Research hierarchical pyramid and RCT in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
evidence hierarchy pyramid levels of evidence research study design 2024
Finding Sources
Finding Sources
Searching PubMed
evidence hierarchy pyramid levels clinical research
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed response.
The Evidence Hierarchy Pyramid and Randomized Controlled Trials (RCTs)
Part 1: The Hierarchy of Evidence (Evidence Pyramid)
The evidence hierarchy - often visualized as a pyramid - is a framework that ranks study designs by their ability to minimize bias and yield valid, reliable results. Those designs that limit bias to the greatest extent sit at the pinnacle of the pyramid; those that are inherently prone to bias occupy the base.
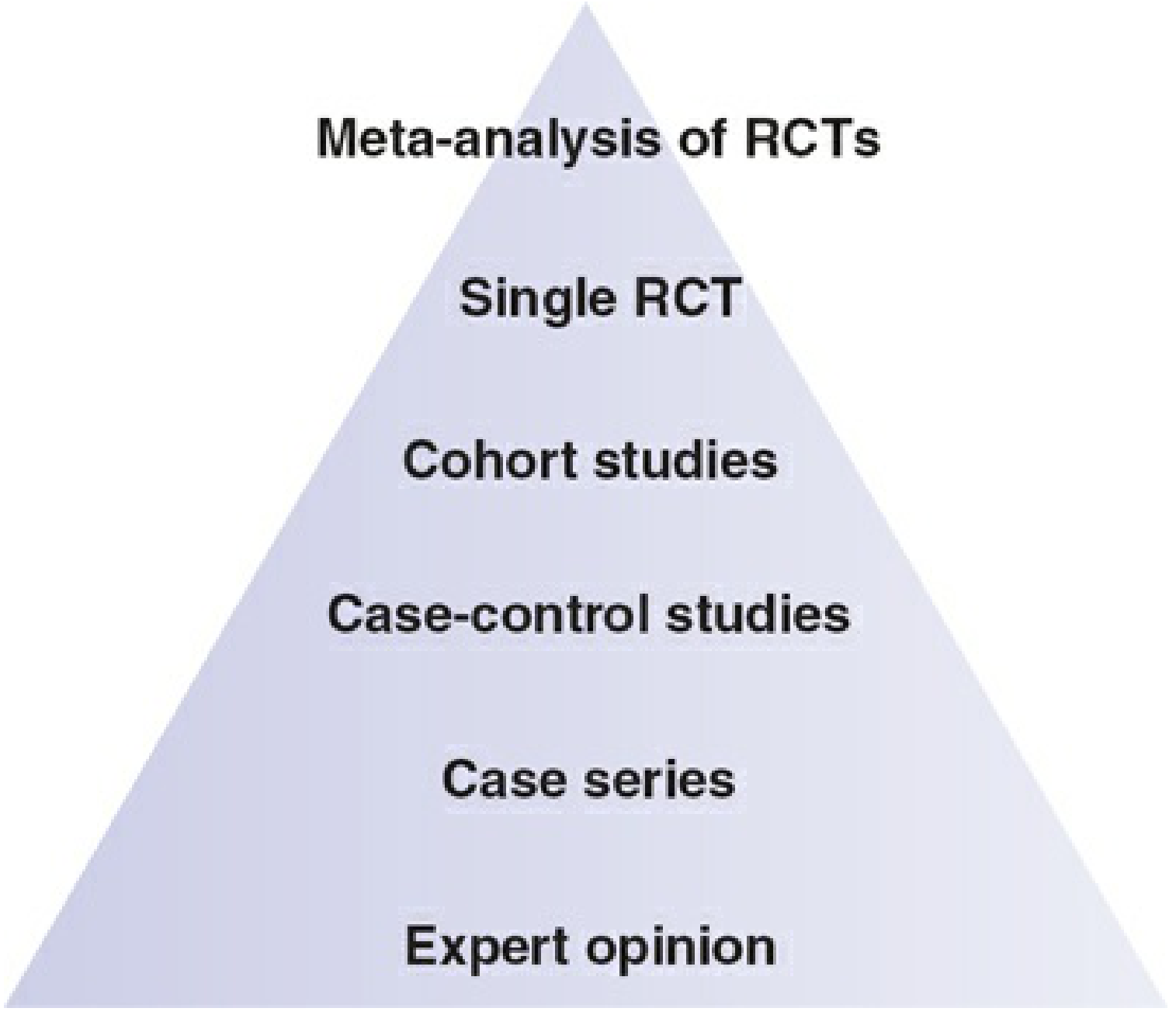
Figure: The hierarchy of evidence with meta-analysis of RCTs at the top and expert opinion at the bottom. - Rockwood and Green's Fractures in Adults, 10th ed. (2025)
The Levels - From Top to Bottom
Level I - Systematic Reviews and Meta-Analyses of RCTs (Highest)
Systematic reviews comprehensively summarize the available evidence using predefined, reproducible, explicit search strategies and inclusion/exclusion criteria. They seek to find all relevant scientific research and grade its quality. When appropriate, a meta-analysis is used to quantitatively pool the results of multiple trials. The prototype resource is the Cochrane Database of Systematic Reviews.
