Tell me about cranial nerves from every resources you have in details
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, multi-source account of the cranial nerves, synthesized from Gray's Anatomy for Students, Neuroscience: Exploring the Brain (5e), Neuroanatomy through Clinical Cases (3e), Kandel's Principles of Neural Science (6e), Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, and Localization in Clinical Neurology (8e).
The Cranial Nerves - Complete Reference
Overview
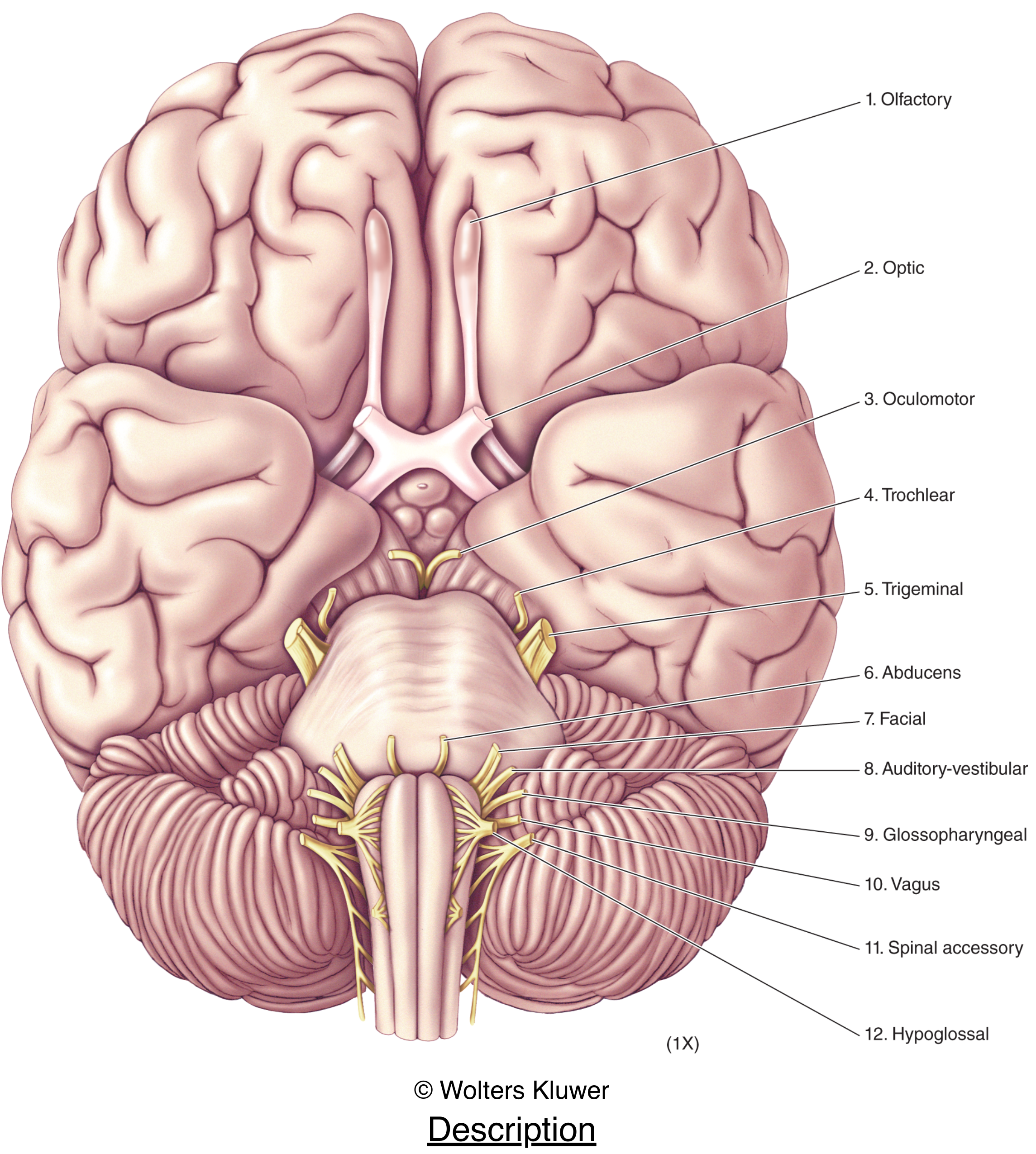
There are 12 pairs of cranial nerves (CN I - XII). Their defining feature is that they exit the cranial cavity through foramina or fissures in the skull. The first two (olfactory and optic) are technically extensions of the central nervous system, not peripheral nerves in the true sense - the rest are analogous to spinal nerves but often carry multiple functional components simultaneously. All innervate structures in the head or neck; the vagus nerve is the exception, descending into the thorax and abdomen.
