MRI physics in depth
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full in-depth answer.
MRI Physics - In Depth
1. The Fundamental Phenomenon: Nuclear Magnetic Resonance (NMR)
MRI is built on the physics of nuclear magnetic resonance, first described in the 1940s. The key insight: certain atomic nuclei with an odd number of protons and/or neutrons possess a net nuclear spin and therefore a magnetic moment - they behave like tiny bar magnets.
Why hydrogen? Although many nuclei (¹³C, ³¹P, ²³Na) exhibit NMR, clinical MRI almost exclusively uses the protium nucleus (¹H) because:
- It is the most naturally abundant nucleus in the human body (present in water and fat)
- It has the highest gyromagnetic ratio among common nuclei, giving the strongest signal
- Water represents ~60-70% of body weight
- Rheumatology, 2-Volume Set (Elsevier, 2022), BASIC PRINCIPLES
2. The Static Magnetic Field (B₀)
When a patient enters the MRI bore, they are placed in a powerful static magnetic field B₀, typically 1.5 Tesla (T) or 3 T in clinical practice (15,000-30,000 times Earth's field). Research scanners reach 7 T and beyond.
What happens to protons in B₀?
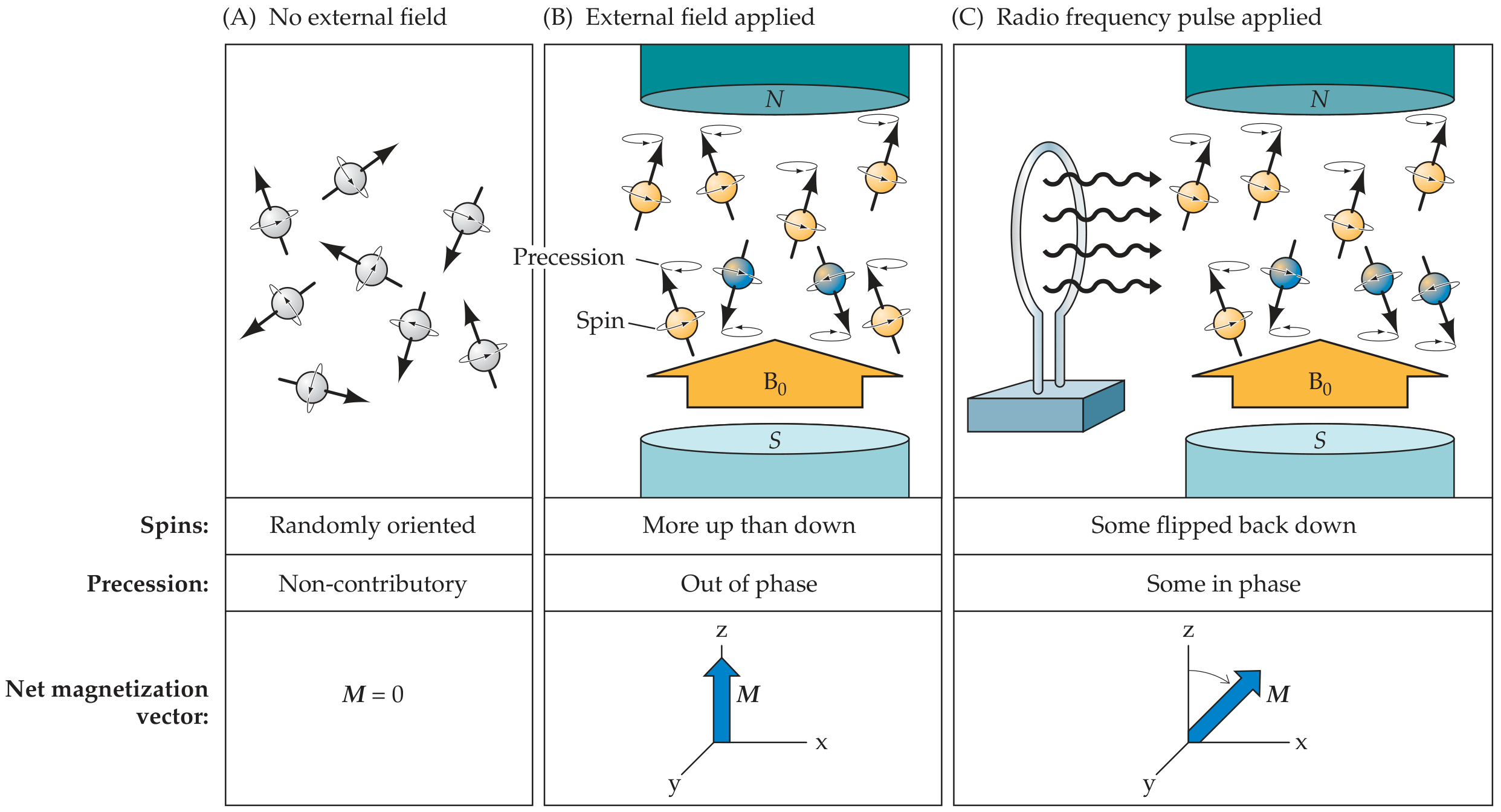
In the absence of any external field, proton magnetic moments point in random directions - the net magnetization vector M = 0.
Once B₀ is applied, quantum mechanics dictates that proton spins can adopt only two states:
- Parallel (low energy, "spin up") - aligned with B₀
- Antiparallel (high energy, "spin down") - opposed to B₀
A slightly greater number align parallel than antiparallel (the population difference is governed by the Boltzmann distribution and is only ~1 in 10⁶ at 1.5 T - MRI is inherently signal-limited). This tiny excess creates a small net magnetization vector M oriented along the z-axis (the bore axis).
