Periocular and intraocular steroids
Reading File
Finding Sources
Finding Sources
Searching PubMed
periocular intraocular corticosteroids ophthalmic
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Periocular and Intraocular Steroids
Corticosteroids are among the most important pharmacological tools in ophthalmology, used across a spectrum of anterior and posterior segment inflammatory conditions. They can be delivered via several routes - topical, periocular (subconjunctival, subtenon, orbital floor), intravitreal (injection or implant), and systemic - each with distinct pharmacokinetics, indications, and risk profiles.
1. Topical Corticosteroids
Agents Available
| Drug | Key Feature |
|---|---|
| Prednisolone acetate 1% | Most potent topical; gold standard for anterior uveitis |
| Difluprednate 0.05% | Allows less frequent dosing than prednisolone acetate; more potent |
| Dexamethasone | Used for allergic and inflammatory conditions |
| Fluorometholone 0.1% | Lower IOP-raising potential; good for mild inflammation |
| Loteprednol etabonate | Soft steroid; metabolized locally; less IOP elevation risk |
| Rimexolone 1% | Reduced systemic absorption |
Indications
- Anterior uveitis (AAU and CAU)
- Postoperative inflammation (cataract, refractive, corneal surgery)
- Allergic conjunctivitis, dry eye syndrome, external ocular inflammation
- Episcleritis, scleritis (adjunctive)
- After glaucoma filtering surgery (to reduce fibroblast scarring of the bleb)
Dosing Regimen (for moderate-severe anterior uveitis)
- 1 drop hourly for 3 days
- Every 2 hours for 3 days
- 4x/day for 1 week
- 3x/day for 1 week
- 2x/day for 1 week
- Once daily for 1 week, then stop
- Treatment is typically completed by 5-6 weeks and carefully tapered
- Kanski's Clinical Ophthalmology, p. 453; Wills Eye Manual, p. 935
2. Periocular Steroids
Periocular injections deposit depot steroid close to the posterior segment without entering the eye. Two main approaches are used: inferior transseptal (orbital floor) and posterior sub-Tenon's capsule.
Drugs Used
- Triamcinolone acetonide 40 mg/mL - most common depot agent
- Methylprednisolone acetate 40 mg/mL
- Betamethasone (sodium phosphate + acetate suspension, 6 mg/mL) - for subconjunctival use
Dose
- Subtenon / orbital floor: 1 mL (40 mg triamcinolone) via 25-gauge needle
- Subconjunctival: 0.5-1.0 mL triamcinolone 40 mg/mL
- Peak action: ~4 weeks; duration: up to 3 months
Indications
- Posterior segment inflammation (intermediate/posterior/panuveitis)
- Cystoid macular edema (CMO) from uveitis or post-surgical
- Unilateral severe anterior uveitis not responding to topical therapy
- Patients non-compliant with topical drops
- Perioperative inflammation control (at time of surgery)
- When systemic steroids are contraindicated (supplement or replacement)
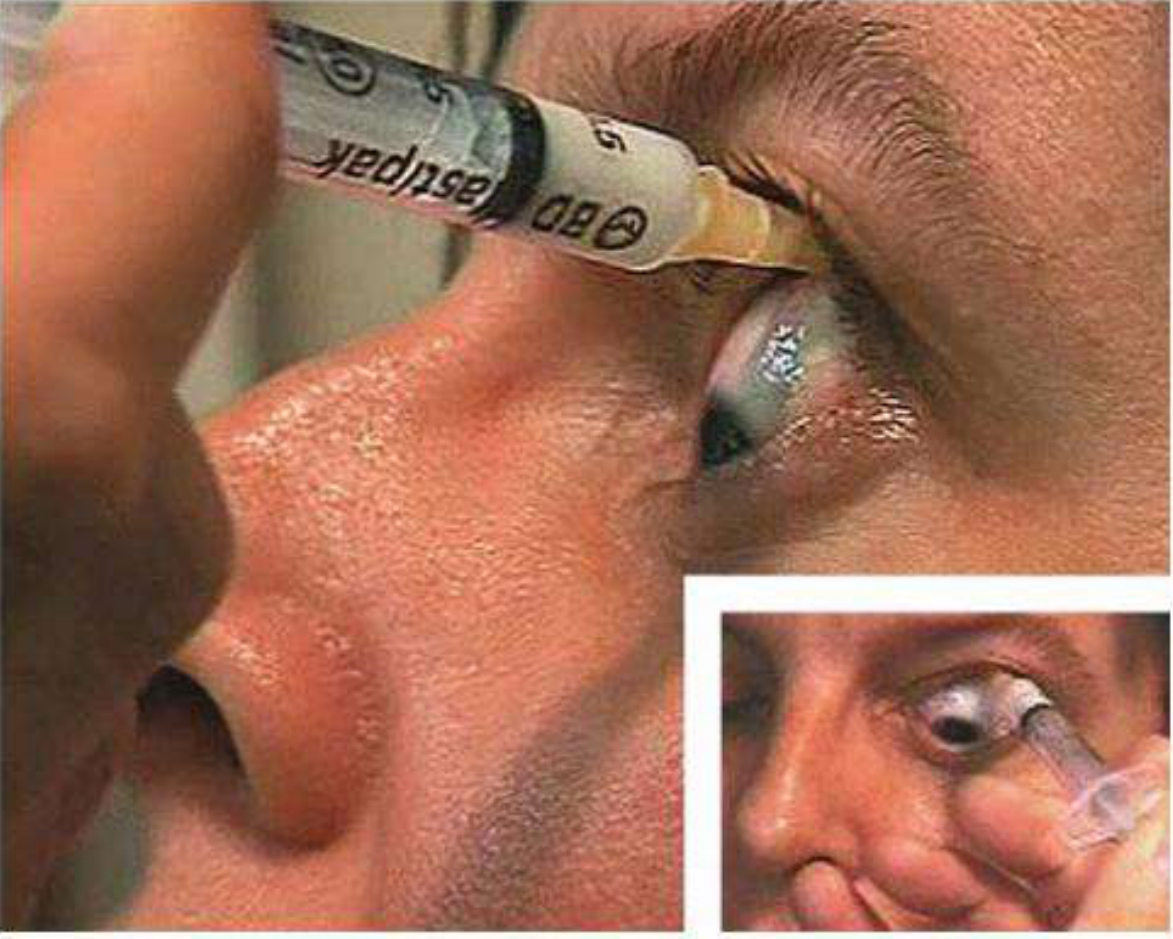
Technique - Inferior Transseptal (Orbital Floor) Approach
- Instill topical anesthetic (e.g., tetracaine)
- Clean lower eyelid skin with antiseptic (povidone-iodine 5%)
- Shake steroid vial; draw up 1 mL into 2 mL syringe with 25-gauge 5/8 inch needle
- Patient maintains straight-ahead gaze