From the base of the brain (inferior view):
Functional Components (Gray's Anatomy for Students, Table 8.4)
Cranial nerves carry one or more of these functional fibre types:
| Abbreviation | Full Name | Function | Cranial Nerves |
|---|---|---|---|
| GSA | General Somatic Afferent | Touch, pain, temperature | V, VII, IX, X |
| GVA | General Visceral Afferent | Sensory from viscera | IX, X |
| SA | Special Afferent | Smell, taste, vision, hearing, balance | I, II, VII, VIII, IX, X |
| GSE | General Somatic Efferent | Motor to skeletal (voluntary) muscles | III, IV, VI, XII |
| GVE | General Visceral Efferent | Motor to smooth muscle, heart, glands (parasympathetic) | III, VII, IX, X |
| BE | Branchial Efferent | Motor to pharyngeal arch-derived muscles | V, VII, IX, X, XI |
Cranial Nerve Nuclei Organization (Kandel's Principles of Neural Science, 6e)
Cranial nerve nuclei reside in the midbrain, pons, and medulla, arranged in rostrocaudal columns. The organization mirrors the spinal cord: the alar plate (dorsal) gives rise to sensory nuclei, and the basal plate (ventral) gives rise to motor nuclei. As the spinal canal opens into the fourth ventricle, dorsal sensory structures are displaced laterally and ventral motor structures remain medial. Nuclei are classed as:
- General nuclei - functions similar to the spinal cord
- Special nuclei - unique to the head (hearing, balance, taste, jaw/face/laryngeal motor control)
The Skull Exit Points (Kandel's Principles of Neural Science, 6e)
Cranial nerves exit in anatomical groups, making them vulnerable to grouped injury from tumors or fractures:
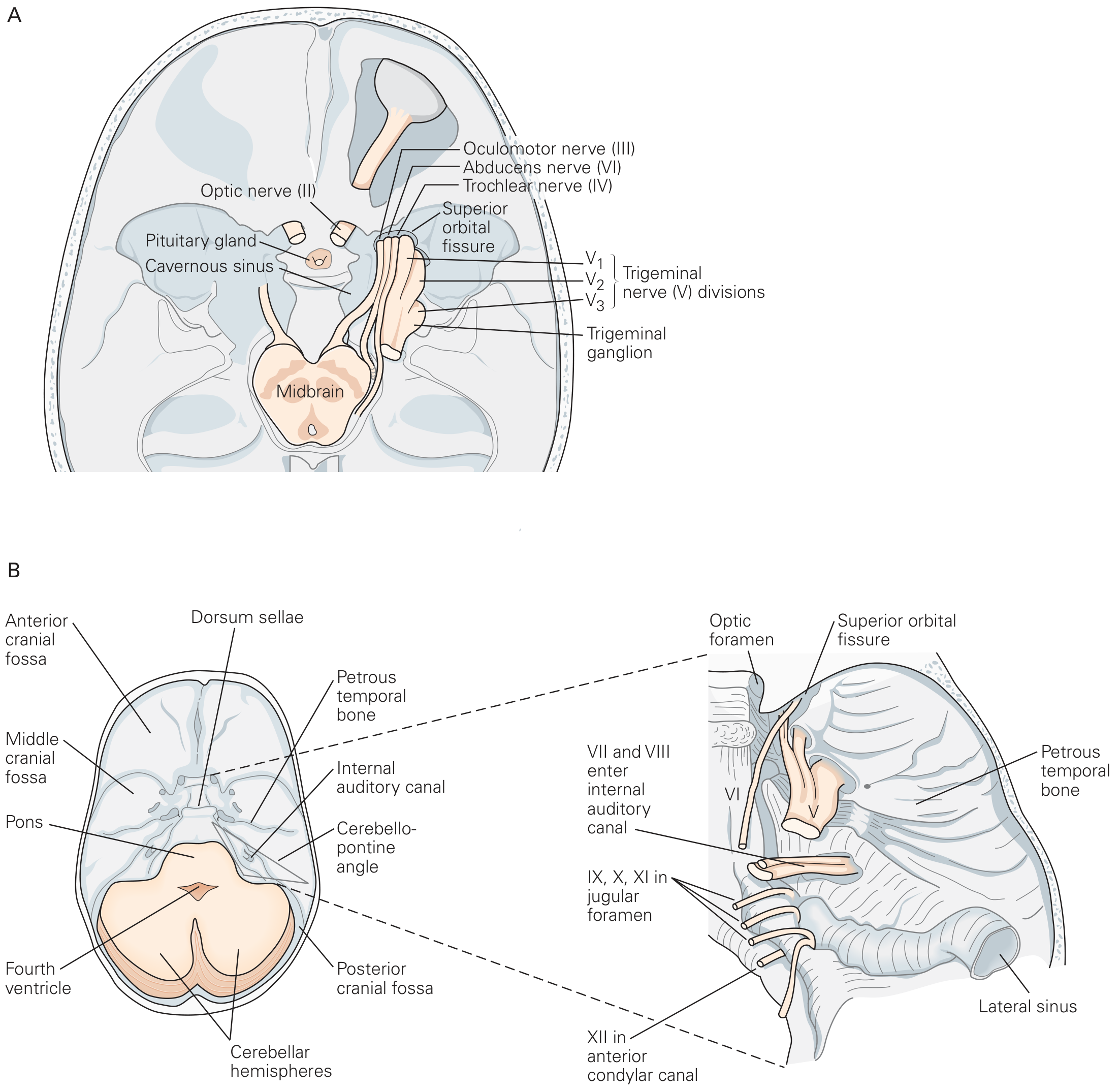
| Foramen/Opening | Cranial Nerves |
|---|---|
| Cribriform plate of ethmoid | CN I |
| Optic canal | CN II |
| Superior orbital fissure | CN III, IV, VI, V1 |