- Neuroanatomy through Clinical Cases 3rd Edition, Fig. 4.5
3. Precession and the Larmor Equation
Protons in B₀ do not simply sit still - they precess (wobble) around the z-axis, like a spinning top in a gravitational field. The angular frequency of this precession is given by:
The Larmor Equation:
ω₀ = γ · B₀
Where:
- ω₀ = Larmor (resonant) frequency
- γ = gyromagnetic ratio (a constant specific to each nucleus; for ¹H, γ = 42.58 MHz/T)
- B₀ = field strength in Tesla
At 1.5 T: ω₀ = 42.58 × 1.5 = ~63.87 MHz (radio frequency range)
At 3.0 T: ω₀ = ~127.7 MHz
This is critical: the RF pulse must be delivered at exactly this frequency for resonance to occur.
- Rheumatology, 2-Volume Set (Elsevier 2022), BASIC PRINCIPLES
4. The Radiofrequency (RF) Pulse and Excitation
An external radiofrequency (RF) coil transmits an electromagnetic pulse at the Larmor frequency (B₁ pulse). This accomplishes two things simultaneously:
- Energy absorption - some protons flip from the parallel (low energy) to antiparallel (high energy) state, reducing the z-component of M
- Phase coherence - the precessions of individual protons come into phase with each other, creating a component of magnetization in the transverse (x-y) plane
The angle through which M is tilted away from the z-axis is called the flip angle (α):
- A 90° pulse tips M entirely into the x-y plane
- A 180° pulse inverts M to the -z direction (used in inversion recovery sequences)
After the RF pulse is switched off, the rotating transverse magnetization induces a current in a nearby receiver coil - this is the free induction decay (FID) signal. The MRI image is ultimately derived from this signal.
