Thyroid auto antibodies in detail according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed from multiple ENT and surgical textbooks. Let me compile the comprehensive answer.
Thyroid Autoantibodies - According to Standard ENT Textbooks
(Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Cummings Otolaryngology Head and Neck Surgery, K.J. Lee's Essential Otolaryngology, Bailey and Love's Short Practice of Surgery)
Overview and Clinical Rationale
Measurement of serum thyroid antibodies confirms the aetiology of thyroid dysfunction, but two important caveats apply:
- Thyroid antibodies are found in approximately 10% of the healthy, euthyroid population
- Measurement is only indicated clinically if it alters management - for example, if radioiodine is planned, it matters little whether TSH-receptor antibodies are positive; but it would be futile to use a course of antithyroid drug treatment expecting a cure in a hyperthyroid patient unless Graves' disease is firmly established
(Scott-Brown's Vol 1)
Classification of Thyroid Autoantibodies
There are three clinically relevant groups:
1. Anti-Thyroid Peroxidase (Anti-TPO) Antibodies
Previously called Antimicrosomal Antibodies (AMA)
Target antigen: Thyroid peroxidase (TPO), a microsomal enzyme critical for iodine organification and thyroid hormone synthesis
Key facts:
- Originally measured by immunofluorescence or haemagglutination methods; now measured by sensitive immunoassays calibrated against standard sera
- Detectable in >90% of patients with chronic autoimmune thyroid disease
- Present in ~100% of patients with Hashimoto thyroiditis
- Present in >80% of patients with Graves' disease
- Positive in approximately 15% of adults in the general population (especially women)
- The term anti-TPO has become interchangeable with "antimicrosomal antibody (AMA)" since the introduction of immunoassay techniques
Clinical significance:
- Most useful screening antibody for autoimmune thyroid disease - more sensitive than anti-Tg for this purpose
- Significant threshold: >25 units/mL (Bailey & Love)
- Positive AMA titer should alert the clinician to possibility of hypothyroidism
- Individuals with positive AMA + elevated TSH (even subclinical hypothyroidism) have a 3-5% per year likelihood of developing clinical hypothyroidism
- If isolated elevated TSH or isolated TPO antibodies: annual risk of progression to overt hypothyroidism = 2% per year
- If both elevated TSH and positive TPO antibodies: annual risk = 5% per year
- Positive TPO antibodies predict higher risk of hypothyroidism after amiodarone, alpha-interferon, or other immune-modulating drug treatment
- Also elevated in other organ-specific autoimmune diseases: SLE, rheumatoid arthritis, autoimmune anaemia, Sjogren syndrome, Type 1 diabetes, Addison disease
(Cummings; Scott-Brown's Vol 1)
2. Anti-Thyroglobulin (Anti-Tg / TgAb) Antibodies
Target antigen: Thyroglobulin (Tg) - the glycosylated protein that serves as substrate for biosynthesis and storage of thyroid hormones
Key facts:
- Measured by immunofluorescence/haemagglutination originally; now by immunoassays
- Less sensitive than anti-TPO for diagnosing autoimmune thyroid disease
- More specific than anti-TPO
- Almost all patients with autoimmune thyroid disease who have Tg antibodies also have TPO antibodies - but the reverse is much less common; hence some laboratories offer only TPO antibody measurement to screen for autoimmune thyroid disease
- Prevalence in general population: ~10%; prevalence in patients with differentiated thyroid cancer (DTC): up to 25%
- Significant threshold: titre >1:100 (Bailey & Love)
Critical clinical interference - Thyroid Cancer Follow-up:
- TgAb interfere with the ability to accurately measure and follow serum Tg trends
- Anti-Tg antibodies are present in 15-25% of differentiated thyroid cancer (DTC) patients vs ~10% in the general population
- They cause falsely low or undetectable Tg values when immunometric Tg assays are used - a major pitfall in post-thyroidectomy surveillance
- Therefore, Tg and TgAb must always be measured concurrently in thyroid cancer follow-up
- Rising TgAb trend may indicate disease relapse even when Tg itself appears undetectable
- A declining TgAb level over time is a good prognostic sign in DTC
- Serum Tg measurement is only reliable in the absence of TgAb
- Presence of TgAb has been associated with higher risk of malignancy in patients presenting with a thyroid nodule
Diagnosis of factitious thyrotoxicosis: Serum Tg is low in factitious thyrotoxicosis (as opposed to elevated in other causes), and TgAb must be excluded as a confounding factor.
(Scott-Brown's Vol 1, Cummings)
3. TSH Receptor Antibodies (TRAb / TSH-RAb)
Target antigen: TSH receptor on thyroid follicular cells
Historical note: The immunopathogenesis of Graves' disease was first suspected in the mid-1950s when injecting sera of Graves' disease patients into rats produced prolonged radioactive iodine uptake in the rat thyroid - hence the term Long-Acting Thyroid Stimulator (LATS). LATS was later characterized as a 7S immunoglobulin.