- The validity of a meta-analysis hinges on two factors:
- Credibility: how methodologically robust the systematic review and meta-analysis process itself is
- Certainty: how trustworthy the pooled effect sizes are - a reflection of the quality of the primary studies included
- A meta-analysis is most persuasive when it includes several large, properly conducted RCTs
- Meta-analyses can detect benefits that individual, underpowered trials cannot
Important caveat: Systematic reviews are not uniformly the highest form of evidence. Their value is limited when only a few trials are available, when trials and observational studies are mixed, or when the entire evidence base is observational. They cannot compensate for deficiencies in underlying research. - Harrison's Principles of Internal Medicine, 22nd ed. (2025)
Level II - Single Randomized Controlled Trial (RCT)
A single well-designed RCT provides the strongest primary (unfiltered) evidence. See Part 2 below for full detail.
Level III - Prospective Cohort Studies
Participants are followed forward in time without intervention. The investigator does not control patient care. Carefully collected prospective observational data can, through causal inference methods, approach RCT-level quality - but lacks protection from treatment selection bias (confounding by clinical indication).
Level IV - Case-Control Studies
Subjects with an outcome (cases) are compared retrospectively with those without (controls). The key effect measure is the odds ratio. Two major sources of systematic error:
- Selecting an appropriate control group
- Obtaining unbiased information about determinants
Case-control studies cannot estimate absolute occurrence of an outcome since no denominator information is available.
Level V - Cross-Sectional Studies and Case Series
- Cross-sectional studies capture a single time point ("snapshot")
- Case series: descriptive collections of individual cases without controls, useful for hypothesis generation only
Level VI - Case Reports
Single patient observations. Important for identifying rare adverse effects or novel presentations but not for causal inference.
Level VII - Expert Opinion / Mechanism-Based Reasoning (Lowest)
Textbook descriptions, expert committee reports, and physiological reasoning without empirical data. - Melnyk & Fineout-Overholt; Rockwood and Green's Fractures
The JBJS 5-Level System (Clinical Application)
The Journal of Bone and Joint Surgery (JBJS) has published the "level of evidence" for each article since 2003. It applies five levels across four study types:
| Level | Therapeutic | Prognostic | Diagnostic | Economic |
|---|---|---|---|---|
| I | RCT | Inception cohort | RCT / validated criteria | Monte Carlo model from Level I studies |
| II | Prospective cohort | Prospective cohort | Consecutive patients, blinded | Monte Carlo model from Level II studies |
| III | Retrospective cohort / case-control | Retrospective / case-control | Non-consecutive patients | Markov model, shorter time horizon |
| IV | Case series / historical controls | Case series | Poor reference standard | Decision tree, short horizon |
| V | Mechanism-based reasoning | Mechanism-based reasoning | Mechanism-based reasoning | Decision tree, prior economic data |
A caveat: one must appraise methodological rigor independently from hierarchy position. A small, poor-quality Level I RCT may be less valid than a large, well-designed Level II prospective cohort. - Rockwood and Green's Fractures in Adults (2025)
The GRADE System
The GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) framework provides more granularity than the traditional hierarchy because it grades quality based not just on study design, but also on:
| Factor | Direction |
|---|---|
| Serious or very serious limitation to study quality | Downgrade -1 or -2 |
| Important inconsistency across studies | Downgrade -1 |
| Uncertainty about directness (applicability) | Downgrade -1 or -2 |
| Imprecise or sparse data | Downgrade -1 |
| High probability of reporting bias | Downgrade -1 |
| Strong evidence of association (RR >2 from consistent observational studies, no confounders) | Upgrade +1 |
Starting grades: RCT = high quality; quasi-randomized = moderate; observational = low; any other = very low.
The GRADE approach considers risk of bias, precision, consistency, and applicability to arrive at certainty ratings of very low, low, moderate, or high. - Rockwood and Green's Fractures in Adults (2025)
Part 2: The Randomized Controlled Trial (RCT)
Definition and Core Concept
An RCT is a prospective cohort study with one defining feature: it uses a random allocation scheme to assign participants to the intervention ("treatment arm") or comparison ("control arm"). This distinguishes it from all other study designs.
"Randomized controlled trials are cohort studies with prospective data collection. Their distinctive feature is that they use a random allocation scheme to assign the determinant. With randomization, you can expect that the prognostic characteristics of the randomized groups or 'arms' of the trial are similar except for differences due to chance variation." - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Why Randomization Is Powerful
Randomization eliminates the influence of both known and unknown confounders that exist at the time of allocation. Without it, imbalances in prognostic factors between groups arise from selection bias - specifically "confounding by clinical indication" (sicker patients may preferentially receive one treatment).
No statistical adjustment method, however sophisticated, can fully replicate what randomization achieves mechanically. This is the core reason RCTs are positioned above observational studies in the hierarchy.