| Foramen rotundum | V2 (maxillary) |
| Foramen ovale | V3 (mandibular) |
| Internal acoustic meatus | CN VII, VIII |
| Jugular foramen | CN IX, X, XI |
| Hypoglossal canal | CN XII |
Each Cranial Nerve - Detailed
CN I - Olfactory Nerve
- Type: Special afferent (SA) - pure sensory
- Origin: Olfactory receptor neurons in nasal mucosa; axons pass through the cribriform plate to the olfactory bulb
- Function: Sense of smell (olfaction)
- Clinical testing (Neuroanatomy through Clinical Cases, 3e): Ask the patient to smell ground coffee or citrus with each nostril separately. Do NOT use noxious odors - they activate CN V pain fibers, not CN I.
- Clinical significance: CN I is one of the most commonly damaged nerves after mild traumatic brain injury (MTBI) - loss of smell (anosmia/hyposmia) results. It is also an early marker of neurodegeneration in Alzheimer's and Parkinson's disease. Subfrontal brain tumors (e.g., olfactory groove meningioma) may silently compress the olfactory bulbs.
CN II - Optic Nerve
- Type: Special afferent (SA) - pure sensory; technically a CNS tract, not a true PNS nerve
- Origin: Retinal ganglion cells; exits the orbit via the optic canal and forms the optic chiasm
- Function: Vision
- Clinical testing:
- Visual acuity (Snellen chart, each eye separately)
- Color vision - red desaturation is a sensitive early sign of optic nerve dysfunction (as in optic neuritis)
- Visual fields (confrontation testing in all four quadrants)
- Ophthalmoscopy - direct visualization of retinal vessels, optic disc, papilledema
- Pupillary light reflex (afferent limb = CN II; efferent = CN III)
- Lesion patterns: Unilateral CN II damage causes monocular visual loss; chiasmal lesions cause bitemporal hemianopia; optic tract lesions cause contralateral homonymous hemianopia.