Types of TRAb:
There are two functionally distinct types:
| Type | Effect | Disease Association |
|---|---|---|
| Stimulating TRAb (TSI - Thyroid-Stimulating Immunoglobulins) | Activates TSH receptor → TSH-like activity → hyperthyroidism | Graves' disease (hyperthyroid form) |
| Blocking TRAb (TBII - TSH-Binding Inhibitory Immunoglobulins) | Blocks TSH receptor → hypothyroidism | Atrophic autoimmune hypothyroidism |
Measurement methods:
- Bioassay (cAMP-generating / functional assay): Measures ability of immunoglobulins to generate cAMP in thyroid cells. The assay is termed Thyroid-Stimulating Immunoglobulin (TSI) - detectable in 90-95% of hyperthyroid Graves' disease patients
- Radioreceptor (binding) assay: Measures TSH-binding inhibitory properties - detects both stimulating and blocking antibodies; termed TBI antibodies - detected in 85% of hyperthyroid Graves' disease patients
New immunoassays for TSH-receptor antibodies have sensitivities of approximately 95% with nearly 100% specificity for Graves' disease. Although these assays do not distinguish between stimulating and blocking antibodies, the clinical and biochemical picture makes the distinction:
- Thyrotoxicosis + positive TSH-receptor antibodies = Graves' disease (stimulating)
- Hypothyroidism + positive TSH-receptor antibodies = blocking antibodies
- Occasionally patients switch from one type to the other, causing a bewildering pendulum swing from hyper- to hypothyroidism (or vice versa)
TRAb in Graves' Disease (clinical importance):
- Pathognomonic for Graves' disease
- Detectable in approximately 98% of untreated patients with Graves' disease (Cummings)
- Rules out other causes of thyrotoxicosis - very helpful when the clinical picture is not clear
- Associated with orbitopathy: TSH-R (TSHR) is the primary auto-antigen; level of TSI correlates with activity of both thyroid disease and orbitopathy (K.J. Lee's)
- High levels in pregnant women with Graves' disease predict neonatal thyrotoxicosis due to transplacental transfer of IgG antibodies
- Current guidance recommends determination of TSH-receptor antibody concentrations at 20 weeks' gestation in pregnant women with Graves' disease, with close monitoring of those with high titres
- TSH-receptor autoantibodies decline during the second half of pregnancy, often leading to remission of Graves' disease
When to measure TRAb:
- Not indicated for routine evaluation of suspected Graves' disease
- Indicated when the diagnosis of Graves' disease is not clinically evident and confirmation is required before committing to antithyroid drug therapy (aiming for remission)
- In pregnancy - to predict risk of fetal/neonatal thyrotoxicosis
- When distinguishing between stimulating vs blocking antibody-driven thyroid disease
(Cummings; Scott-Brown's Vol 1; K.J. Lee's)
Summary Table: Thyroid Autoantibodies at a Glance
| Antibody | Target | Significant Level | Sensitivity | Key Disease | Key Clinical Use |
|---|---|---|---|---|---|
| Anti-TPO (AMA) | Thyroid peroxidase | >25 U/mL | >90% autoimmune TD; ~100% Hashimoto's | Hashimoto thyroiditis; Graves' | Screen for autoimmune thyroid disease; risk of hypothyroidism |
