Bowel obstruction detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bowel obstruction"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have extensive material from multiple authoritative textbooks. Let me compile a comprehensive answer.
Bowel Obstruction — Comprehensive Overview
Definition
Intestinal obstruction is the inability of the intestinal tract to permit regular passage of food and bowel contents, resulting from either mechanical obstruction or adynamic ileus (paralytic ileus). — Tintinalli's Emergency Medicine
Classification
By Mechanism
| Type | Description |
|---|---|
| Mechanical | Physical barrier to intestinal flow; requires intervention |
| Functional (Adynamic/Paralytic Ileus) | Loss of coordinated peristalsis without a physical blockage |
| Pseudo-obstruction (Ogilvie's syndrome) | Signs/symptoms and radiographic appearance of obstruction without mechanical lesion |
By Location of Obstructing Lesion (relative to bowel wall)
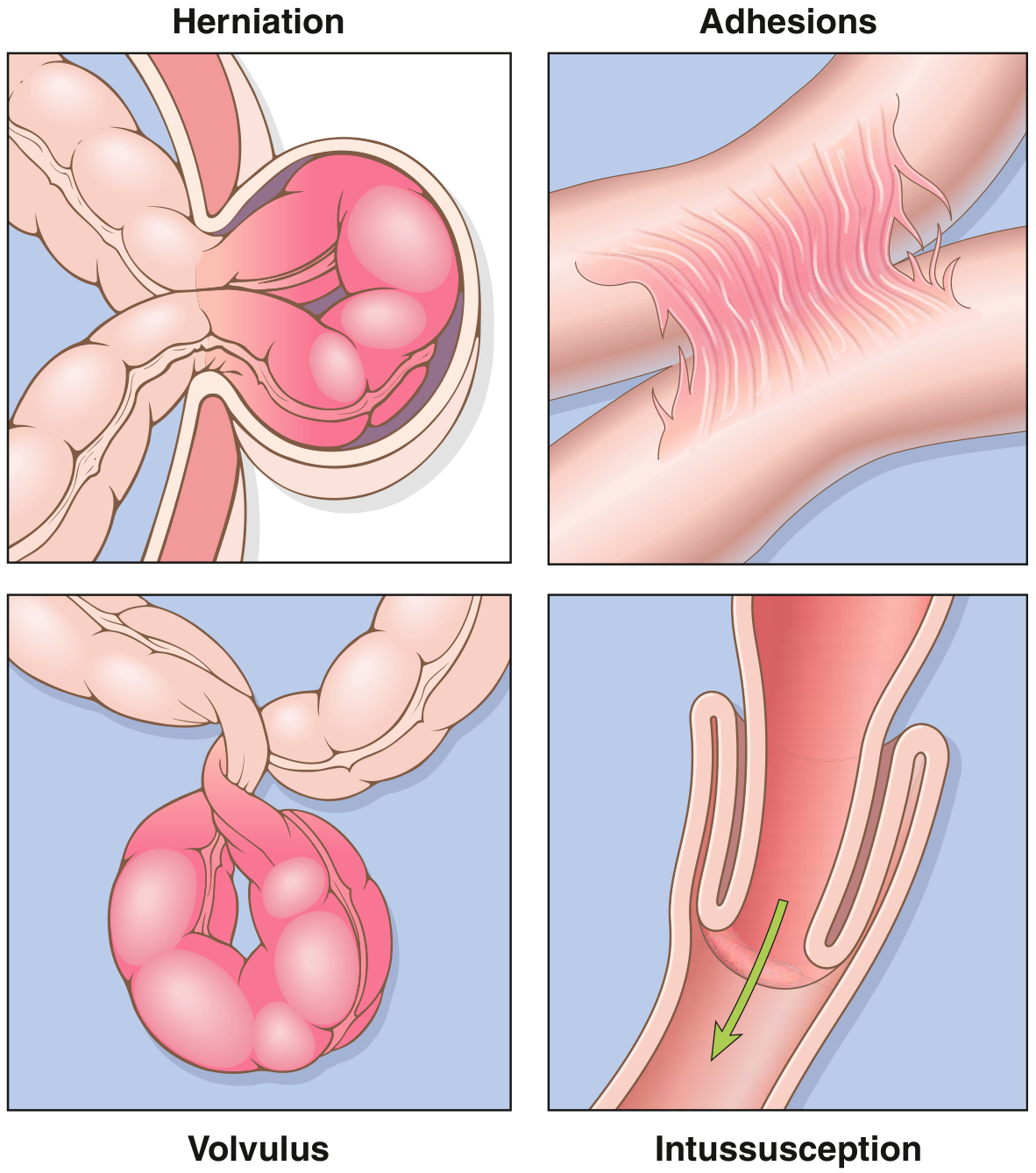
- Extrinsic — adhesions, hernias, peritoneal neoplasms
- Intrinsic (intramural) — primary neoplasms, Crohn's stricture, hematoma, radiation damage
- Intraluminal — bezoars, foreign bodies, gallstone ileus, fecal impaction
By Loop Dynamics
- Simple obstruction — obstruction at a single point; proximal decompression is possible
- Closed-loop obstruction — obstruction at two sites; no proximal escape; rapidly leads to ischemia and necrosis; mortality is twice that of simple SBO
Small Bowel Obstruction (SBO)
Epidemiology
- Accounts for the majority of all bowel obstructions
- Responsible for ~2% of all ED visits for abdominal pain
- Approximately 300,000 hospitalizations/year in the U.S.