Key Design Features of RCTs
1. Allocation Concealment
The randomization process must be concealed from the investigators who include participants. Proper concealment means investigators do not know which arm a participant will be assigned to until that participant has definitively been enrolled. Without concealment, investigators can consciously or unconsciously influence group balance by selectively recruiting patients.
2. Blinding
Blinding prevents participants and/or investigators from knowing which treatment has been received. It prevents bias in three ways:
- Prevents participants' perceptions and expectations from influencing compliance and physiological response (e.g., placebo effect)
- Prevents investigators from managing participants differently based on group assignment
- Prevents outcomes from being assessed differently based on group knowledge
Types:
- Single-blind: only participants are blinded
- Double-blind: both participants and investigators are blinded
- Triple-blind: extends blinding to outcome assessors or statisticians
Double blinding is nearly impossible in surgical trials. In those cases, strategies include: standardizing co-interventions, using third-party blinded outcome assessors, using "hard outcomes" (e.g., death, objective measurements) resistant to bias, and having participants self-complete validated outcome scales. - Scott-Brown's Otorhinolaryngology
3. Placebo Control
A placebo is a treatment indistinguishable from the active intervention but with no known specific mechanism of action. Its use:
- Enables blinding
- Separates specific treatment effects from non-specific (placebo) effects
- Especially useful when measuring subjective outcomes (pain, quality of life)
Placebo controls are rarely feasible in surgical trials; "sham surgery" has been used in select contexts.
4. Equipoise
The ethical justification for randomization is equipoise - a state of genuine uncertainty about which treatment is superior. If there is true uncertainty, no patient is harmed by random assignment. Informed consent addresses patient preferences and risks.
5. Intention-to-Treat (ITT) Analysis
All randomized participants are analyzed in the group to which they were allocated, regardless of whether they received the intervention or deviated from protocol. ITT analysis preserves the benefits of randomization and gives an estimate of real-world effectiveness. Per-protocol analysis (restricted to compliers) gives an estimate of efficacy but can introduce bias.
6. Run-In Period
Some trials include a run-in phase before randomization to exclude non-compliant participants, allow washout of prior treatments, or achieve a stable baseline. This can improve internal validity but affects generalizability.
Phases of Clinical Trials
| Phase | Purpose | Typical N | Focus |
|---|---|---|---|
| Phase I | Safety, dosing, pharmacokinetics | 10-80 | "Is it safe?" |
| Phase II | Efficacy signal, dose optimization | 100-300 | "Does it work?" |
| Phase III | Definitive efficacy vs. comparator | 300-3000+ | "Is it better than standard?" |
| Phase IV | Post-marketing surveillance | Large populations | Long-term safety, rare AEs |
Phase III trials are the classic RCT used for regulatory approval and guideline development.
Internal Validity vs. External Validity (Generalizability)
Internal validity: The extent to which the trial results correctly reflect the true causal effect in the study population. Achieved through randomization, concealment, blinding, and minimizing dropouts.
External validity (generalizability): The extent to which results apply to patients outside the trial. RCTs often have restrictive inclusion/exclusion criteria, meaning recruited patients may not represent the broader population clinicians treat. - Harrison's Principles of Internal Medicine (2025)
An important tension: the features that maximize internal validity (strict eligibility criteria, close monitoring, ideal conditions) can reduce external validity.
Limitations of RCTs
- Ethical constraints: Cannot randomize patients to harmful exposures (smoking, obesity, inequitable access)
- Feasibility: Expensive, time-consuming, require large sample sizes
- External validity: Restrictive eligibility criteria limit generalizability
- Can't answer all questions: Rare outcomes, long latency diseases, or widely accepted treatments may not be suitable for RCTs
- Regulatory vs. practice design conflict: Trials designed for FDA approval (using placebo controls) may not reflect the comparators most useful to clinicians - Harrison's Principles of Internal Medicine (2025)
Summary Comparison Table
| Feature | RCT | Cohort Study | Case-Control | Case Series |
|---|---|---|---|---|
| Direction | Prospective | Prospective or retrospective | Retrospective | Descriptive |
| Randomization | Yes | No | No | No |
| Controls confounding | Best (known + unknown) | Partial (known only) | Partial | None |
| Effect measure | Risk ratio, hazard ratio | Risk ratio, HR | Odds ratio | None |
| Evidence level | I-II | II-III | III | IV |
| Cost/feasibility | High | Moderate | Lower | Low |
| Best used for | Intervention efficacy | Etiology, prognosis | Rare diseases | Hypothesis generation |
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. (2025) - Chapter 8: Evidence Hierarchy, GRADE System
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Evidence-Based Medicine, Clinical Trials, Meta-Analysis
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Fundamentals of Study Design, RCTs
- UC Davis Library - Levels of Evidence
- PMC: Conceptualizing the evidence pyramid (2024)
This is a shared conversation. Sign in to Orris to start your own chat.