CN III - Oculomotor Nerve
- Type: General somatic efferent (GSE) + General visceral efferent (GVE / parasympathetic)
- Origin: Midbrain (oculomotor nucleus for GSE; Edinger-Westphal nucleus for GVE); exits via the superior orbital fissure
- GSE function: Innervates levator palpebrae superioris, superior rectus, inferior rectus, medial rectus, inferior oblique
- GVE function: Parasympathetic via ciliary ganglion to sphincter pupillae (pupillary constriction) and ciliary muscle (lens accommodation)
- CN III palsy: "Down and out" eye position (lateral rectus and superior oblique unopposed), ptosis, and a fixed dilated pupil (mydriasis - parasympathetic fibers travel on the outside of CN III and are compressed first by aneurysms). A posterior communicating artery aneurysm classically presents with a painful third nerve palsy with pupil involvement.
CN IV - Trochlear Nerve
- Type: GSE - pure motor
- Origin: Midbrain; the only cranial nerve to exit the dorsal surface of the brainstem; exits skull via superior orbital fissure
- Function: Innervates the superior oblique muscle, which depresses and intorts the eye
- Clinical note (Rosen's EM): CN IV palsy causes vertical diplopia worsened when looking down and inward - patients complain of difficulty reading or descending stairs. CN IV is more commonly injured than CN III in mild TBI.
CN V - Trigeminal Nerve
- Type: GSA (large sensory component) + BE (branchial efferent/motor)
- Origin: Pons (main sensory nucleus and motor nucleus); largest cranial nerve
- Three divisions:
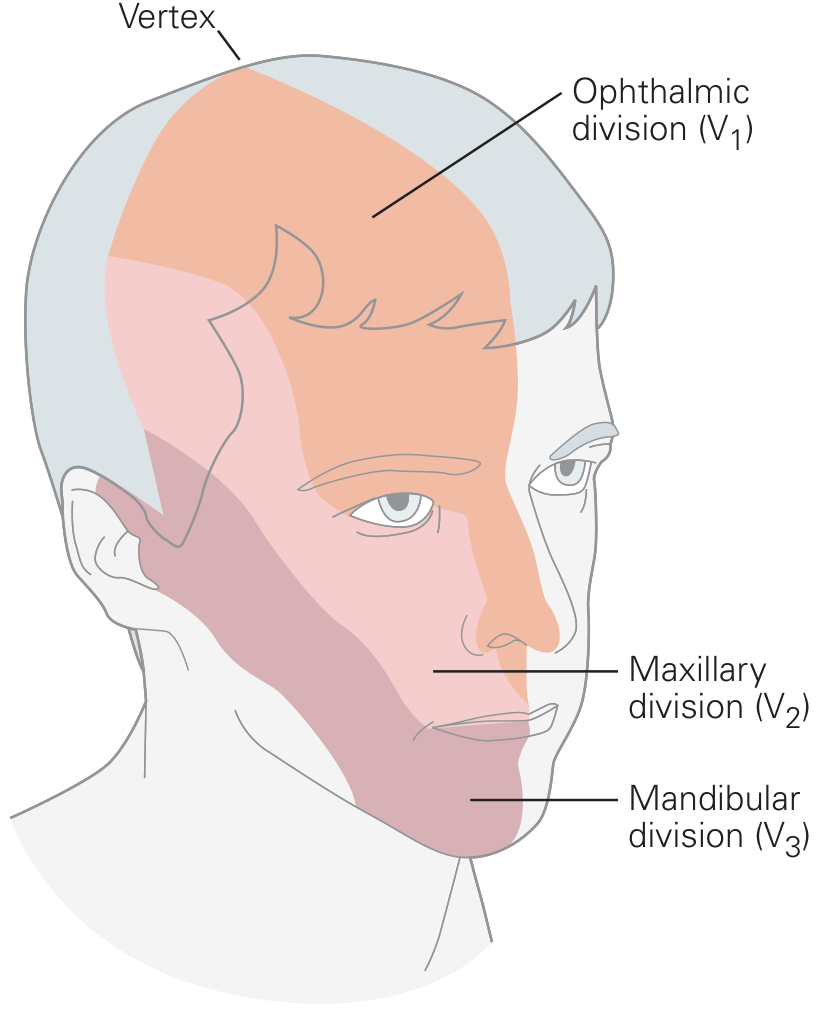
| Division | Exit | Sensory Territory |
|---|---|---|
| V1 (Ophthalmic) | Superior orbital fissure | Eyes, conjunctiva, orbital contents, nasal cavity, frontal sinus, upper eyelid, dorsum of nose, anterior scalp, dura of anterior cranial fossa |
| V2 (Maxillary) | Foramen rotundum | Nasopharynx, palate, nasal cavity, upper teeth, maxillary sinus, lower eyelid, cheek, upper lip |
| V3 (Mandibular) | Foramen ovale | Lower face, cheek, lower lip, anterior ear, external acoustic meatus, anterior two-thirds of tongue (GSA only, not taste), lower teeth, mastoid air cells |
- Motor (BE): V3 innervates temporalis, masseter, medial and lateral pterygoids, tensor tympani, tensor veli palatini, anterior belly of digastric, mylohyoid (muscles of mastication and more)
- Trigeminal neuralgia: Brief, lancinating, shock-like facial pain triggered by nonpainful stimuli (eating, talking, touch). First-line treatment is carbamazepine (200-400 mg/day up to 1200 mg/day) or oxcarbazepine (300-600 mg/day up to 1800 mg/day) per Rosen's EM. Neurological deficits on exam should prompt MRI to exclude a structural lesion.