- Mortality has fallen from ~60% (1900) to <8% with modern management
Causes (in order of frequency)
| Cause | Frequency |
|---|---|
| Post-surgical adhesions | ~60% |
| Tumors | ~20% |
| Abdominal hernias | ~10% |
| Gallstone ileus, volvulus, intussusception | remainder |
Special causes:
- Gallstone ileus: Rare (1–4% of SBO); gallstone enters bowel via cholecystoduodenal fistula, migrates distally, lodges at the ileum (narrowest segment). Most common in elderly patients.
- Small bowel volvulus: Rare in the West (3–6%); commoner in Africa/India/Middle East (up to 20%). Closed-loop → strangulation risk is high. Surgical emergency.
- Intussusception: Most common cause of obstruction in children 6–36 months. In adults, a mechanical cause (often tumor) is found in >90% of cases.
- Obturator hernia: Rare; older, thin women; no external mass → diagnosis frequently delayed; highest mortality (~70%) of any abdominal hernia when incarcerated.
Large Bowel Obstruction (LBO)
Epidemiology
- 4–5× less common than SBO in Western countries
- Affects an older population
- Patients present for medical attention on average 5 days after symptom onset (better tolerated than SBO due to slower distention)
Causes (~90% from 3 entities)
- Colorectal adenocarcinoma — most common cause in the USA; ~30% of CRC patients present obstructed; left-sided (distal to splenic flexure) tumors predominate because lumen is narrower and stool is more solid
- Colonic volvulus — 5–10% of LBO; sigmoid (75%) > cecal (22%); volvulus is the leading cause in developing countries
- Diverticular disease — fibrotic intramural stricture
Other causes: ischemic colitis, IBD (Crohn's/UC) strictures, anastomotic strictures, extraluminal compression (abscesses, adhesions, incarcerated hernias), non-colorectal primaries (~10% of malignant LBO).
Pathophysiology of LBO — Ileocecal Valve (ICV) Competence
- Competent ICV (75% of patients): colonic contents cannot decompress into small bowel → closed-loop obstruction → rapid ischemia and perforation risk
- By the Law of LaPlace: wall tension = intraluminal pressure × radius. The cecum (widest, thinnest wall) is most vulnerable to ischemia and rupture
- Critical cecal diameter: 10–13 cm (perforation risk is significant)
- Cecal dilation >12–14 cm on plain film = surgical emergency
- Incompetent ICV: contents back up into small bowel → massive distension, feculent emesis over weeks to months
Pathophysiology (General)
- Obstruction → intraluminal accumulation of GI secretions (gastric, biliary, pancreatic) continues even without oral intake
- Distention → increased intraluminal pressure → enhanced peristaltic contractions, air swallowing
- Vomiting + reduced intake + decreased absorption → volume depletion, hemoconcentration, electrolyte imbalance, renal failure, shock
- When intraluminal pressure exceeds capillary/venous pressure → bowel wall ischemia, decreased lymphatic drainage
- Bacterial overgrowth, translocation → septicemia and bowel necrosis
- This cascade accelerates in closed-loop obstruction
Clinical Features
| Feature | SBO | LBO |
|---|---|---|
| Pain | Colicky, periumbilical, early | Colicky, less severe; later onset |
| Vomiting | Early and prominent | Late finding |
| Distention | Moderate | Marked |
| Constipation/obstipation | Present | Predominant symptom |
| Bowel sounds | High-pitched, hyperactive early → absent | Variable |
Strangulation warning signs: fever, localized peritoneal signs (rebound, guarding), tachycardia, leukocytosis → suggest ischemia/necrosis → urgent surgery
Diagnosis
Plain Abdominal X-Ray
- SBO: dilated small bowel loops with air-fluid levels on upright film; "stepladder" pattern; absence of colonic gas
- LBO: dilated colon peripheral/frame-like; cecal distention
- Combination of upright + supine films: excellent sensitivity for LBO but lower specificity (cannot reliably distinguish from ileus/pseudo-obstruction)
- Colonic loop ≥6 cm or cecal diameter ≥9 cm = dilated
CT Scan (imaging of choice)
- Identifies transition point, cause, and complications (ischemia, perforation)
- Malignant obstruction features: mass at obstruction site, adenopathy, abrupt transition zone with irregular bowel thickening
- Benign obstruction features: mesenteric vascular changes, large ascites, smooth transition zone, smooth bowel thickening
- CT enteroclysis: water-soluble contrast via naso-enteric tube followed by CT — useful for challenging low-grade SBO
- Signs of impending perforation: cecal dilation >10 cm, pneumatosis intestinalis, portal venous gas, pneumoperitoneum