- Needle inserted through skin near bony orbital margin, advanced tangentially to the globe
- Confirm no blood on aspiration, then inject full 1 mL slowly
Technique - Posterior Sub-Tenon Approach
- Topical anesthetic + cotton pledget in superior fornix for 2 minutes
- Patient looks in direction opposite to superotemporal injection site
- Bevel toward globe, pierce bulbar conjunctiva in superior fornix
- Advance posteriorly following globe contour - make side-to-side motions to confirm globe not engaged (limbal movement = sclera engaged - stop)
- Advance to needle hub, aspirate to confirm no blood, inject full 1 mL slowly
There is no clear evidence of superiority of one route over the other, but the orbital floor approach may have lower risk of globe perforation, IOP rise, and ptosis. - Kanski's, p. 454
Complications of Periocular Injection
- Subconjunctival hemorrhage
- Globe penetration (rare but serious)
- Refractory IOP elevation (up to 25%)
- Cataract
- Ptosis
- Eyelid hemorrhage / ischemic necrosis
- Retrobulbar hemorrhage
- Subdermal fat atrophy
- Extraocular muscle paresis
- Optic nerve injury
- Retinal/choroidal vascular occlusion
- Cutaneous hypopigmentation
- Systemic absorption (rare)
Important: Periocular depot steroids should be used with extreme caution in scleritis due to risk of scleral melting. Always rule out infectious uveitis before injecting. - Wills Eye Manual, p. 935
Periocular triamcinolone is off-label and must be discussed with patients. A trial of full-strength topical steroids helps identify steroid responders before committing to depot injection. - Wills Eye Manual, p. 935
3. Intraocular (Intravitreal) Steroids
A. Intravitreal Triamcinolone Acetonide (IVTA)
- Dose: 4 mg in 0.1 mL (i.e., one-tenth of the orbital periocular dose)
- FDA-approved for ocular inflammatory conditions unresponsive to topical corticosteroids and for visualization during vitrectomy
- IOP elevation typically lasts 2-4 months post-injection
Indications:
- CMO unresponsive to periocular steroids or other therapy
- Diabetic macular edema (DME)
- Macular edema from retinal vein occlusion
- Posterior/panuveitis
- Rarely, high-risk anterior uveitis patients at the time of intraocular surgery
Complications:
- Elevation of IOP
- Posterior subcapsular cataract
- Endophthalmitis (sterile or infectious)
- Intraocular hemorrhage
- Retinal detachment
- Pseudohypopyon (settling of triamcinolone crystals in anterior chamber)
- Kanski's Clinical Ophthalmology, p. 454; Goodman & Gilman's, p. 976
B. Sustained-Release Intravitreal Implants
These devices allow prolonged drug delivery, avoiding repeated injections:
| Implant | Drug | Dose | Duration | Indication |
|---|---|---|---|---|
| Ozurdex (dexamethasone implant) | Dexamethasone | 0.7 mg biodegradable | Up to 6 months | Uveitis, DME, macular edema from RVO |
| Yutiq / Iluvien (fluocinolone acetonide) | Fluocinolone acetonide | 0.19 mg (Yutiq) / 0.59 mg (Iluvien) | 3 years | Chronic noninfectious uveitis, DME |
| Retisert (fluocinolone acetonide) | Fluocinolone acetonide | 0.59 mg surgically placed | Up to 3 years | Chronic noninfectious posterior uveitis |