- Fuster and Hurst's The Heart, 15th Edition, Physical Principles
5. Relaxation: T1 and T2
After excitation, protons must return to equilibrium. This relaxation occurs via two independent and simultaneous processes:
5a. T1 Relaxation (Longitudinal / Spin-Lattice)
- The z-component of M recovers toward its equilibrium value M₀
- Energy is transferred from excited protons to the surrounding molecular lattice (hence "spin-lattice")
- The recovery follows an exponential curve: M_z(t) = M₀(1 - e^(-t/T1))
- T1 = time for the longitudinal magnetization to recover to 63% of its equilibrium value after a 90° pulse
- T1 depends on how efficiently the local molecular environment can absorb the precessional energy (molecular motion matching the Larmor frequency accelerates T1 recovery)
Typical T1 values at 1.5 T:
| Tissue | T1 (ms) |
|---|---|
| Fat | 200-250 |
| White matter | 600-800 |
| Gray matter | 800-1000 |
| Muscle | 870 |
| CSF | 2000-4000 |
Short T1 = fast recovery = bright on T1-weighted images (fat, gadolinium, methemoglobin)
- Rheumatology, 2-Volume Set (Elsevier 2022), T1 RELAXATION
5b. T2 Relaxation (Transverse / Spin-Spin)
- The x-y component of M decays toward zero
- Protons in the transverse plane begin to lose phase coherence - individual spins point in increasingly random directions, canceling each other out
- This happens due to spin-spin interactions (fluctuating local magnetic fields caused by neighboring nuclei)
- Follows an exponential decay: M_xy(t) = M₀ · e^(-t/T2)
- T2 = time for transverse magnetization to decay to 37% of its peak value (the exponential decay constant)
T2 is always ≤ T1. Importantly, T2 relaxation is faster in solid or semi-solid tissues (rapid spin-spin interactions) and slower in pure fluids (slow molecular tumbling, less spin-spin dephasing).
Typical T2 values at 1.5 T:
| Tissue | T2 (ms) |
|---|---|
| Fat | 60-80 |
| White matter | 70-90 |
| Gray matter | 90-100 |
| Muscle | 45-65 |
| CSF | 1500-2000 |
Long T2 = slow signal decay = bright on T2-weighted images (CSF, edema, most pathology)
- Neuroanatomy through Clinical Cases 3rd Edition; Rheumatology 2022
5c. T2* Relaxation
In practice, the T2 decay is accelerated by:
- Inhomogeneities in the main B₀ field (magnet imperfections)
- Local susceptibility differences between tissues
The observed transverse decay constant is called T2* (T2-star), and is always shorter than T2:
1/T2* = 1/T2 + 1/T2_inhomogeneity
T2* is what you actually measure in a gradient echo sequence (no refocusing pulse). A spin echo sequence uses a 180° refocusing pulse to cancel out field inhomogeneity effects, recovering "true" T2.
- Fuster and Hurst's The Heart, 15th Edition; Rheumatology 2022
6. Pulse Sequences and Image Weighting
The appearance of tissues on MRI is controlled by the operator via pulse sequence parameters:
| Parameter | Definition |
|---|---|
| TR (repetition time) | Time between successive RF excitation pulses |
| TE (echo time) | Time between RF excitation and signal measurement |
| TI (inversion time) | Used in inversion recovery sequences |
How TR and TE create image contrast:
| Image Type | TR | TE | What it emphasizes |
|---|---|---|---|
| T1-weighted | Short | Short | T1 differences (short-TR penalizes long-T1 tissues; CSF stays dark) |
| T2-weighted | Long | Long | T2 differences (long-TE allows short-T2 tissues to decay; CSF is bright) |
| Proton density | Long | Short | Proton density (long TR allows full T1 recovery; short TE minimizes T2 decay) |
- Rheumatology 2022, MAGNETIC RESONANCE IMAGING CONTRAST
Tissue appearances by sequence:
| Tissue | T1-weighted | T2-weighted | FLAIR |
|---|---|---|---|