Management
Initial Stabilization (all bowel obstruction)
- IV fluid resuscitation + electrolyte replacement
- Nasogastric (NG) decompression — relieves distension; may allow non-surgical resolution (especially adhesive SBO)
- NPO (bowel rest)
- Foley catheter for urine output monitoring
- Correct underlying metabolic abnormalities
SBO Management
Conservative (non-operative)
- Indicated for adhesive SBO (most common cause) — majority resolve without surgery
- Bowel rest, IV fluids, NG decompression, pain control
- Water-soluble contrast agents (e.g., Gastrografin) have both diagnostic and therapeutic roles — promote resolution and predict need for surgery
Surgical
- Indicated for: failed conservative management, suspected/confirmed strangulation, peritonitis, closed-loop obstruction, incarcerated/strangulated hernia, complete obstruction not responding to non-operative treatment
- Options: lysis of adhesions, bowel resection with/without anastomosis, hernia repair, enterostomy
LBO Management
Right-sided obstructing cancer: Right or extended right hemicolectomy, often with primary anastomosis; consider end ileostomy if patient is hemodynamically unstable, frail, or malnourished
Left-sided obstructing cancer (more complex):
- Resection + anastomosis with diverting ileostomy
- Resection + end colostomy (Hartmann's procedure)
- Diverting proximal colostomy alone (without resection)
- Endoscopic stenting — bridge to surgery (decompression + bowel prep → elective single-stage resection) OR palliative (in advanced disease)
- Risk of perforation, occlusion, migration; requires experienced endoscopist
Sigmoid volvulus: Endoscopic/sigmoidoscopic decompression first; surgical resection if this fails or if signs of ischemia/perforation
Cecal volvulus: Usually requires surgical intervention (right hemicolectomy or cecopexy)
Malignant Bowel Obstruction (palliative)
Pharmacological management for inoperable obstruction:
- Opioids for abdominal pain
- Antiemetics (dopamine antagonists: phenothiazines, butyrophenones) for nausea
- Antisecretory agents (anticholinergics, octreotide) — reduce colicky pain and intestinal secretions
- Glucocorticoids — anti-inflammatory; may assist resolution
- Metoclopramide — cautiously for incomplete/functional obstruction only; contraindicated in complete obstruction
- NG tube relief or venting gastrostomy for prolonged palliation
Special Entities
Strangulated Bowel Obstruction
- Compromise of bowel blood supply → ischemia → necrosis → perforation
- Clinical: fever, tachycardia, severe unrelenting pain, peritonism, leukocytosis
- Mortality doubles compared to simple obstruction
- Surgical emergency
Intussusception
- Telescoping of a bowel segment into the distal segment
- Children <2 years: usually idiopathic (often linked to Peyer patch hyperplasia, adenovirus); treated with contrast enema reduction
- Adults: >90% have a mechanical lead point (tumor in >65%); requires surgery
- Complications: obstruction, mesenteric vessel compression, infarction
Hirschsprung Disease
- Congenital aganglionic megacolon (1:5000 live births); males > females
- Failure to pass meconium in neonatal period → obstructive constipation
- Complications: enterocolitis, perforation, electrolyte disturbances
- Treatment: surgical resection of aganglionic segment + anastomosis
Adynamic Ileus vs. Mechanical Obstruction
| Feature | Adynamic Ileus | Mechanical Obstruction |
|---|---|---|
| Cause | Post-op, infection, metabolic (hypokalemia), drugs | Adhesion, hernia, tumor, volvulus |
| Bowel sounds | Absent/quiet | Hyperactive initially → absent |
| Gas pattern | Gas throughout small + large bowel | Dilated loops proximal to obstruction; collapsed distal |
| Treatment | Conservative (treat underlying cause) | Often surgical |
Key Numbers to Remember
| Parameter | Value |
|---|---|
| Most common SBO cause | Adhesions (~60%) |
| SBO mortality (modern) | <8% |
| LBO vs. SBO frequency | LBO is 4–5× less common |
| Colorectal cancer presenting obstructed | ~30% |
| Sigmoid:cecal volvulus ratio | ~75%:22% |
| Competent ICV frequency | ~75% of patients |
| Critical cecal diameter (perforation risk) | 10–13 cm |
| Surgical emergency cecal dilation | >12–14 cm |
| Malignant bowel obstruction median survival | 3–4 months |
| Obturator hernia incarceration mortality | ~70% |
Sources: Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Current Surgical Therapy 14e; Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.