Hypoglycemia
Reading File
Finding Sources
Searching PubMed
hypoglycemia management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive response.
Hypoglycemia
Definition
Hypoglycemia is defined as a plasma glucose level low enough to cause symptoms or signs of neurological dysfunction. In clinical practice, a blood glucose below 70 mg/dL (3.9 mmol/L) is the alert threshold, with severe neuroglycopenic dysfunction typically occurring below 50 mg/dL (2.8 mmol/L). In diabetic patients, it is always iatrogenic or due to accidental/intentional overdose.
Pathophysiology
Normally, a falling blood glucose triggers two protective responses:
- Cessation of endogenous insulin secretion
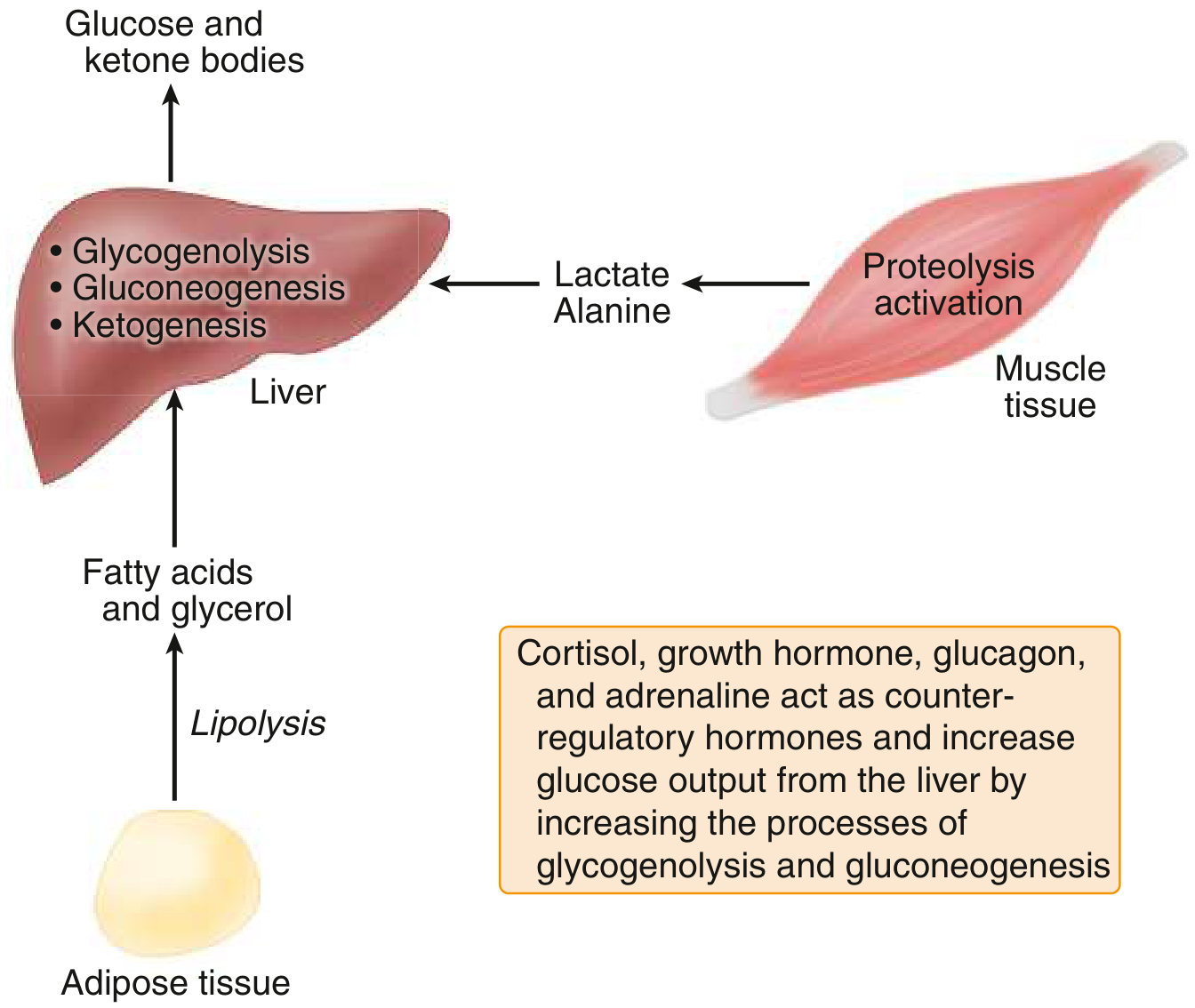
- Release of counter-regulatory hormones: glucagon, epinephrine (adrenaline), cortisol, and growth hormone
These hormones stimulate hepatic glycogenolysis and gluconeogenesis, lipolysis in adipose tissue, and proteolysis in muscle (providing lactate and alanine as gluconeogenic substrates).