CN VI - Abducens Nerve
- Type: GSE - pure motor
- Origin: Pons (abducens nucleus); exits via superior orbital fissure
- Function: Innervates the lateral rectus muscle (eye abduction)
- Clinical note: CN VI has the longest intracranial course - it is vulnerable to raised intracranial pressure (false localizing sign). Palsy causes medial deviation of the eye and horizontal diplopia on gaze toward the affected side.
CN VII - Facial Nerve
- Type: GSA + SA (special afferent/taste) + GVE (parasympathetic) + BE (branchial efferent/motor)
- Origin: Pons; exits the cranial cavity through the internal acoustic meatus, gives branches within the facial canal of the temporal bone, then exits the skull via the stylomastoid foramen
- Functions:
- BE (motor): Muscles of facial expression, scalp, stapedius, posterior belly of digastric, stylohyoid (all from second pharyngeal arch)
- GVE (parasympathetic): Via pterygopalatine ganglion to lacrimal gland, nasal/palatal mucous glands; via submandibular ganglion to submandibular and sublingual salivary glands
- SA (taste): Anterior two-thirds of tongue via chorda tympani
- GSA: Part of external acoustic meatus and deeper parts of the auricle
Parasympathetic pathways from CN VII:
- Bell's palsy (CN VII palsy, Kandel's 6e): Ipsilateral facial weakness affecting ALL facial muscles (distinguishing it from an UMN stroke which spares the forehead). May also cause:
- Hyperacusis (stapedius paralysis - sounds boom in the affected ear)
- Loss of taste on anterior 2/3 of tongue
- Reduced lacrimation
- If caused by herpes zoster of the geniculate ganglion: blisters in the outer ear canal (Ramsay Hunt syndrome)
- Temporal bone fracture: CN VII palsy + hearing loss = likely temporal bone fracture (Rosen's EM)
CN VIII - Vestibulocochlear Nerve (Auditory-Vestibular Nerve)
- Type: Special afferent (SA) - pure sensory; two functional divisions
- Origin: Enters cranial cavity via internal acoustic meatus; fibers from cochlear ganglion (hearing) and vestibular ganglion (balance)
- Cochlear division: Relays sound information from the cochlea
- Vestibular division: Relays angular and linear acceleration from the semicircular canals, utricle, and saccule; connects to CN III, IV, VI via the medial longitudinal fasciculus (MLF) for coordinated eye movements
- Vestibular schwannoma (acoustic neuroma - Kandel's 6e): Most common intracranial tumor of the posterior fossa, grows along the vestibular component of CN VIII in the internal auditory meatus. Usually presents first with hearing loss; the brain adapts to gradual vestibular loss from one side.
