Giant cell lesion of bone
Reading File
Finding Sources
Searching PubMed
"giant cell tumor" OR "giant cell lesion" AND bone
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from all major sources. Let me compile a thorough, well-structured answer.
Giant Cell Tumor of Bone (GCTB)
Giant cell tumor of bone (also called osteoclastoma) is a locally aggressive but histologically benign neoplasm composed of neoplastic mononuclear stromal cells surrounded by abundant reactive osteoclast-type multinucleate giant cells. It accounts for approximately 5% of all bone neoplasms and is one of the classic "aggressive benign" tumors encountered in clinical practice.
Epidemiology
-
Peak incidence: 20-40 years of age (skeletally mature adults)
-
Slight female predominance
-
Rare in skeletally immature patients
-
Typically solitary; 1-2% of cases present with multicentric (synchronous or metachronous) lesions
-
Campbell's Operative Orthopaedics 15th Ed 2026
Pathogenesis / Molecular Basis
The neoplastic cell population is the mononuclear stromal cell, which is a primitive osteoblast precursor. Key mechanisms:
- Neoplastic stromal cells overexpress RANKL (Receptor Activator of Nuclear Factor kB Ligand)
- RANKL drives proliferation and differentiation of osteoclast precursors into mature, functioning osteoclasts
- The abundant osteoclasts - not the neoplastic cells themselves - destroy bone through local resorption
- Normal osteoblast-osteoclast feedback is lost, resulting in progressive, destructive bone resorption
- The neoplastic stromal cells harbor mutations in H3-3A (the gene encoding histone 3.3, a chromatin packaging protein) - the mechanism by which this drives tumorigenesis remains unclear
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Location
- Epiphyses of long bones - this is the hallmark location, distinguishing GCTB from most other bone tumors
- Most common sites (in order):
- Distal femur
- Proximal tibia (these two together constitute the majority - "around the knee")
- Distal radius (tends to be more aggressive)
- Sacrum (for axial involvement)
- Spinal involvement otherwise uncommon
- Lesion abuts the subchondral bone and may extend into the metaphysis
- In skeletally immature patients (rare), arises in the metaphysis and likely extends into the epiphysis after physeal closure