| Gray matter | Gray | Light gray | Light gray |
| White matter | White | Dark gray | Gray |
| CSF / water | Dark | Bright | Dark (suppressed) |
| Fat | Bright | Bright | Bright |
| Air / cortical bone | Black | Black | Black |
| Acute edema / infarct | Gray | Bright | Bright |
| Gadolinium enhancement | Bright | - | - |
- Neuroanatomy through Clinical Cases 3rd Edition, Table 4.3
7. Common Pulse Sequences
Spin Echo (SE)
- Uses a 90° excitation pulse followed by a 180° refocusing pulse
- The 180° pulse reverses the dephasing from field inhomogeneities, generating an echo at time TE
- This recovers signal lost to B₀ inhomogeneity, measuring "true" T2
- Slower but robust
Fast Spin Echo (FSE / Turbo Spin Echo)
- Multiple 180° refocusing pulses per TR, collecting multiple echoes ("echo train")
- Much faster acquisition; fat appears brighter than in conventional SE
Gradient Echo (GRE)
- Uses a gradient reversal (not a 180° pulse) to generate the echo
- Sensitive to T2* (field inhomogeneities are not corrected)
- Useful for detecting blood products, calcification, flow
- Allows shorter TR → rapid imaging (used in cardiac MRI, dynamic contrast studies)
Inversion Recovery (IR)
- Starts with a 180° inversion pulse (TI), then a 90° excitation pulse
- By choosing TI = T1 × ln(2) for a tissue, that tissue's signal is nulled at the moment of readout
- STIR (Short TI IR): nulls fat signal (TI ~150 ms). Used for edema detection in MSK and spine
- FLAIR (Fluid Attenuated IR): nulls CSF signal (TI ~2000 ms). Reveals periventricular/cortical lesions otherwise obscured by bright CSF
Diffusion-Weighted Imaging (DWI)
- Strong gradient pulses applied to dephase and rephase moving protons
- Freely diffusing water protons are rephased normally; restricted diffusion (as in cytotoxic edema from ischemic stroke) gives bright signal on DWI
- Detectable within 30 minutes of ischemic stroke onset (far earlier than conventional T2/FLAIR changes, which appear only after several hours)
- DWI bright + ADC dark = true restricted diffusion (e.g., acute infarct, abscess, dense tumor)
- DWI bright + ADC bright = "T2 shine-through" (not true restriction)
- Neuroanatomy through Clinical Cases 3rd Edition
Susceptibility-Weighted Imaging (SWI)
- Exquisitely sensitive to paramagnetic and diamagnetic substances
- Detects hemosiderin deposits from microhemorrhages, venous blood, calcification, iron deposition
- Useful in traumatic brain injury, cavernous malformations, cerebral amyloid angiopathy
8. Spatial Encoding and K-space
The signal from the entire patient volume must be localized to generate an image. This is accomplished using magnetic gradient coils that impose small, controlled variations on B₀.
Three gradient types:
- Slice selection gradient (Gz): Applied during the RF pulse. Only protons in the thin slice where ω₀ matches the RF frequency are excited. Slice thickness is determined by gradient strength and RF bandwidth.
- Frequency encoding gradient (Gx): Applied during signal readout. Protons along x precess at slightly different frequencies, encoding x-position in the signal frequency.
- Phase encoding gradient (Gy): Applied briefly between excitation and readout. Protons along y temporarily precess faster or slower, encoding y-position as a phase shift.
K-space:
Raw MRI data is stored in a mathematical domain called k-space (spatial frequency domain). Each row of k-space corresponds to one phase-encoding step. The image is recovered by applying a 2D Fourier transform to k-space. The center of k-space contains low spatial frequency data (overall contrast/brightness); the periphery contains high spatial frequency data (edges and fine detail).
