Describe the classification of fracture snd fracture healing- from orthopaedics book
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
I now have excellent, comprehensive content from multiple orthopaedic textbooks. Let me compose the full answer.
Classification of Fractures and Fracture Healing
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Pye's Surgical Handicraft 22nd Ed; Bailey & Love's Short Practice of Surgery 28th Ed; Rockwood & Green's Fractures in Adults 10th Ed 2025
PART 1: CLASSIFICATION OF FRACTURES
Fractures can be classified by several criteria. Most orthopaedic textbooks classify them along the following axes:
1. By Skin Integrity
Closed (Simple) Fracture
There is no communication between the fracture and the external environment. The skin over the fracture remains intact.
Open (Compound) Fracture
There is a wound communicating with the fracture site - either the bone pierces through the skin from inside, or an external injury penetrates to the bone. This is always a surgical emergency because of the risk of infection and osteomyelitis. A wound communicating with a mucosal surface (e.g., lung, bowel) is equally regarded as open.
Complicated Fracture
This term is reserved for fractures where important adjacent structures are injured - a major blood vessel, nerve, or internal organ.
2. By Fracture Line Pattern (Mechanism of Injury)
| Fracture Type | Mechanism | Key Features |
|---|---|---|
| Transverse | Direct blow / three-point force system | Fracture line perpendicular to the long axis; may have a 'butterfly' fragment; significant soft-tissue damage at fracture site |
| Spiral | Rotational stress (e.g., body rotating on a fixed foot) | Oblique winding fracture line; soft-tissue damage is away from fracture site; less local contusion |
| Oblique | Combined bending and compression | Similar mechanism to spiral but without rotational component |
| Comminuted | High-energy trauma | More than two fragments; fragments may be driven outward (burst fracture, especially in vertebrae) |
| Crush / Impacted | Direct axial compression into cancellous bone | Characteristic of vertebral bodies, calcaneum, tibial plateau; cancellous bone impacted into itself |
| Burst | Extreme compressive forces | Bone appears to explode with fragments driven outward; characteristic in vertebral fractures |
| Avulsion | Traction - tendon or ligament pulls off a fragment | Functionally equivalent to a complete ligamentous rupture; joint instability may result |
| Greenstick | Incomplete fracture in children | Pliable pediatric bone fractures on the tension side while remaining in continuity on the concave side; inherently stable |
| Stress (Fatigue) | Repetitive subthreshold loading | Accumulative microtrauma exceeds bone repair capacity; common in military recruits and athletes |
Pye's Surgical Handicraft 22nd Ed, p. 142-143
3. By Stability
Stable Fracture
The fracture components are unlikely to shift without further violence. Examples include impacted fractures, greenstick fractures, and those with intact soft-tissue hinge.
Unstable Fracture
After reduction, fragments tend to redisplace toward their pre-manipulation position. Most displaced fractures are unstable and require mechanical stabilization.
4. By Completeness
- Complete fracture - The bone is broken all the way through
- Incomplete fracture - The cortex is disrupted on only one side (e.g., greenstick, torus/buckle fractures in children)
5. By Anatomical Location
- Diaphyseal (shaft): proximal, middle, distal third
- Metaphyseal: the flared region between shaft and growth plate
- Epiphyseal: involving the joint surface; threatens articular cartilage and growth
- Intra-articular vs. Extra-articular
- Periarticular: near but not involving the joint
6. By Number of Fractures
- Isolated - single bone
- Multiple - more than one bone in the same limb or in different locations
- Segmental - two fracture lines isolating a middle segment of the same bone
7. Pathological Fracture
Occurs through bone weakened by pre-existing disease (tumor, osteoporosis, Paget's disease, osteomyelitis, bone cysts). The causative force is trivial relative to the resulting fracture.
8. Salter-Harris Classification (Growth Plate / Physeal Fractures in Children)
| Type | Description | Mnemonic (SALTR) |
|---|---|---|
| Type I | Pure separation through the physis; no bony fracture | S - Slip (physis alone) |
| Type II | Fracture through physis + metaphysis; most common | A - Above (metaphyseal fragment) |
| Type III | Fracture through physis + epiphysis; intra-articular | L - Lower (epiphyseal fragment) |
| Type IV | Fracture through metaphysis + physis + epiphysis | T - Through (all layers) |
| Type V | Crush injury of the physis; worst prognosis for growth | R - Rammed (crush) |
| Type VI | Injury to perichondral structures by direct trauma; rare; high chance of abnormal growth |
Bailey & Love's Short Practice of Surgery 28th Ed, p. 445
9. AO/OTA Classification
The AO Foundation (Arbeitsgemeinschaft fur Osteosynthesefragen) classification is the universal alphanumeric system used in research and surgical planning:
- Bone: numbered (e.g., 2 = humerus, 3 = radius/ulna)
- Segment: 1 = proximal, 2 = diaphyseal, 3 = distal
- Type: A (simple), B (wedge), C (complex/comminuted)
- Group and Subgroup further characterize fracture morphology
Rockwood & Green's Fractures in Adults 10th Ed 2025, p. 296
PART 2: FRACTURE HEALING
Fracture healing is a complex process requiring the recruitment of appropriate cells (fibroblasts, macrophages, chondroblasts, osteoblasts, osteoclasts) and expression of the right genes at the right time. A fracture initiates a sequence of inflammation, repair, and remodeling that can restore bone to its original state within months if each stage proceeds undisturbed.
Campbell's Operative Orthopaedics 15th Ed 2026, p. 3273
Two Fundamental Modes of Fracture Healing
A. Indirect (Secondary) Bone Healing - Most Common
Occurs when there is movement/strain at the fracture site. Involves callus formation. Analogous to a wound forming a scab that gradually returns to normal tissue.