Clinical Features
- Pain - the most common symptom; initially activity-related, later at rest
- Pathologic fracture - present in 10-30% of patients at initial diagnosis
- Arthritis-like symptoms due to proximity to the joint
- Swelling over the affected area
- Rarely: intraarticular extension (subchondral bone usually remains intact)
Imaging
Plain Radiograph
- Purely lytic (radiolucent), no matrix calcification
- Eccentric epiphyseal location, extending to or abutting subchondral bone
- Zone of transition may be poorly defined (aggressive lesions) or show a partial rim of reactive bone (less aggressive)
- Cortical expansion or breakthrough common
- Soft-tissue extension visible in aggressive cases

MRI
-
T1: dark (low signal)
-
T2: bright (high signal)
-
Fluid-fluid levels visible in ~20% of cases - indicates secondary aneurysmal bone cyst (ABC) component
-
Best modality to determine intra-osseous and soft-tissue extent
-
Campbell's Operative Orthopaedics 15th Ed 2026
Pathology / Histology
Gross
- Large, red-brown mass (due to hemosiderin and vascular stroma)
- Frequently undergoes cystic degeneration
- Destroys overlying cortex, creating a bulging soft-tissue mass bounded by a thin shell of reactive bone
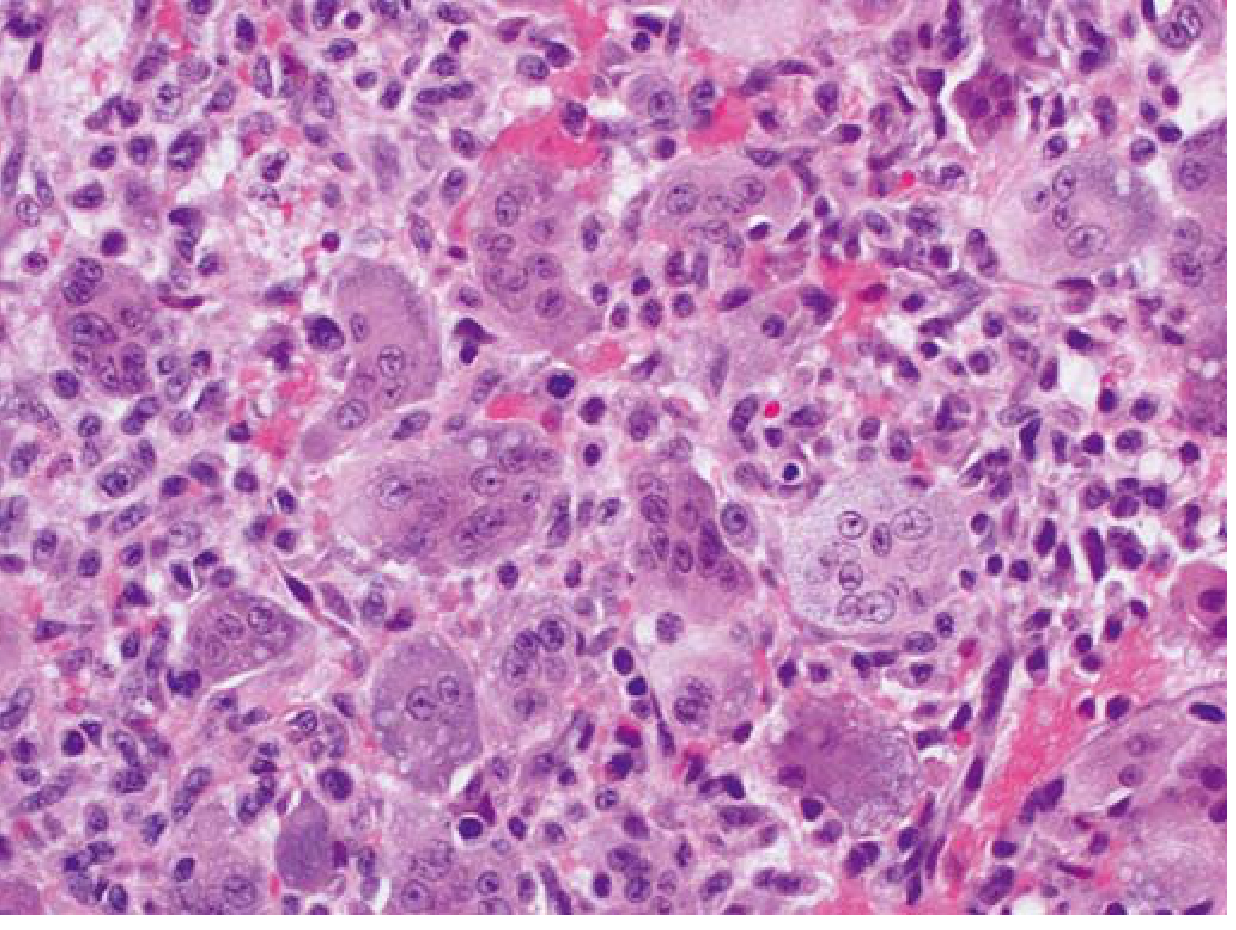
Microscopy
- Osteoclast-type giant cells with 40-100+ nuclei per cell - distributed uniformly throughout the lesion
- Key diagnostic feature: the nuclei of the mononuclear stromal cells are identical to the nuclei within the giant cells - this helps distinguish GCTB from other giant-cell-containing lesions
- Background: uniform oval mononuclear stromal cells (the true neoplastic component)
- May show: storiform spindle cell areas, reactive bone formation, foamy macrophages, secondary ABC changes
- Necrosis and mitotic activity may be prominent
- Histologic grading has no prognostic significance - no grading system has been validated
Staging (Enneking / Campanacci)
GCTB is most often staged using the Campanacci system:
- Stage 1 (Latent/Inactive): well-defined margin with reactive bone rim; intracortical
- Stage 2 (Active): expanded cortex, well-marginated; most common at presentation
- Stage 3 (Aggressive): cortical destruction, soft-tissue extension; poorly marginated
Most GCTB present as stage 2 or stage 3 at diagnosis.