CN IX - Glossopharyngeal Nerve
- Type: GVA + SA + GSA + GVE + BE - a mixed nerve
- Exit: Jugular foramen
- Functions:
- GVA: Carotid body (chemoreceptors) and carotid sinus (baroreceptors) - important in cardiovascular reflexes; also posterior one-third of tongue, tonsils, oropharynx, middle ear mucosa, pharyngotympanic tube, mastoid air cells
- SA (taste): Posterior one-third of tongue
- GVE (parasympathetic): Via otic ganglion to parotid salivary gland
- BE (motor): Stylopharyngeus muscle
- Clinical (Rosen's EM): Isolated CN IX pathology is rare. Glossopharyngeal neuralgia presents as painful paroxysms beginning in the throat, radiating down the side of the neck in front of the ear but behind the mandible.
- Jugular foramen syndrome (Vernet syndrome - Localization in Clinical Neurology): Combined IX, X, XI palsy from a lesion at the jugular foramen (e.g., glomus jugulare tumor, basal skull fracture).
CN X - Vagus Nerve
- Type: GSA + GVA + SA + GVE + BE - the most widely distributed cranial nerve
- Exit: Jugular foramen; descends through the neck into the thorax and abdomen
- Functions:
- GVE (parasympathetic): Heart, lungs, and abdominal viscera up to the foregut/midgut junction (splenic flexure of colon)
- GVA: Aortic chemoreceptors and baroreceptors; esophagus, bronchi, lungs, heart, and foregut/midgut viscera
- GSA: Larynx, laryngopharynx, part of the auricle and external acoustic meatus, dura of posterior cranial fossa
- SA (taste): Epiglottis and pharynx
- BE (motor): Palatoglossus (one tongue muscle), muscles of the soft palate (except tensor veli palatini), pharynx (except stylopharyngeus), and larynx
- Clinical (Rosen's EM):
- Unilateral palatal weakness: fluid regurgitates nasally on drinking
- Unilateral vocal cord palsy: hoarse voice
- Recurrent laryngeal nerve injury (e.g., during thyroid or thoracic surgery) is a common cause of CN X motor deficit
CN XI - Spinal Accessory Nerve
- Type: BE (branchial efferent) - purely motor
- Origin: Unique among cranial nerves - arises from the cervical spinal cord (C1-C5 levels), ascends through the foramen magnum into the skull, then exits via the jugular foramen
- Function: Motor to sternocleidomastoid (turns head to opposite side) and trapezius (elevates and retracts shoulder/scapula)
- Clinical (Rosen's EM): Lesion causes downward/lateral rotation of the scapula and shoulder drop. CN XI is classified as "branchial efferent" because its target muscles are derived from pharyngeal arch mesoderm (Diogo R et al. Nature 2015).