Perren's Strain Theory governs what tissue forms at the fracture gap:
- Strain > 100% → fibrous tissue
- Strain < 10% → soft cartilaginous callus
- Strain < 2% → hard callus and progressive mineralization
"A little movement is good, too much movement is bad."
B. Direct (Primary) Bone Healing
Occurs only under absolute stability and cortical apposition (e.g., rigid plate fixation with compression). Heals directly with bone WITHOUT callus formation. Osteoclastic cutting cones cross the fracture line, followed by osteoblasts laying down lamellar bone - essentially the same remodeling process that occurs in normal bone homeostasis. No callus is visible on radiographs, which can make it difficult to judge when weight-bearing is safe.
Bailey & Love's Short Practice of Surgery 28th Ed, p. 445
Stages of Indirect Fracture Healing (Secondary Bone Healing)
The process is continuous but four overlapping stages are recognized:
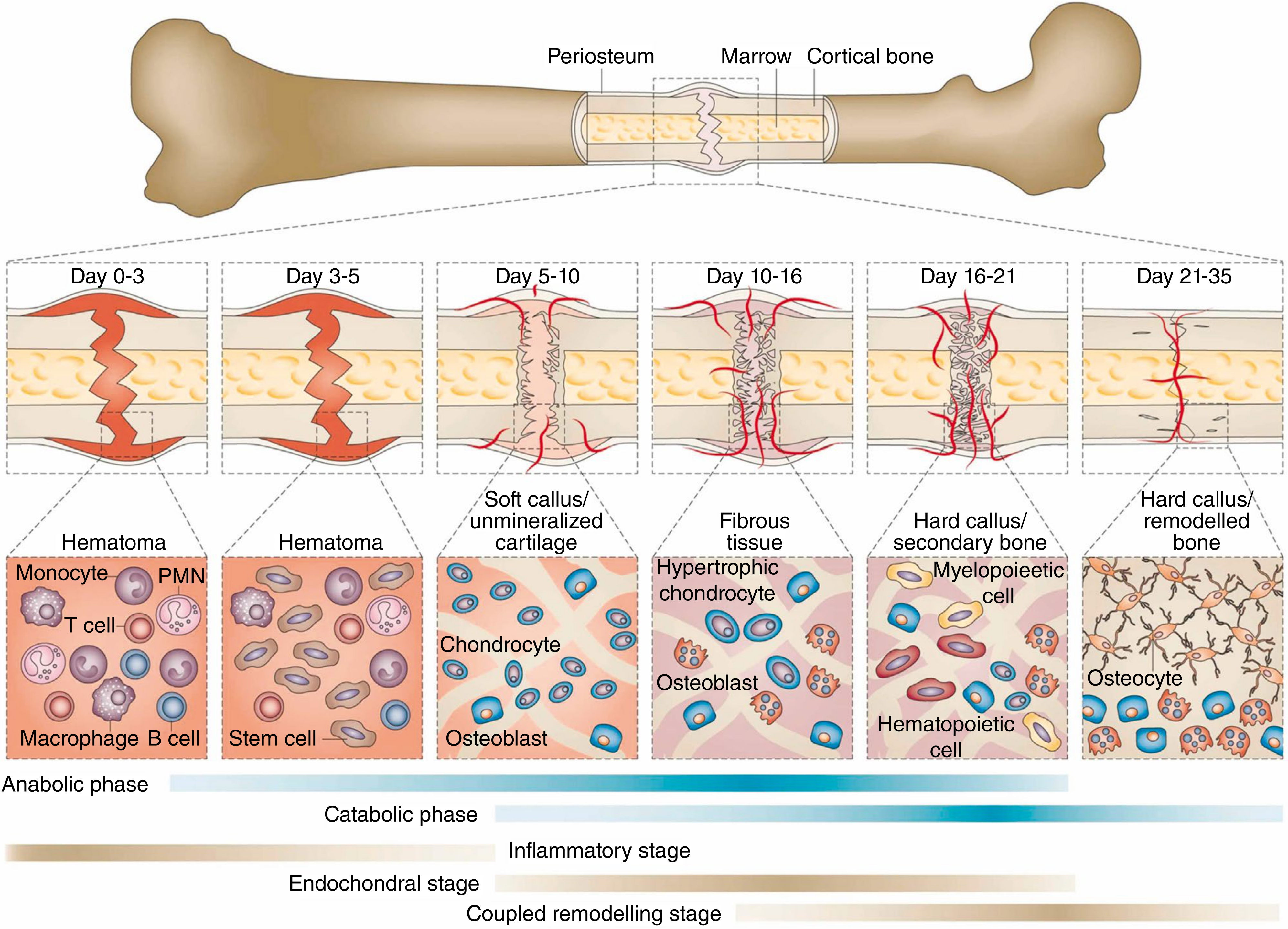
Fracture healing process at different phases, showing primal cell types found at each stage. Metabolic phases (anabolic and catabolic) and biological stages (inflammatory, endochondral bone formation, coupled remodeling) are shown. - Campbell's Operative Orthopaedics 15th Ed 2026, after Einhorn & Gerstenfeld, Nat Rev Rheumatol 2015
Stage 1: Haematoma Formation (Days 0-3)
- Rupture of blood vessels at the fracture site fills the gap with haematoma
- Haematopoietic cells, clots, and the haematoma form the initial framework
- Inflammatory cells invade and initiate lysosomal degradation of necrotic tissue
- Monocytes, PMNs (neutrophils), T cells, macrophages, and B cells are the primary cell types
- Capillary dilation, fluid exudation, and capillary budding begin
Stage 2: Granulation Tissue / Soft Callus Formation (Days 3-10)
- Beginning ~4-5 days after injury
- Pluripotential mesenchymal / stem cells invade and differentiate into fibroblasts, chondroblasts, and osteoblasts
- A soft cartilaginous callus forms (soft callus / unmineralized cartilage)
- Angiogenesis occurs in periosteal tissues and marrow space
- This routes appropriate cells to the fracture site
- A bed of granulation tissue forms
- Chondrocytes and osteoblasts are the key cells
Stage 3: Bony Callus Formation / Endochondral Ossification (Days 10-21)
- The cartilaginous callus undergoes endochondral ossification and is replaced with woven bone
- Hypertrophic chondrocytes and osteoblasts are prominent (Days 10-16)
- Hard callus / secondary bone forms (Days 16-21) with hematopoietic and myelopoietic cells
- At the end of this stage, calcified callus of immature (woven) bone remains
Stage 4: Bony Remodeling (Days 21-35 and continuing for years)
- Mineralization stiffens and strengthens the newly formed bone
- Hard callus is remodeled to cortical bone
- Osteocytes become the dominant cell type
- Involves intramembranous ossification, appositional new bone formation, and osteonal migration (creeping substitution)
- Radioisotope studies show increased activity at fracture sites long after painless function and radiographic union are achieved - remodeling continues for years
- In children (and to a lesser degree adults), bone remodels according to forces passing through it (Wolff's Law)
Campbell's Operative Orthopaedics 15th Ed 2026, p. 3273-3274; Pye's Surgical Handicraft 22nd Ed, p. 143
