Psvt
Reading File
Finding Sources
Searching PubMed
"paroxysmal supraventricular tachycardia" management
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Here is a comprehensive overview of PSVT from multiple authoritative textbooks:
Paroxysmal Supraventricular Tachycardia (PSVT)
Definition
PSVT is a clinical syndrome characterized by a rapid, regular tachycardia with abrupt onset and termination. It encompasses all tachyarrhythmias that originate from or incorporate supraventricular tissue (above the bundle of His) in a reentrant circuit.
- Fuster and Hurst's The Heart, 15th Edition
Mechanisms / Types
| Type | Frequency |
|---|---|
| AV Nodal Reentrant Tachycardia (AVNRT) | ~65-80% of cases |
| AV Reentrant Tachycardia (AVRT) via accessory pathway (e.g., WPW) | ~15-30% |
| Atrial tachycardia (ectopic atrial focus) | ~5% |
- AVNRT: Reentry within the AV node using a slow and fast pathway. The most common mechanism.
- AVRT (orthodromic): Antegrade conduction via the AV node; retrograde via an accessory pathway - produces narrow QRS.
- AVRT (antidromic): Antegrade via accessory pathway - produces wide QRS (preexcited tachycardia).
- Harrison's 22E; Fuster and Hurst's The Heart
Epidemiology
- Incidence ~35 cases per 100,000 person-years; prevalence ~2.25 per 1,000
- More frequent in females (2:1 ratio for AVNRT)
- Peak onset in late teenage and young adult years (emergency medicine) or beyond the 4th decade for AVNRT specifically
- Majority of patients have no active cardiovascular disease
- Fuster and Hurst's The Heart; Tintinalli's Emergency Medicine
ECG Features
ECG of PSVT - regular narrow-complex tachycardia:

Key ECG findings (from Tintinalli's Emergency Medicine):
- Absence of normal sinus P waves (no normal P wave with normal PR interval)
- Narrow QRS complex (<100 ms) - unless aberrant conduction
- Rate: typically 170-180 bpm; range 130-300 bpm
- P waves buried within the QRS in ~70% of cases
- Retrograde P waves (inverted, immediately adjacent to QRS) in ~30%
- Regular rhythm
Clinical Presentation
- Palpitations (most common), lightheadedness, dyspnea
- Abrupt onset and termination - patients can often identify the exact moment it starts and stops
- Usually hemodynamically stable, but can cause presyncope/syncope
- Associated with WPW syndrome in some cases (up to 50% of WPW patients develop paroxysmal tachyarrhythmias)
Acute Management
Treatment algorithm:
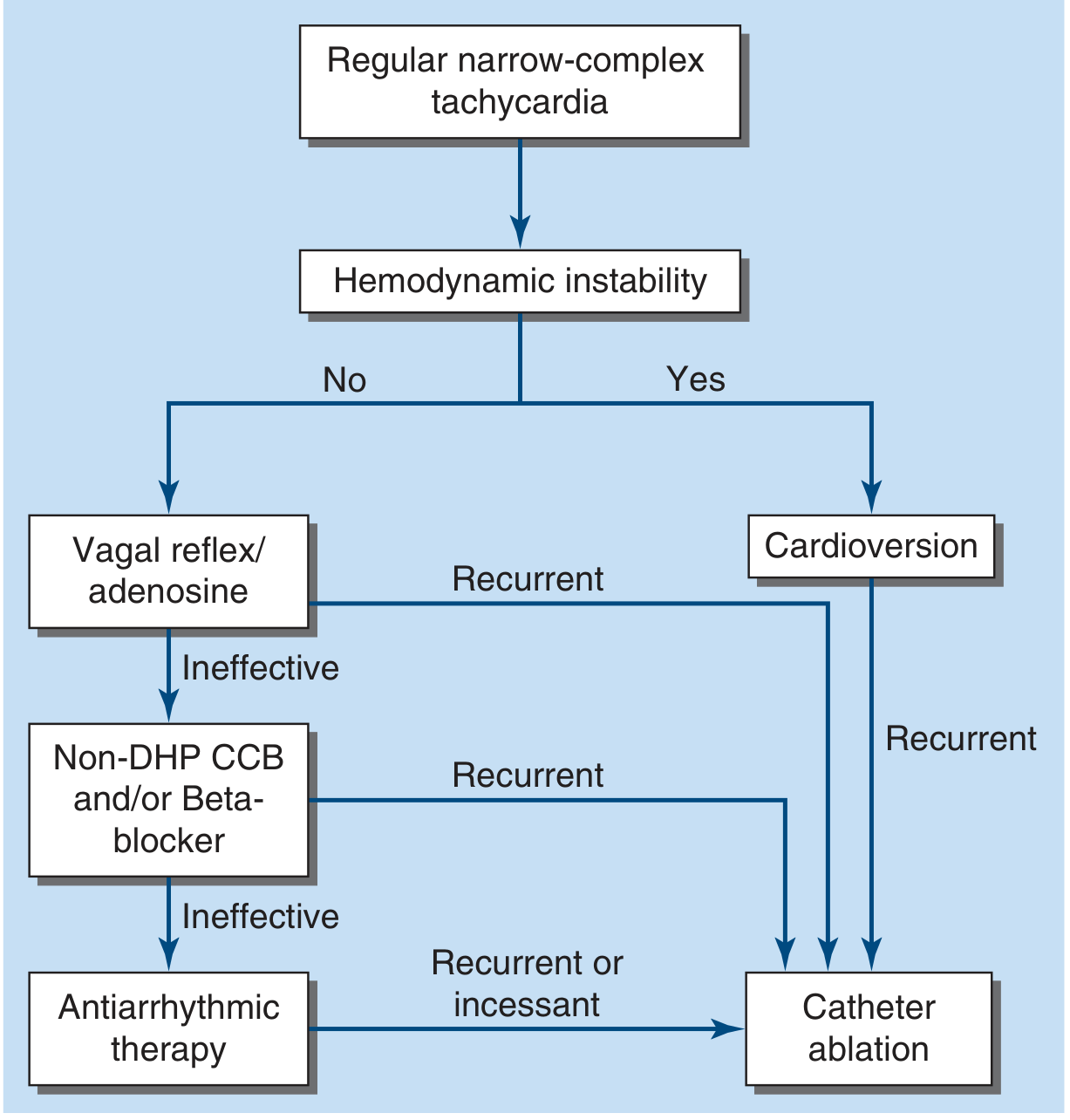