Intravitreal preservative-free triamcinolone and the dexamethasone/fluocinolone implants are more effective for uveitic macular edema than periocular triamcinolone. - Wills Eye Manual, p. 943
4. Steroid-Induced Complications (Relevant to All Routes)
Steroid-Induced Glaucoma
- ~1 in 3 individuals show some IOP rise to potent topical steroids ("steroid responders")
- Secondary open-angle glaucoma with normal-appearing angle
- Mechanism: increased resistance to aqueous outflow via altered trabecular meshwork extracellular matrix / endothelial cell function
- IOP rise is dose-, potency-, and duration-dependent; usually begins 2-4 weeks after starting
- After IVTA: IOP elevation lasts 2-4 months
- After dexamethasone implant (Ozurdex): up to 6 months
- Risk factors: existing glaucoma/OHT, family history of glaucoma, high myopia, young age, connective tissue disease (especially RA)
- Management: discontinue steroid (IOP normalizes within days-weeks); switch to less potent drop (fluorometholone, loteprednol); persistent elevation - medical or surgical management
- 3% of patients have persistent IOP elevation despite stopping steroids
- Kanski's Clinical Ophthalmology, p. 453
Posterior Subcapsular Cataract (PSC)
- Less common with topical than systemic steroids
- Risk increases with dose and duration
- A major reason intravitreal implants require careful long-term follow-up
Other Toxicities
- Secondary infections (bacterial, fungal; reactivation of HSV keratitis)
- Corneal melting (especially with periocular steroids in scleritis)
- Systemic absorption effects (rare with topical; more relevant in children)
5. Step-Up Treatment Algorithm for Uveitis
1st line: Topical prednisolone acetate 1% q1-2h ± cycloplegia
↓ (severe, unilateral, unresponsive)
2nd line: Periocular repository steroid (subtenon triamcinolone 40 mg/mL, 0.5-1.0 mL)
Repeat every 6-8 weeks x 3 if needed
↓ (bilateral, or no response after 3 injections)
3rd line: Systemic steroids (prednisone 40-60 mg/day, taper over weeks)
OR intravitreal sustained-release implant (Ozurdex 0.7 mg; fluocinolone 0.19 mg)
↓ (refractory / steroid-sparing needed)
4th line: Immunomodulatory therapy (methotrexate, mycophenolate, anti-TNF agents)
+ Rheumatology referral
In children and adolescents, systemic steroids may be preferred over bilateral periocular injections to avoid growth suppression, but long-term systemic use carries its own significant risk. Bilateral disease generally favors systemic therapy. - Wills Eye Manual, p. 943
6. Key Drug Comparisons
| Property | Fluorometholone | Loteprednol | Prednisolone | Dexamethasone |
|---|---|---|---|---|
| Anti-inflammatory potency | Moderate | Moderate | High | High |
| IOP-raising potential | Low | Low | High | High |
| Corneal penetration | Good | Good | Excellent | Excellent |
| Best use | Mild inflammation, long-term | Mild-moderate, "safe" steroid | Acute uveitis, post-op | Uveitis, implants |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 453-455
- The Wills Eye Manual, 8th ed., pp. 826, 935, 942-943
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, p. 976
This is a shared conversation. Sign in to Orris to start your own chat.