Terminology of Bone Healing
| Term | Definition |
|---|---|
| Clinical Union | Fracture site stable and pain free; progressively increasing stiffness through mineralization |
| Radiographic Union | Plain radiographs show bone trabeculae or cortical bone crossing the fracture site |
| Consolidation | Follows union; bone returns to normal strength; cortical pattern restored on radiograph |
| Remodeling | Long-term reshaping of bone along lines of mechanical stress |
| Delayed Union | Fracture slow to heal, has not healed within the expected time frame |
| Non-union | Fracture fails to heal and shows no potential to heal without further intervention; no clinical/radiological improvement over 3 months; formally diagnosed at 6 months |
| Malunion | Fracture has healed but in a position of deformity |
Types of Non-union:
- Atrophic non-union - Biological problem; lack of stimulus or blood supply; no callus
- Hypertrophic non-union - Too much movement at the fracture site; elephant-foot appearance; biologically active but mechanically insufficient
- Infected non-union - Infection has compromised the healing environment
Bailey & Love's Short Practice of Surgery 28th Ed, p. 445-446
Factors Affecting Fracture Healing
Systemic Factors
- Age (healing faster in young patients)
- Nutritional status
- Hormonal factors (growth hormone, thyroid, PTH)
- Diseases: diabetes, malignancy, pulmonary insufficiency, immunodeficiency
- Vitamin deficiencies (C, D)
- Smoking - the single most notable inhibitory factor; delays both fracture and wound healing significantly and increases nonunion risk
- Medications: NSAIDs (conflicting data), fluoroquinolone antibiotics (implicated in slowing bone healing), corticosteroids
Local Factors
- Severity of injury and high-energy trauma
- Degree of fracture displacement
- Neurovascular disruption
- Soft-tissue interposition
- Loss of bone (segmental defect)
- Blood supply to the periosteum and nutrient artery
- Infection (especially in open fractures)
- Peripheral vascular disease / diabetes (microvascular)
Treatment Factors
- Extent of surgical trauma
- Type of fixation and degree of rigidity
- Overdistraction of fragments
- Load-induced deformation
- Poor reduction and malalignment
Campbell's Operative Orthopaedics 15th Ed 2026, p. 3274
Requirements for Bone Regeneration (Bone Graft)
Three essential components:
- Osteoconduction - Scaffolding that allows bone ingrowth
- Osteoinduction - Ability to induce production of osteoblasts (e.g., BMPs)
- Cellular Osteogenesis - Live osteogenic cells (osteoblasts and osteocyte precursors)
Autologous bone graft (from iliac crest or local bone) contains all three components and remains the gold standard.
Campbell's Operative Orthopaedics 15th Ed 2026, p. 3273-3275
describe supracondyler fracture of Humrus, its classification and Management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Supracondylar Fracture of the Humerus
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Rosen's Emergency Medicine; Bailey & Love's Short Practice of Surgery 28th Ed; Grainger & Allison's Diagnostic Radiology
DEFINITION AND EPIDEMIOLOGY
A supracondylar fracture is a fracture of the distal humerus just above the condyles, through the thin metaphyseal bone between the coronoid fossa anteriorly and the olecranon fossa posteriorly.