Step 1: Assess hemodynamic stability
- Unstable (hypotension, unconsciousness, respiratory distress): Synchronized DC cardioversion immediately
- For PSVT/atrial flutter: initial energy 50-100 J
Step 2: Stable patient - Vagal Maneuvers
- Carotid sinus massage - only if no carotid bruits or prior stroke history
- Valsalva maneuver - effective and patient can be taught self-administration
- Apply early in the dysrhythmia for best results
Step 3: IV Adenosine (first-line drug)
- Terminates the vast majority of PSVT by transiently blocking AV nodal conduction
- Side effects: transient chest pain, dyspnea, anxiety (very short half-life ~10 sec)
- Contraindicated in prior cardiac transplant (hypersensitivity due to denervation)
- Use caution in WPW - adenosine can precipitate AF in up to 15% of patients, which may cause hemodynamic instability in WPW
- Use caution in asthma/bronchospasm
Step 4: If adenosine fails - AV nodal blocking agents
- IV beta-blockers or non-DHP calcium channel blockers (verapamil, diltiazem)
- Effective but may cause hypotension; longer duration of action
- Can also be given orally on an as-needed basis ("pill in pocket") combined with Valsalva
Wide-Complex PSVT
- Differential: ventricular tachycardia (VT), PSVT with bundle branch block aberrancy, preexcited tachycardia
- Default: treat as VT until proven otherwise
- If regular, patient stable, trial of IV adenosine is reasonable
- Very irregular wide-complex tachycardia = likely preexcited AF/flutter → manage with cardioversion, IV procainamide, or ibutilide
- Harrison's 22E
Long-Term / Chronic Management
- Most patients with recurrent PSVT are candidates for catheter ablation
- Success rates very high (>95% for AVNRT)
- Antiarrhythmic drug therapy for patients unwilling or unsuitable for ablation
- Harrison's 22E; Fuster and Hurst's The Heart
Summary Table
| Feature | PSVT |
|---|---|
| Rate | 130-300 bpm (typically ~170-180) |
| Rhythm | Regular |
| QRS | Narrow (<100 ms); wide if aberrancy or preexcitation |
| P waves | Buried or retrograde |
| Onset/offset | Abrupt |
| Most common mechanism | AVNRT (65-80%) |
| First-line acute Rx | Vagal maneuvers → Adenosine |
| Unstable Rx | Synchronized cardioversion |
| Long-term Rx | Catheter ablation |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Tintinalli's Emergency Medicine | Fuster and Hurst's The Heart, 15th Ed. | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.