopathy; for spinal stenosis, a well-designed RCT found no significant advantage of glucocorticoids over lidocaine alone
- Medial branch blocks / facet joint injections - diagnostic and therapeutic for facet syndrome
- SI joint corticosteroid injection - for sacroiliac syndrome
Surgical Indications
| Condition | Indication |
|---|---|
| Cauda equina syndrome | Emergency decompression |
| Progressive neurological deficit | Urgent surgery |
| Disc herniation | Failed >3 months conservative + MRI-confirmed herniation; severe focal deficit |
| Spinal stenosis | Persistent disabling pseudoclaudication not responding to conservative care (elective) |
| Spondylolisthesis | Serious/progressive neurologic deficit |
"In patients without fixed neurologic deficits, delayed surgery produces similar benefits to surgery selected as initial treatment [for stenosis]" - Firestein & Kelley's Textbook of Rheumatology
Natural history of lumbar stenosis: symptoms remain unchanged in 70%, improve in 15%, worsen in 15% over ~49 months without intervention.
Summary Table - Differentiating Main Causes of Bilateral LBP with Leg Radiation
| Feature | Spinal Stenosis | Disc Herniation (Central) | Cauda Equina | Facet Syndrome |
|---|---|---|---|---|
| Bilateral leg radiation | Yes (hallmark) | Large central only | Yes | Rarely below knee |
| SLR | Usually negative | Positive | May be positive | Negative |
| Aggravated by | Extension, walking | Flexion, Valsalva | Any | Extension, rotation |
| Relieved by | Flexion, sitting | Variable | Surgical decompression | NSAIDs, injection |
| Sphincter dysfunction | Rare (late) | Rare | Yes (hallmark) | No |
| Saddle anaesthesia | No | No | Yes | No |
| MRI finding | Canal narrowing | Disc herniation | Large central herniation | Facet arthropathy |
| Urgency | Elective | Urgent if progressive | Emergency | Elective |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, pp. 796-800, 1099-1101
- Harrison's Principles of Internal Medicine 22E (2025), pp. 1945-1948
- Adams and Victor's Principles of Neurology, 12th Ed, pp. 217-219
- Firestein & Kelley's Textbook of Rheumatology, pp. 918-928
- Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.