- Most common elbow fracture in children (peak age 5-8 years)
- The most common fracture treated surgically by pediatric orthopedic surgeons
- During childhood, ligaments around the elbow are stronger than the underlying bone, so falls tend to produce bone fractures rather than ligamentous injuries
- The distal humerus ossifies at multiple centers - the CRITOE sequence is important to know to avoid misidentifying ossification centers as fracture fragments
CRITOE - Order of ossification center appearance:
| Ossification Center | Age at Appearance | Age at Closure |
|---|---|---|
| Capitellum | 6-12 months | 14 yrs |
| Radial head | 4-5 years | 16 yrs |
| Internal (medial) epicondyle | 5-7 years | 15 yrs |
| Trochlea | 8-10 years | 14 yrs |
| Olecranon | 8-9 years | 14 yrs |
| External (lateral) epicondyle | 9-13 years | 16 yrs |
Rosen's Emergency Medicine, p. 3304
MECHANISM OF INJURY
Extension Type (95% - Most Common)
- Fall onto an outstretched, extended hand (FOOSH)
- The body's weight drives the humerus forward while the elbow hyperextends
- The distal fragment is displaced posteriorly and superiorly
- The sharp proximal humeral shaft end can injure the brachial artery and median/anterior interosseous nerve anteriorly
Flexion Type (5% - Rare)
- Direct blow or fall onto a flexed elbow
- The distal fragment is displaced anteriorly
- More commonly associated with ulnar nerve injury
- Higher rate of open reduction required due to ulnar nerve entrapment risk
CLINICAL FEATURES
Presentation:
- Painful, swollen elbow after a fall
- Child holds the arm in extension with slight pronation
- "S" deformity of the distal humerus on lateral view
- Puckering, dimpling, or anterior bruising over the antecubital fossa suggests the proximal humeral shaft has penetrated the brachialis muscle - this predicts difficulty with closed reduction
Immediate Assessment - Neurovascular Status:
Assess for the 5 "P"s of arterial compromise:
- Pain (especially pain with passive finger extension - a sign of compartment syndrome)
- Pallor
- Pulselessness
- Paralysis
- Paresthesias
RADIOGRAPHIC ASSESSMENT
Views required: AP (elbow extended if possible) + true lateral (elbow flexed at 90°)
1. Anterior Humeral Line
On a true lateral view, a line drawn along the anterior humeral cortex should pass through the posterior two-thirds of the capitellum. If the capitellum is anterior to this line or the line passes through only the anterior one-third, a posteriorly displaced supracondylar fracture is present.

Anterior humeral line (solid) and proximal radial line (dashed) bisecting the capitellum - normal elbow. Rosen's Emergency Medicine, p. 3304
2. Baumann Angle
On the AP view, this is the angle formed between:
- A line drawn along the growth plate of the capitellum
- A line drawn down the long axis of the humerus
Normal = 70-75 degrees. Helpful for detecting subtle fractures and assessing adequacy of reduction (especially varus/valgus alignment). A decreased Baumann angle indicates cubitus varus.
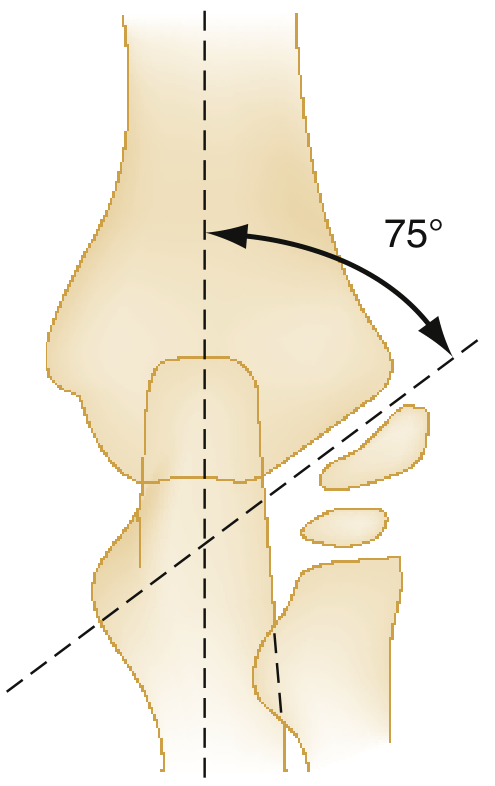
Baumann angle - normally 70 to 75 degrees. Rosen's Emergency Medicine, p. 3306
3. Fat Pad Signs
On a lateral radiograph with the elbow at 90°:
- Anterior fat pad "sail sign" - bulging anterior fat pad; suggests effusion and occult fracture (a thin anterior fat pad can be normal)
- Posterior fat pad sign - always pathological; indicates a joint effusion/haemarthrosis; strongly suggests occult fracture even when no fracture line is visible
CLASSIFICATION
Gartland Classification (Extension-Type - Most Used)
| Type | Description | Key Feature |
|---|---|---|
| Type I | Nondisplaced fracture | Cortex intact; may only show fat pad sign |
| Type II | Displaced with intact posterior cortex | Posterior cortex acts as hinge; capitellum displaced anterior to AHL |
| Type III | Completely displaced; no cortical contact | - |
| Type IIIA | Posteromedial rotation of distal fragment | Most common subtype |
| Type IIIB | Posterolateral rotation of distal fragment | Higher risk of radial nerve injury |
(Adapted from Gartland JJ, Surg Gynecol Obstet 1959;109:145)
A Type IV has been added by some authors (Leitch et al.) to describe multidirectional instability - the fracture is unstable in both flexion and extension, which is only apparent under anaesthesia during reduction.
NEUROVASCULAR INJURIES
The supracondylar region is close to major neurovascular structures; injury is not uncommon:
| Structure Injured | Mechanism | Clinical Test |
|---|---|---|
| Anterior Interosseous Nerve (branch of median nerve) - most common | Posterolateral displacement (Type IIIB) | Cannot form "OK" sign - loss of FPL and FDP to index finger |
| Radial nerve | Posterolateral displacement | Loss of wrist and finger extension |
| Median nerve | Posteromedial displacement (Type IIIA) | Sensory loss on thumb, index, middle finger |
| Ulnar nerve | Flexion-type injuries | Loss of intrinsic hand function; sensory loss ring and little finger |
| Brachial artery | Sharp proximal fragment pierces anteriorly | Absent radial pulse; pallor; white pulseless hand |
Most nerve injuries are neuropraxia and resolve with fracture reduction and swelling resolution.