9. MRI Hardware
| Component | Function |
|---|---|
| Main magnet | Generates B₀; usually a superconducting solenoid cooled with liquid helium |
| Gradient coils | Three orthogonal coils creating Gx, Gy, Gz; their rapid switching produces the characteristic banging noise |
| RF transmit coil | Delivers the excitation pulse at Larmor frequency |
| RF receive coil | Detects the NMR signal; surface coils placed close to the anatomy of interest maximize SNR |
| Shim coils | Fine-tune B₀ homogeneity across the bore |
10. Signal-to-Noise Ratio (SNR) and Image Quality
SNR is the primary determinant of image quality and depends on:
- Field strength (B₀): SNR ∝ B₀^~1.7; doubling field strength roughly doubles SNR
- Voxel volume: larger voxels → more protons → more signal (but less spatial resolution)
- Number of signal averages (NSA/NEX): SNR ∝ √NEX (doubling NEX doubles scan time for only 41% SNR gain)
- Bandwidth: narrower receiver bandwidth → less noise → better SNR (but longer minimum TE)
- Coil design: phased-array surface coils dramatically outperform body coils for SNR
The three key image quality metrics are: contrast sensitivity, spatial resolution, and SNR - and there is always a trade-off between them.
- Rheumatology 2022, IMAGE QUALITY
11. MRI Contrast Agents
Gadolinium (Gd) is the standard IV MRI contrast agent. It is paramagnetic (7 unpaired electrons) and shortens T1 of nearby protons, producing T1 brightening in regions of:
- Increased vascularity (tumors, inflammation)
- Blood-brain barrier (BBB) breakdown (metastases, abscesses, active MS plaques)
Gadolinium is far less nephrotoxic than iodinated CT contrast, but can cause nephrogenic systemic fibrosis (NSF) in patients with severe renal failure.
USPIO (ultra-small superparamagnetic iron oxide) particles are T2/T2* contrast agents that produce signal loss (darkening).
12. Special Considerations and Artifacts
Contraindications:
- Cardiac pacemakers (most older models) and implantable defibrillators
- Certain cerebral aneurysm clips (ferromagnetic)
- Cochlear implants
- Ocular/orbital metallic fragments
- Some prosthetic heart valves
Common Artifacts:
| Artifact | Cause | Appearance |
|---|---|---|
| Motion | Patient movement or physiological motion | Blurring, ghosting |
| Chemical shift | Fat and water protons precess at slightly different frequencies | Dark band at fat-water interfaces |
| Susceptibility / metal | Local field distortion around metal | Signal void + distortion |
| Aliasing (wrap) | FOV smaller than anatomy | Anatomy from outside FOV overlaps image |
| Gibbs ringing | Truncation of k-space | Ringing at sharp boundaries |
| Magic angle | Tendons/ligaments at 55° to B₀ show T2 prolongation | False bright signal in tendon/ligament on short-TE sequences |
Hemorrhage signal by age (paramagnetic effects):
| Stage | Age | T1 | T2 | Dominant species |
|---|---|---|---|---|
| Hyperacute | <6h | Iso | Bright | OxyHb |
| Acute | 6-72h | Iso/dark | Dark | DeoxyHb |
| Early subacute | Days | Bright | Dark | MetHb (intracellular) |
| Late subacute | Weeks | Bright | Bright | MetHb (extracellular) |
| Chronic | Months-years | Dark rim | Dark rim | Hemosiderin |
13. Key Clinical Takeaways (CT vs. MRI)
| Situation | Preferred |
|---|---|
| Acute head trauma / fresh hemorrhage | CT |
| Subtle infarct, demyelination, posterior fossa | MRI |
| Old hemorrhage | MRI |
| Bony detail / fracture | CT |
| Soft tissue, marrow, cord | MRI |
| Pacemaker or mobile metallic fragments | CT |
| Acute ischemic stroke <6h | MRI (DWI) |
- Neuroanatomy through Clinical Cases 3rd Edition, Table 4.2
Sources:
- Neuroanatomy through Clinical Cases, 3rd Edition - Blumenfeld (Sinauer/OUP)
- Rheumatology, 2-Volume Set (2022, Elsevier) - Basic Principles & MRI contrast
- Fuster and Hurst's The Heart, 15th Edition - Physical Principles of CMR
- Miller's Review of Orthopaedics, 9th Edition - Tables 134-136
- Rheumatology/Firestein & Kelley's Textbook of Rheumatology - MSK MRI principles
This is a shared conversation. Sign in to Orris to start your own chat.