In patients with type 1 diabetes, glucagon release during hypoglycemia becomes impaired shortly after onset of disease. Epinephrine secretion also becomes progressively defective with longer diabetes duration. This defect in counter-regulation, compounded by hypoglycemia unawareness (from prior episodes resetting the glycemic threshold), makes recurrent severe hypoglycemia a major hazard.
- Goldman-Cecil Medicine, Ch. 211
Causes
Diabetic / Iatrogenic (most common)
- Insulin excess relative to carbohydrate intake
- Sulfonylureas (particularly dangerous - prolonged, severe, and recurrent)
- Missed meals, increased exercise, weight loss, alcohol intake
- Renal failure (reduced insulin clearance), liver disease
Non-Diabetic: Fasting Hypoglycemia
| Category | Examples |
|---|---|
| Excess insulin/IGF | Insulinoma, congenital hyperinsulinism, exogenous insulin factitious disorder |
| Hormone deficiency | Cortisol deficiency (Addison's), growth hormone deficiency, glucagon deficiency |
| Hepatic disease | Severe liver failure, glycogen storage diseases, fatty acid oxidation defects |
| Drugs | Alcohol, quinolones, pentamidine, quinine, salicylates |
| Tumors (non-islet) | Large retroperitoneal sarcomas/hepatocellular carcinoma secreting IGF-II |
| Critical illness | Sepsis, multiorgan failure |
| Inherited metabolic disorders | Galactosemia, fructosemia, MCAD deficiency, maple syrup urine disease |
Non-Diabetic: Postprandial (Reactive) Hypoglycemia
-
Most commonly due to alimentary hyperinsulinism after gastric surgery (gastrectomy, gastrojejunostomy, pyloroplasty, vagotomy)
-
ROSEN's Emergency Medicine, Ch. 115 | Goldman-Cecil Medicine, Ch. 211
Clinical Features
Symptoms arise from two mechanisms:
1. Neurogenic (Autonomic) Symptoms - occur ~60 mg/dL
- Adrenergic: palpitations, tremor, anxiety
- Cholinergic: sweating, hunger, paresthesias
2. Neuroglycopenic Symptoms - occur ~50 mg/dL
- Dizziness, confusion, difficulty speaking, headache, inability to concentrate
- Bizarre behavior, focal neurologic deficits
- Seizures, coma
Hypoglycemia Unawareness: Patients with recurrent hypoglycemia have their glycemic thresholds reset lower, so the warning neurogenic symptoms are blunted or absent. They may rapidly become unarousable without the usual adrenergic prodrome.
Somogyi Phenomenon: Excessive insulin dosing causes a nocturnal (early morning) hypoglycemic episode. The counter-regulatory rebound produces fasting hyperglycemia, which is mistakenly interpreted as a need to increase the insulin dose - worsening the cycle.