Rosen's Emergency Medicine, p. 3305
MANAGEMENT
Gartland Type I - Undisplaced
- Posterior long-arm splint or collar and cuff with elbow at 90° flexion, forearm neutral or pronated
- Immobilization for 3 weeks
- Follow-up with orthopaedics within 24 hours for casting and repeat radiograph
- Progressive mobilization after cast/splint removal
Gartland Type II - Displaced with Intact Posterior Cortex
- Closed reduction under sedation or general anaesthesia
- If reduction is maintained with < 90° of elbow flexion → above-elbow cast for 3-4 weeks
- If > 90° of flexion is required to hold the reduction (dangerous because of vascular compromise risk) → percutaneous K-wire fixation + above-elbow cast
- Avoid deep flexion if there is significant swelling - risk of Volkmann's ischaemic contracture
Gartland Type III - Completely Displaced
- Admission required
- Operative closed reduction and percutaneous K-wire pinning is the standard of care
- Prone to neurovascular compromise - emergent orthopaedic consultation
- If closed reduction fails or neurovascular compromise persists → open reduction
K-wire Configuration:
- Lateral-entry parallel or divergent K-wires (2 or 3 lateral wires) - preferred to avoid ulnar nerve injury
- Crossed K-wires (one lateral, one medial) - provides more rotational stability but risks ulnar nerve injury with the medial pin; should be placed with elbow partially extended to protect the nerve
- Wires are typically removed in clinic at 3-4 weeks
Special Situations
White Pulseless Hand (absent pulse + ischaemic limb):
- Surgical emergency - immediate urgent reduction
- If pulse does not return after reduction → emergent vascular exploration and repair of brachial artery
Pink Pulseless Hand (absent pulse but perfused limb):
- More controversial management
- If adequate perfusion, no compartment syndrome, no neurological injury: reduce and stabilise, take an expectant approach
- Pulse often returns within 24-48 hours
- If perfusion worsens → vascular exploration
Open Fractures / Failed Closed Reduction:
- Open reduction through anterior (cubital) or posterior approach
COMPLICATIONS
| Complication | Details |
|---|---|
| Volkmann's Ischaemic Contracture | Most feared; results from missed compartment syndrome; excessive swelling + deep elbow flexion compromises forearm perfusion; causes fibrous contracture of forearm flexors |
| Cubitus Varus ("Gunstock Deformity") | Most common late complication of malunion; caused by posteromedial displacement and varus malreduction; cosmetic rather than functional in most cases; remodels poorly; requires corrective supracondylar osteotomy |
| Cubitus Valgus | Less common; results from lateral condylar malunion; risk of delayed ulnar nerve palsy |
| Nerve Injury | Usually neuropraxia; resolves with fracture healing; persistent deficit after 3 months warrants exploration |
| Stiffness | Loss of full extension is common; usually recovers over 12-18 months |
| Myositis Ossificans | Rare; caused by repeated manipulation or forced passive movement during rehabilitation |
| Pin-tract Infection | After percutaneous pinning; usually superficial and resolves with pin removal |
| Avascular Necrosis of Trochlea | Rare; from disrupted blood supply to trochlea |
SUMMARY - MANAGEMENT ALGORITHM
Supracondylar Fracture of Humerus
├── Type I (Undisplaced)
│ └── Collar & cuff / posterior splint × 3 weeks
│
├── Type II (Posterior cortex intact)
│ ├── Closed reduction
│ ├── If stable at <90° flexion → Above-elbow cast × 3-4 weeks
│ └── If unstable / >90° needed → Percutaneous K-wires + cast
│
└── Type III (No cortical contact)
├── Admit → Closed reduction + percutaneous K-wire pinning
├── White pulseless hand → Emergency reduction ± vascular exploration
└── Failed closed reduction → Open reduction
Sources: Bailey & Love's Short Practice of Surgery 28th Ed, p. 462; Rosen's Emergency Medicine, p. 3304-3307; Campbell's Operative Orthopaedics 15th Ed 2026; Grainger & Allison's Diagnostic Radiology, p. 1145
short notes on 1)TARDY ulnar nerve palsy 2)Colles fracture 3) Volkmann's Ischaemic contracture 4) FAT EMBOLISM
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content for all four topics. Let me compile the short notes.
Short Notes on Four Orthopaedic Topics
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; S. Das Manual on Clinical Surgery 13th Ed; Bailey & Love's Short Practice of Surgery 28th Ed; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Murray & Nadel's Textbook of Respiratory Medicine; Pye's Surgical Handicraft 22nd Ed
1. TARDY ULNAR NERVE PALSY
Definition
Tardy (meaning "late" or "delayed") ulnar nerve palsy is a late-onset progressive ulnar nerve paralysis that develops weeks, months, or even years after a bony injury around the elbow - not at the time of injury.
Causes / Aetiology
The common underlying mechanism is gradual stretching, friction, or compression of the ulnar nerve at the elbow due to:
-
Cubitus valgus (most classic cause) - from malunion of a lateral condyle fracture of the humerus in children. As the child grows, progressive valgus deformity develops, stretching the ulnar nerve in its groove behind the medial epicondyle over many years.
-
Callus formation after supracondylar fracture - bony callus at the fracture site gradually compresses the ulnar nerve.
-
Malunion of medial epicondyle fracture - ulnar nerve becomes entrapped in callus if anterior transposition was not performed at the time of surgery.
-
Shallow ulnar groove on the posterior medial epicondyle - causes recurrent subluxation or dislocation of the ulnar nerve (found in 16.2% of 2000 elbows in one series), with repeated microtrauma on elbow flexion.