CN XII - Hypoglossal Nerve
- Type: GSE - pure motor
- Origin: Medulla; exits via the hypoglossal canal
- Function: Innervates hyoglossus, genioglossus, styloglossus, and ALL intrinsic muscles of the tongue
- Clinical (Rosen's EM):
- LMN lesion (e.g., skull base metastasis, ALS): Tongue deviates toward the side of the lesion on protrusion; ipsilateral atrophy and fasciculations develop over time
- UMN lesion (e.g., stroke): Tongue deviates away from the side of the lesion (toward the weak side)
- Bilateral LMN lesion (as in ALS): Severe dysarthria and dysphagia, tongue atrophy and fasciculations bilaterally
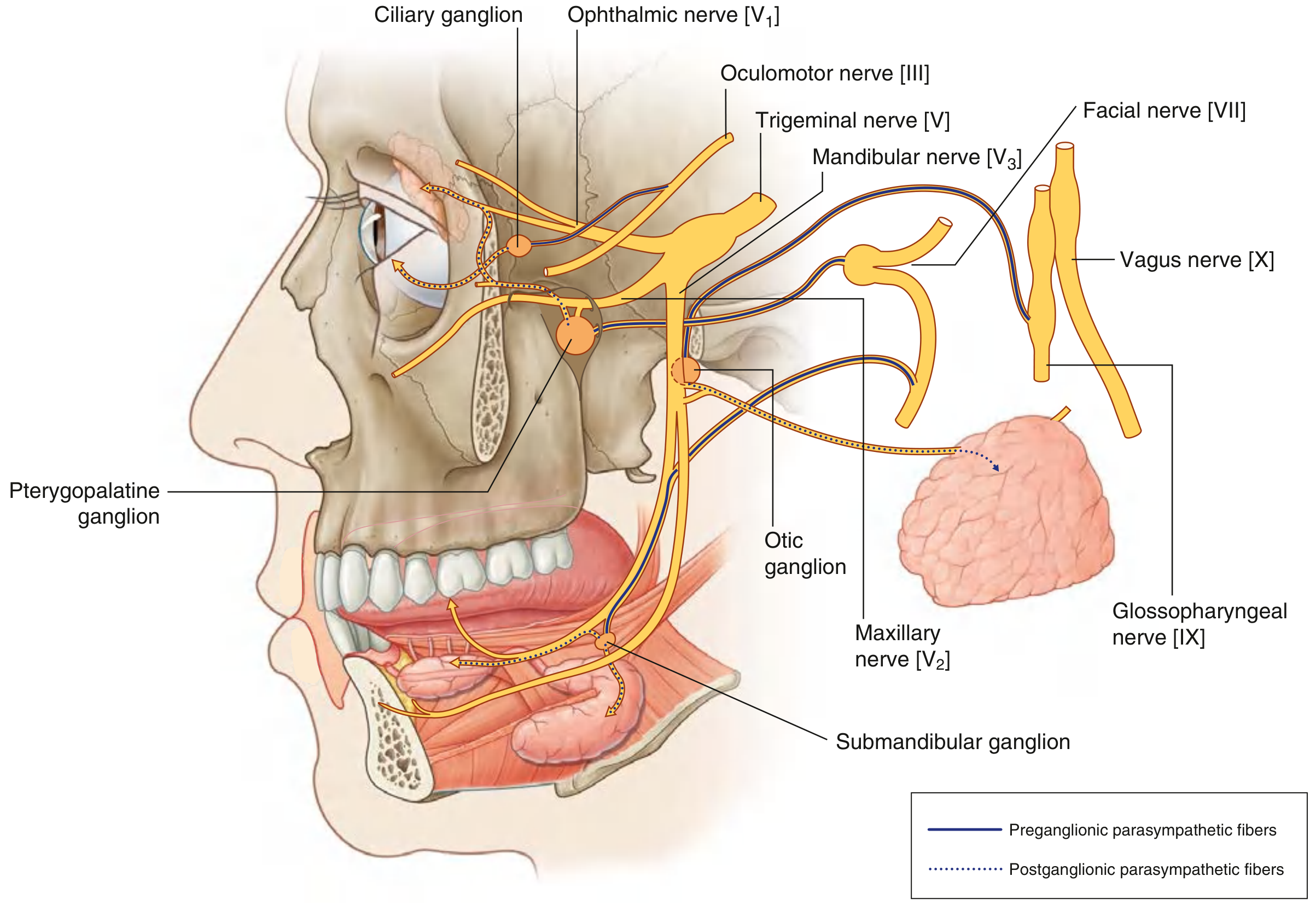
Parasympathetic Summary (Gray's Anatomy for Students)
The four cranial nerves carrying parasympathetic fibers and their ganglia:
| CN | Ganglion | Target |
|---|---|---|
| III (Oculomotor) | Ciliary ganglion | Pupillary constriction, lens accommodation |
| VII (Facial) | Pterygopalatine ganglion | Lacrimal gland, nasal/palatal glands |
| VII (Facial) | Submandibular ganglion | Submandibular and sublingual salivary glands |
| IX (Glossopharyngeal) | Otic ganglion | Parotid salivary gland |
| X (Vagus) | Terminal ganglia in organ walls | Heart, lungs, foregut/midgut viscera |
Parasympathetic fibers from CN III, VII, and IX travel to their targets by hitchhiking on branches of the trigeminal nerve (CN V).