| Anti-Tg (TgAb) | Thyroglobulin | Titre >1:100 | Less sensitive than TPO | Hashimoto thyroiditis | Thyroid cancer surveillance; presence invalidates Tg measurement |
| TRAb / TSI | TSH receptor | - | ~95-98% Graves' | Graves' disease | Diagnosis of Graves'; neonatal thyrotoxicosis risk; orbitopathy correlation |
Prevalence Data (from Cummings - NHANES III)
- Thyroid peroxidase antibodies elevated in 11.3% of the general population
- Thyroglobulin antibodies elevated in 10.4% of the general population
- TPO antibody positivity was associated with both hypothyroidism and hyperthyroidism; thyroglobulin antibodies alone were not associated with either
- Approximately 15% of adults in the United States, especially women, have elevated AMA/anti-TPO titres
- Prevalence of positive AMA titres increases with age, as does the incidence of primary hypothyroidism
Risk Stratification for Progression to Hypothyroidism
The figure below (from the Whickham Survey, cited in Scott-Brown's) illustrates how the probability of developing overt hypothyroidism increases in proportion to the initial TSH level, with an additional risk conferred by having positive thyroid autoantibodies:
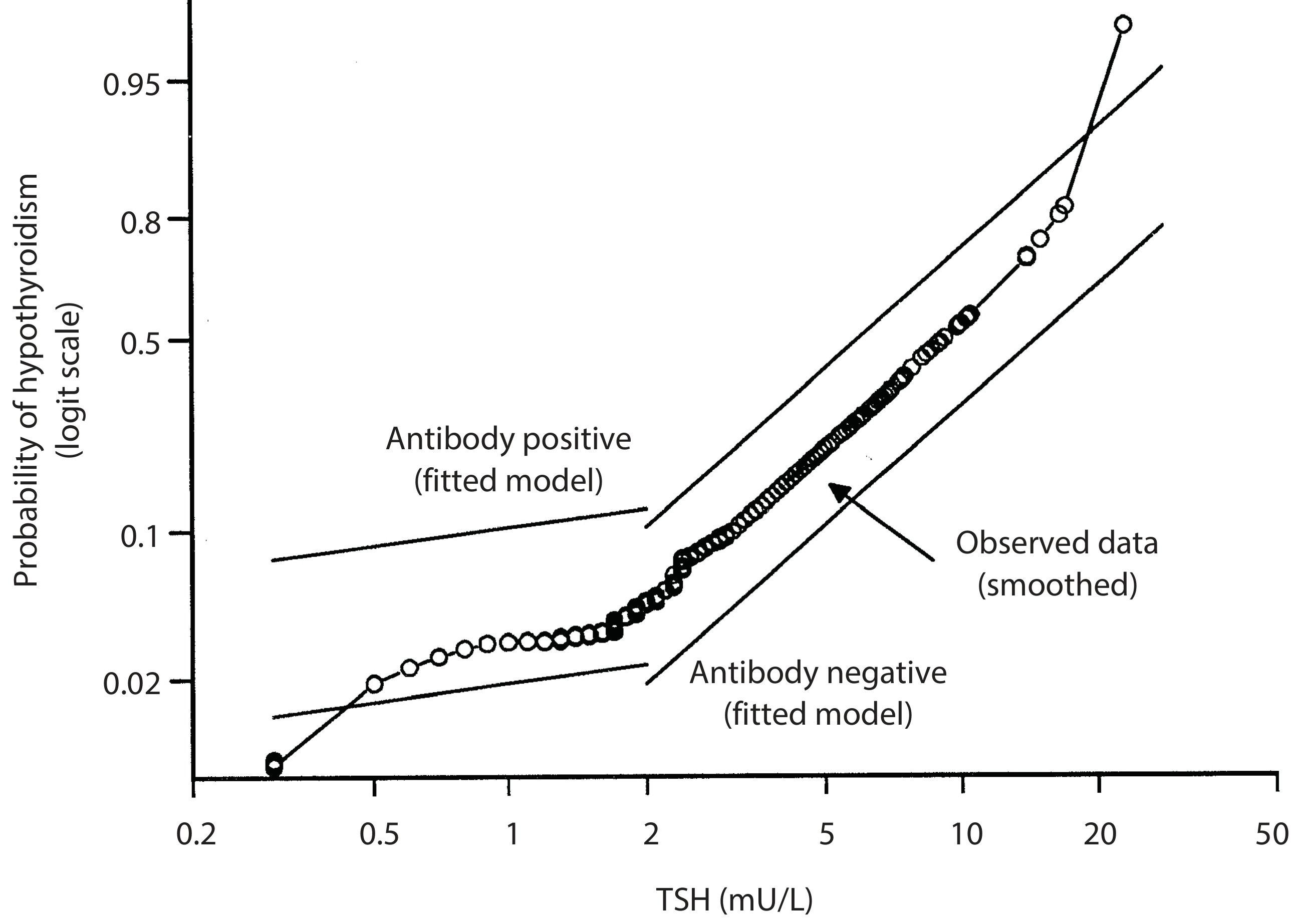
Figure: Probability of developing overt hypothyroidism. The antibody-positive line sits significantly above the antibody-negative line at all TSH values. (Vanderpump et al., Whickham Survey - cited in Scott-Brown's Otorhinolaryngology)
ENT-Specific Relevance of Thyroid Autoantibodies
| ENT Condition | Relevant Antibody | Significance |
|---|---|---|
| Hashimoto thyroiditis | Anti-TPO (elevated); Anti-Tg (elevated) | Diagnostic; may cause goitre, hoarseness, sensorineural hearing loss, vertigo |
| Graves' disease / orbitopathy | TRAb/TSI | Pathognomonic; level correlates with orbitopathy activity |
| Sensorineural hearing loss in hypothyroidism | Anti-TPO | Worsens with severity of hypothyroidism; bilateral, progressive |
| Hoarseness in hypothyroidism | Anti-TPO | Mucopolysaccharide infiltration of vocal cords; resolves with thyroxine |
| Differentiated thyroid cancer surveillance | TgAb | Interferes with Tg measurement; rising trend indicates relapse |
| Thyroid lymphoma | Anti-TPO | Arises from Hashimoto thyroiditis background |
| Subclinical hypothyroidism (endocrine follow-up) | Anti-TPO | ATA guidelines support treatment in TPO-positive women |
| Neonatal thyrotoxicosis | TRAb (maternal) | Transplacental transfer; check at 20 weeks gestation |
Summary Box (Bailey & Love's)
Essential thyroid investigations include:
- Serum TSH (T3 and T4 if abnormal)
- Thyroid autoantibodies (Anti-TPO and Anti-Tg)
- FNAC of palpable discrete swellings
A proportion of patients with histological evidence of lymphocytic (autoimmune) thyroiditis are seronegative - negative antibodies do not exclude autoimmune thyroid disease.
(Bailey & Love's Short Practice of Surgery, 28th Ed.; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Cummings Otolaryngology; K.J. Lee's Essential Otolaryngology)
This is a shared conversation. Sign in to Orris to start your own chat.