-
Hypoplasia of the humeral trochlea or inadequate fibrous arch.
-
Elbow dislocations, contusions, and post-traumatic fibrosis.
(Note: Cubital tunnel syndrome - compression at the cubital tunnel without antecedent trauma - is technically distinct but has a similar presentation.)
Clinical Features
Sensory loss:
- Medial side of the hand, entire little finger, and medial half of the ring finger
Motor weakness / paralysis (ulnar nerve at the elbow level):
| Muscle | Function Lost |
|---|---|
| Flexor carpi ulnaris | Weak wrist flexion and ulnar deviation |
| Medial half of Flexor digitorum profundus | Weak flexion of ring and little finger DIP joints |
| Hypothenar muscles (abductor, flexor, opponens digiti minimi) | Weak little finger abduction/opposition |
| All interossei | Weak finger abduction/adduction; loss of fine pinch |
| 3rd and 4th lumbricals | Clawing of ring and little fingers |
| Adductor pollicis | Weak pinch (positive Froment's sign - patient uses FPL to compensate) |
Classic deformity: "Ulnar claw hand" (Benediction deformity) - hyperextension at MCP joints and flexion at IP joints of ring and little fingers (more pronounced if nerve is injured at the wrist, where FDP is spared - "lower ulnar palsy is more clawed than high ulnar palsy").
Froment's sign: Patient pinches a sheet of paper between thumb and index finger; uses FPL (median nerve) to compensate for weak adductor pollicis - thumb IP joint flexes.
Management
- Conservative: Elbow padding, avoidance of sustained elbow flexion
- Surgical decompression: Simple decompression of the cubital tunnel
- Anterior transposition of the ulnar nerve (subcutaneous, intramuscular, or submuscular) - moves the nerve to a position where it is no longer stretched by valgus deformity or elbow flexion; this is the preferred treatment in tardy palsy
- Corrective osteotomy if significant cubitus valgus persists
- Medial epicondylectomy - removes the bony prominence causing compression
Campbell's Operative Orthopaedics 15th Ed 2026; S. Das Manual on Clinical Surgery 13th Ed, p. 145
2. COLLES' FRACTURE
Definition
A Colles' fracture is a transverse fracture of the distal radial metaphysis (within 2 cm of the radiocarpal joint) with:
- Dorsal displacement and dorsal angulation of the distal fragment
- Radial shortening (impaction)
- Loss of normal volar tilt of the radial articular surface
First described by Abraham Colles in 1814.
Mechanism
- Fall on an outstretched hand (FOOSH) with the wrist in dorsiflexion
- Commonest in postmenopausal women with osteoporosis (most common fragility fracture)
- Also seen in young adults after high-energy trauma
Pathological Anatomy
- Fracture line within 2 cm of the radial articular surface
- Dorsal comminution is common (compression forces on the dorsal cortex)
- May extend intra-articularly into the radiocarpal joint ("die-punch fracture") or radioulnar joint
- Ulnar styloid fracture is commonly associated - indicates triangular fibrocartilage complex (TFCC) injury
Clinical Features
"Dinner-fork deformity" (or "silver-fork deformity"):
- Seen on the lateral view of the wrist
- The dorsal displacement of the distal fragment creates a step resembling the profile of a dinner fork
- Wrist is in characteristic dorsiflexion posture
- Swelling, tenderness, and bruising over the distal forearm
Neurological: Palmar paraesthesias from pressure on the median nerve (most common nerve injury) - acute from contusion, traction, or secondary to swelling.
Radiological Features
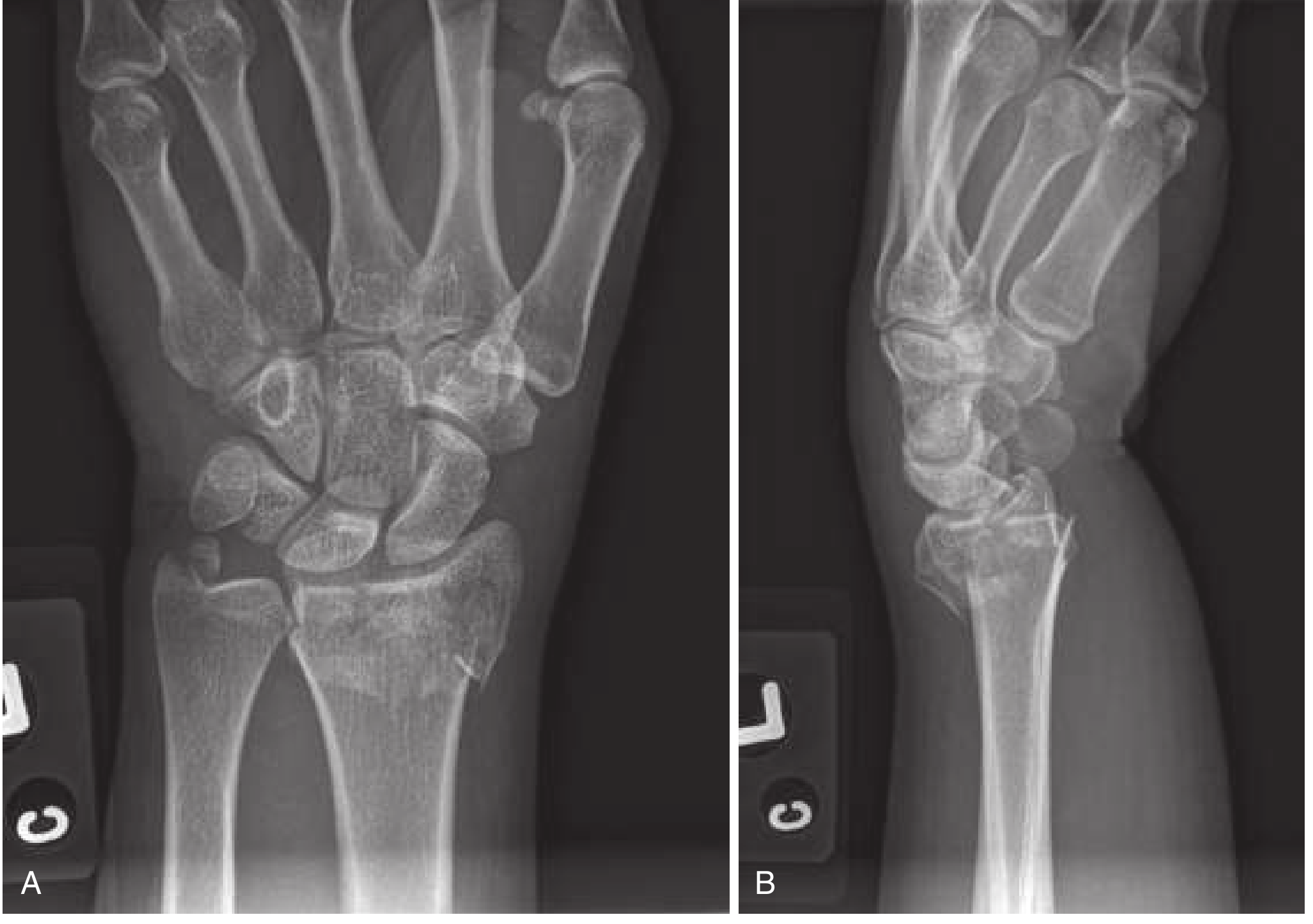