Malignant Giant Cell Tumor of Bone (MGCTB)
A rare but important entity (<10% of cases):
- Primary MGCTB: sarcomatous cells identified alongside conventional GCTB at initial biopsy
- Secondary MGCTB: sarcomatous transformation in a previously treated GCTB, often years later; strongly associated with prior radiotherapy
- Most common sarcoma subtype: osteosarcoma
- Radiographic and clinical features indistinguishable from aggressive conventional GCTB
- Definitive diagnosis requires biopsy
Treatment
Intralesional Curettage (Standard)
- Extended/aggressive curettage with power burr (enlarging cavity 1-2 cm in all directions) is the standard surgical approach
- Cortical window must be at least as large as the lesion to prevent "leaving tumor around the corner"
- Recurrence rates historically >50% with simple curettage; with modern technique (MRI-guided extent, extended curettage + adjuvants): 5-15%
Adjuvants
Used after curettage to eliminate residual tumor cells:
- Argon beam coagulator (preferred at many centers - effective, easy, low complication rate)
- Phenol or liquid nitrogen - historically used but associated with pathologic fracture, wound healing problems, and nerve injury
- Bisphosphonates (local or systemic) - preliminary evidence suggests may reduce recurrence
Cavity Filling
- Methyl methacrylate bone cement (preferred): provides immediate stability, allows detection of recurrence (appears as expanding radiolucency adjacent to cement), may kill residual cells via polymerization heat
- Autograft / allograft bone / artificial substitutes: restore bone stock but require prolonged joint protection and make recurrence detection harder
- Cement can be reinforced with crossed or divergent screws, or a periarticular plate
Wide Resection
Required for:
- Stage 3 tumors unresponsive to curettage
- Recurrent lesions
- Tumors where curettage would be inadequate (e.g., distal radius - primary resection with proximal fibular autograft reconstruction)
- Reconstructive options: hemicondylar osteoarticular allograft, rotating hinge endoprosthesis
Denosumab (RANKL Inhibitor)
-
Highly effective medical treatment by blocking RANKL - removes the osteoclast-stimulating signal
-
Induces tumor reduction and bone formation
-
Indications: unresectable tumors, resection would cause significant functional morbidity or deformity, recurrent disease
-
Does not eliminate the neoplastic stromal cells; disease can recur after cessation
-
Standard of care for surgically challenging GCTB
-
Campbell's Operative Orthopaedics 15th Ed 2026; Robbins & Kumar Basic Pathology
Prognosis and Metastasis
| Outcome | Rate |
|---|---|
| Local recurrence after curettage (modern technique) | 5-15% |
| Pulmonary metastases | ~3-4% |
| Mortality with pulmonary metastases | ~15% |
| Malignant transformation | <10% |
- Pulmonary metastases ("benign metastasizing GCT") retain benign histology; some spontaneously regress, others remain asymptomatic; most can be cured by surgical excision of metastases
- Risk factors for pulmonary metastasis: stage 3 disease, recurrent tumors, aggressive radiographic features
Differential Diagnosis (Other Giant-Cell-Containing Lesions)
| Lesion | Key Distinguishing Feature |
|---|---|
| Aneurysmal Bone Cyst (ABC) | Metaphyseal, blood-filled spaces, USP6 rearrangement, younger age group |
| Brown tumor of hyperparathyroidism | Elevated PTH/Ca²+, diffuse skeletal involvement |
| Chondroblastoma | Epiphyseal, younger patients (open physis), "chicken-wire" calcification |
| Tenosynovial giant cell tumor | Soft tissue, periarticular; RANKL/CSF1 driven |
| Non-ossifying fibroma | Metaphyseal cortical lesion, younger age, no giant cells like GCTB |
Recent Evidence
Recent systematic reviews confirm the ongoing debate about cavity filling:
- A 2024 meta-analysis (PMID 39236154) of 1,454 patients found bone cement associated with lower recurrence compared to bone graft after intralesional curettage
- A 2024 systematic review (PMID 38711180) on surgical adjuvants confirms extended curettage + adjuvant significantly reduces local recurrence over simple curettage
- Heat treatment (radiofrequency ablation, cryotherapy) is being studied as an adjuvant; a 2023 systematic review (PMID 37726111) found promising results but noted heterogeneity in available data
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Campbell's Operative Orthopaedics 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.