- Goldman-Cecil Medicine, Ch. 211
Whipple's Triad (Diagnostic Criteria)
- Symptoms consistent with hypoglycemia
- Low plasma glucose measured at time of symptoms
- Relief of symptoms with correction of blood glucose
Diagnostic Workup
| Test | Significance |
|---|---|
| Blood glucose (fluoride tube, immediate analysis) | Confirmation; whole-blood is ~15% lower than serum |
| Insulin level | Elevated insulin with low glucose = insulinoma or exogenous insulin |
| C-peptide | Low C-peptide with high insulin = exogenous insulin (factitious); elevated = endogenous |
| Cortisol, growth hormone | Exclude hormone deficiencies |
| Lactate, 3-β-hydroxybutyrate, NEFA | Metabolic profiling |
| Acylcarnitine profile (blood spot) | Fatty acid oxidation disorders |
| Urine ketones, organic acids | Inherited metabolic disease |
| Sulfonylurea screen | Suspected secretagogue ingestion |
A 72-hour supervised fast followed by measurement of glucose, insulin, C-peptide, and proinsulin remains the gold standard for diagnosing insulinoma.
- Goldman-Cecil Medicine, Ch. 211
Management
Mild-Moderate (Patient Alert, Able to Swallow)
- Oral glucose: sugar-containing food or drink, fast-acting carbohydrates (15-20 g)
Moderate-Severe (Impaired Consciousness, IV Access Available)
- D50W (50% dextrose): 1-3 ampules IV; glucose rise can be <40 to >350 mg/dL per ampule
- In suspected alcohol use disorder: give thiamine first (or simultaneously) to prevent precipitating Wernicke encephalopathy
- Children <8 years: use D25W (dilute D50W 1:1 with sterile water) at 0.5-1 g/kg (2-4 mL/kg), or D10W; avoid hyperosmolar injury
No IV Access
- Glucagon 1-2 mg IM or SC (onset 10-20 min, peak 30-60 min); may repeat. Intranasal glucagon is an alternative.
- Families of type 1 diabetic patients should be trained to administer glucagon at home.
Sulfonylurea-Induced Hypoglycemia (Special Case)
- Tends to be prolonged and severe
- Add octreotide (somatostatin analogue) to suppress further insulin release: 50-100 mcg IV/SC q12h in adults; 0.1 mcg/kg in children
- Observe for at least 24 hours in hospital due to delayed recurrence (up to 18 hours post-ingestion in some cases)
- A single tablet can cause severe hypoglycemia in renal failure patients, children, or sulfonylurea-naive patients
Disposition
-
Type 1 DM with brief, uncomplicated episode: may discharge after identifying and correcting the cause, giving a meal, and arranging short-term follow-up
-
Sulfonylurea-induced with recurrent hypoglycemia in ED: admit
-
Non-diabetic hypoglycemia: inpatient workup usually warranted
-
ROSEN's Emergency Medicine, Ch. 115 | Goldman-Cecil Medicine, Ch. 210-211
Risk Factors Summary
| Medical | Lifestyle |
|---|---|
| Strict glycemic control | Missed or delayed meals |
| Prior severe hypoglycemia | Intense exercise |
| Long duration of type 1 DM | Alcohol use |
| Insulin use in type 2 DM | |
| Impaired hypoglycemia awareness | |
| Renal or hepatic disease | |
| Elderly age | |
| Lipohypertrophy at injection sites |
Special Populations
- Elderly: Reduced adrenergic symptoms, so neuroglycopenic impairment may dominate without warning signs; higher risk of cognitive sequelae
- Pregnancy: Intensive insulin therapy for euglycemia increases hypoglycemia risk; fetal effects are unclear but maternal DKA carries 50-90% fetal mortality
- Critical illness: Common in ICU; associated with sepsis and multiorgan failure
- Children: More common; hypoglycemia from a single sulfonylurea tablet is well documented; use weight-based dilute dextrose solutions
Recent Evidence Note
A 2025 systematic review in Diabetes Care (PMID 40117466) assessed inpatient hyperglycemia/hypoglycemia management guidelines and found significant variation across institutions - no major paradigm shift in the core hypoglycemia treatment algorithm, but reinforcing individualized glucose targets, especially in the inpatient setting.
This is a shared conversation. Sign in to Orris to start your own chat.