(A) PA view: fracture with radial shortening, intra-articular extension, associated ulnar styloid fracture. (B) Lateral: dorsal displacement and classic dinner fork deformity. - Rosen's Emergency Medicine
Normal values to restore on reduction:
- Volar tilt: 11-12° (range 0-28°); minimum acceptable = 0° (neutral)
- Radial inclination: 22-23°
- Radial length: 11 mm
Unstable fracture criteria:
- Dorsal angulation > 20°
- Intra-articular extension
- Marked comminution
-
1 cm radial shortening
- Distal radioulnar joint instability
Management
Stable / Undisplaced:
- Compression dressing and below-elbow backslab/splint
- Orthopaedic review within 7-10 days
Displaced (most cases):
- Closed reduction under anaesthesia (haematoma block, Bier block, or regional nerve block)
- Technique: traction with finger traps → distal and palmar push on fragment → restore volar tilt
- Double sugar-tong splint (not circumferential cast for 24 hours - allow for swelling)
- Short arm cast or above-elbow cast for 4-6 weeks
- Repeat radiograph at 1 week to check maintenance of reduction
Unstable / Comminuted / Intra-articular:
- Percutaneous K-wire fixation (Kapandji technique)
- External fixation (distraction fixator)
- Volar locking plate (ORIF) - preferred for young patients, intra-articular fractures
Open/neurovascularly compromised: Immediate orthopaedic referral.
Complications
| Complication | Notes |
|---|---|
| Malunion / Dinner-fork deformity | Most common; commoner in elderly/osteoporotic |
| Median nerve injury / Carpal tunnel syndrome | Acute from displacement or late from callus |
| Rupture of extensor pollicis longus tendon | Attrition rupture 4-12 weeks post injury over Lister's tubercle |
| TFCC injury / DRUJ instability | From associated ulnar styloid fracture |
| Reflex Sympathetic Dystrophy (CRPS Type I) | Sudeck's atrophy - burning pain, vasomotor changes |
| Finger and wrist stiffness | From prolonged immobilization |
| Post-traumatic arthritis | After intra-articular extension |
Rosen's Emergency Medicine, p. 611-612; Tintinalli's Emergency Medicine, p. 1847
3. VOLKMANN'S ISCHAEMIC CONTRACTURE
Definition
Volkmann's ischaemic contracture (VIC) is a fixed fibrous contracture of the muscles of the forearm (predominantly the flexors) resulting from irreversible ischaemia caused by an untreated or inadequately treated acute compartment syndrome of the forearm.
It is the most feared complication of paediatric supracondylar fractures of the humerus.
Pathophysiology
The forearm is enclosed in tight fascial compartments (volar and dorsal). When pressure within these compartments rises - from swelling, haematoma, or external compression (tight cast) - capillary blood flow is reduced below the level needed for tissue viability:
Ischaemia → Muscle necrosis → Fibrosis and contracture
The flexor digitorum profundus in the middle third of the forearm is the first and most severely affected muscle (most centrally placed, most susceptible to ischaemia). The median and ulnar nerves are also compromised.
Causes
- Supracondylar fracture of the humerus in children (classical cause)
- Any fracture or dislocation around the elbow or forearm
- Tight plaster cast / bandage
- Crush injuries of the forearm
- Brachial artery injury
- Prolonged limb compression (e.g., drug overdose)
- Excessive deep elbow flexion after reduction of supracondylar fractures
Clinical Features (Established VIC)
The typical posture includes:
- Elbow flexion
- Forearm pronation
- Wrist flexion
- Thumb adduction
- MCP joints in extension
- Fingers (IP joints) in flexion
Sensory loss in median and/or ulnar nerve distributions depending on severity.