Cranial Nerve Exam (Neuroanatomy through Clinical Cases, 3e)
Cranial nerve testing is critical because abnormalities together with symptoms like headache, dizziness, or unsteadiness strongly suggest brainstem dysfunction rather than a systemic cause.
| # | Exam | Nerves Tested |
|---|---|---|
| 1 | Olfaction (smell coffee/citrus) | CN I |
| 2 | Ophthalmoscopy | CN II |
| 3 | Visual acuity, fields, color vision | CN II |
| 4 | Pupillary responses | CN II (afferent), CN III (efferent) |
| 5 | Extraocular movements | CN III, IV, VI |
| 6 | Facial sensation, mastication muscles | CN V |
| 7 | Facial expression, taste | CN VII |
| 8 | Hearing, vestibular testing | CN VIII |
| 9 | Palate elevation, gag reflex | CN IX, X |
| 10 | Articulation | CN V, VII, IX, X, XII |
| 11 | SCM and trapezius strength | CN XI |
| 12 | Tongue movements and symmetry | CN XII |
In coma, the cranial nerve exam is adapted: blink-to-threat (CN II), pupillary responses (II/III), spontaneous eye movements + vestibulo-ocular reflex/oculocephalic maneuver/caloric testing (III, IV, VI, VIII), corneal reflex (V/VII), and gag reflex (IX/X).
Clinically Important Syndromes
Jugular Foramen Syndromes (Localization in Clinical Neurology, 8e)
| Syndrome | Nerves | Site |
|---|---|---|
| Vernet | IX, X, XI | Jugular foramen |
| Collet-Sicard | IX, X, XI, XII | Retroparotid space (intra- or extracranial) |
| Villaret | IX, X, XI, XII + sympathetic chain (+/- VII) | Retroparotid/retropharyngeal space |
Collet-Sicard findings (all ipsilateral):
- Paralysis of trapezius and SCM (XI)
- Vocal cord and pharyngeal paralysis (X/IX)
- Hemiparalysis of the tongue (XII)
- Loss of taste on posterior third of tongue (IX)
- Hemianesthesia of palate, pharynx, and larynx (IX/X)
Cranial Nerves and Trauma (Rosen's Emergency Medicine)
After MTBI with skull base fractures:
- CN I - most commonly injured; anosmia is often missed
- CN VII + VIII - temporal bone fracture
- CN IV, VI - more common than CN III in blunt head injury
- CN IX, X - occipital condyle fractures
- CN V - facial pain/occipital neuralgia
Cavernous Sinus Syndrome
CN III, IV, V1/V2, and VI all run through or adjacent to the cavernous sinus. A lesion here (thrombosis, aneurysm, tumor) can produce combined ophthalmoplegia, ptosis, and facial sensory loss in the V1/V2 distribution.
Quick Memory Mnemonics
Names: Oh Oh Oh, To Touch And Feel Very Good Velvet, Ahh Heaven
(Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal)
Sensory/Motor/Both:
Some Say Marry Money, But My Brother Says Big Brains Matter More
(S, S, M, M, B, M, B, S, B, B, M, M)
Sources consulted:
- Gray's Anatomy for Students (Tables 8.4 and 8.5)
- Neuroscience: Exploring the Brain, 5e (Chapter on Cranial Nerves)
- Neuroanatomy through Clinical Cases, 3e (Chapter 2)
- Kandel's Principles of Neural Science, 6e (Chapter 40)
- Rosen's Emergency Medicine (CN injury in MTBI; CN function table)
- Tintinalli's Emergency Medicine (CN examination)
- Localization in Clinical Neurology, 8e (Jugular foramen syndromes, Collet-Sicard, Villaret)
This is a shared conversation. Sign in to Orris to start your own chat.