Classification and Treatment
| Severity | Clinical Findings | Treatment |
|---|---|---|
| Mild (Localized) | Flexion contractures of 2-3 fingers; minimal/absent sensory changes; no intrinsic contractures | Physiotherapy + dynamic splinting; muscle-tendon lengthening / release after 3 months |
| Moderate | Flexion contractures all digits + thumb + wrist; sensory changes in median/ulnar distribution; intrinsic minus deformity | Excision of necrotic muscle + neurolysis; muscle sliding operation (Page's operation) |
| Severe | All of the above + wrist flexion contracture + forearm pronation contracture + severe sensory loss | Excision + neurolysis + tendon transfers (brachioradialis to FPL, ECRL to FDP) or free functioning muscle transfer (gracilis) |
Prevention (Most Important!)
- Early diagnosis and emergency fasciotomy of forearm compartments when compartment syndrome is suspected
- Do not apply circumferential cast acutely; use back-slab only
- Avoid deep elbow flexion after supracondylar fracture reduction if there is significant swelling
- If > 90° of flexion is needed to hold reduction → K-wire fixation instead
- Monitor the "5 Ps" - Pain, Pallor, Pulselessness, Paraesthesia, Paralysis
Campbell's Operative Orthopaedics 15th Ed 2026, p. 4460; Bailey & Love's Short Practice of Surgery 28th Ed; Tintinalli's Emergency Medicine
4. FAT EMBOLISM SYNDROME (FES)
Definition
Fat embolism syndrome (FES) is a serious clinical syndrome resulting from fat globules entering the pulmonary and systemic circulation, most commonly after fracture of long bones. It is characterized by a triad of:
- Respiratory distress / hypoxaemia
- Neurological abnormalities (confusion, restlessness, deteriorating consciousness)
- Petechial rash
Incidence
- 1-2% of patients with isolated long bone fractures
- 5-10% of patients with multiple fractures
- Most common after fractures of the tibia and femur (marrow-rich bones)
- Also after hip fractures in the elderly and after intramedullary nailing (surgical FES)
- Incidence rises with the number of fractures
- Mortality once FES is established: 10-20%
Pathophysiology
Two mechanisms are proposed:
1. Mechanical Theory (Embolic):
- Trauma disrupts medullary fat cells → fat globules enter torn venous sinusoids → travel to pulmonary capillaries → mechanical obstruction → V/Q mismatch → hypoxaemia
- Fat particles can traverse pulmonary capillaries or patent foramen ovale → systemic circulation → brain, skin, kidneys
2. Biochemical (Metabolic) Theory - Probably More Important:
- Lipases break down neutral fat → release of free fatty acids (FFAs)
- FFAs cause diffuse vasculitis with leakage from cerebral, pulmonary, and other vascular beds
- Explains the lag time between injury and syndrome onset
- Also associated with hypovolaemia and the shock response
Timing
- Symptoms typically appear 12-72 hours (Pye's: 3-10 days) after the inciting injury
- Appearance within 24-48 hours of intramedullary nailing is well recognized
Clinical Features
Early signs:
- Respiratory: Dyspnoea, tachypnoea, hypoxaemia (PaO₂ < 60 mmHg) - earliest and most common
- Neurological: Restlessness, confusion, disorientation, deteriorating GCS - early sign; may progress to coma
Later signs:
- Petechial rash - pathognomonic; distributed over the head, neck, anterior chest, and axillae (conjunctiva and retina also); present in only 20-50% of cases - absence does not exclude FES
- Fever, tachycardia
- Retinal fat emboli visible on fundoscopy
- Jaundice (from hepatic involvement)
- Renal involvement
- Thrombocytopenia
Investigations
No single test is diagnostic - FES is a clinical diagnosis in the right context.
| Investigation | Finding |
|---|---|
| ABG / SpO₂ | Hypoxaemia (PaO₂ < 60 mmHg on room air) - most sensitive early finding |
| CXR | Bilateral "snowstorm" opacities |
| CT Chest | Ground glass opacities + consolidation |
| FBC | Thrombocytopenia, anaemia |
| Urine microscopy | Fat globules in urine (50% of patients within 3 days) |
| Serum lipase | Elevated |
| Blood film | Fat globules in circulation |
| Fundoscopy | Retinal fat emboli |
Gurd's Criteria (for diagnosis)
Major criteria (1 required):
- Petechial rash
- Respiratory insufficiency (PaO₂ < 60 mmHg, FiO₂ > 0.4)
- Cerebral involvement (not head injury)
Minor criteria:
- Pyrexia > 38.5°C
- Tachycardia > 120/min
- Retinal fat emboli
- Fat in urine
- Thrombocytopenia (> 50% drop)
- High ESR
- Fat globules in sputum
(Diagnosis = 1 major + 4 minor + fat macroglobulinaemia)
Management
Primarily supportive - no specific treatment proven effective:
- Respiratory support - supplemental oxygen; may require intubation and mechanical ventilation (ARDS management protocol) in ICU
- Haemodynamic support - IV fluids, inotropes if needed
- Early fracture stabilization - intramedullary nailing reduces fat release compared to prolonged traction; early fixation may reduce FES incidence
- Corticosteroids - high-dose methylprednisolone (controversial; some evidence for prevention in high-risk patients; not proven once FES is established)
- Heparin, albumin, dextran - suggested but none proven effective
- Supportive ICU care - careful fluid balance, nutritional support
Prognosis: Most uncomplicated fat embolism resolves without severe sequelae with meticulous supportive care. Severe FES with widespread CT opacities and ARDS is life-threatening with mortality 10-20%.
Murray & Nadel's Textbook of Respiratory Medicine; Rosen's Emergency Medicine, p. 543; Pye's Surgical Handicraft 22nd Ed; Bailey & Love's Short Practice of Surgery 28th Ed
This is a shared conversation. Sign in to Orris to start your own chat.