Hyperparathyroidim in detail
Reading File
Finding Sources
Searching PubMed
"hyperparathyroidism"[MeSH Terms] AND ("management" OR "treatment")
Reading File
Reading File
Searching Images
hyperparathyroidism parathyroid gland pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from Harrison's and Robbins. Let me compile the complete answer:
Hyperparathyroidism — Comprehensive Overview
Definition
Hyperparathyroidism is a condition of excess parathyroid hormone (PTH) secretion, resulting in hypercalcemia and its systemic consequences. It is classified into three types: primary, secondary, and tertiary.
PTH Physiology — What Goes Wrong
PTH normally maintains calcium homeostasis through four key actions:
- Osteoclast activation — via increased RANKL expression on osteoblasts → bone resorption → calcium mobilization
- Renal calcium resorption — increased tubular reabsorption of Ca²⁺
- Phosphaturia — increased urinary phosphate excretion
- Vitamin D activation — stimulates renal 1α-hydroxylase → 1,25(OH)₂D synthesis → enhanced intestinal calcium absorption
The net result is elevated serum calcium, which under normal circumstances suppresses further PTH production. In hyperparathyroidism, this feedback is lost.
Classification
1. Primary Hyperparathyroidism (PHPT)
The most common cause of asymptomatic hypercalcemia in adults.
Causes & Pathology
| Cause | Frequency |
|---|---|
| Solitary parathyroid adenoma | ~85–90% |
| Multiglandular hyperplasia | ~10–15% |
| Parathyroid carcinoma | <1% |
| Double adenoma | Rare |
- Sporadic adenoma: Autonomous, clonal, single-gland enlargement. Associated with somatic mutations in MEN1 (chromosome 11q13) in ~15–20% of cases and overexpression of cyclin D1 (PRAD1/CCND1).
- Parathyroid hyperplasia: Multiglandular enlargement — the hallmark of MEN-1 (MEN1/MENIN tumor suppressor) and MEN-2A (Ret protooncogene gain-of-function).
- Parathyroid carcinoma: Associated with inactivating mutations in CDC73 (HRPT2 gene, chromosome 1q21-31), encoding parafibromin. Rb gene abnormalities also found. Importantly, carcinoma involves a different genetic pathway than benign adenoma — it does not evolve from adenoma through progressive mutations.
- HPT-JT syndrome: Familial hyperparathyroidism with jaw tumors — caused by germline CDC73 mutations.
Harrison's Principles of Internal Medicine 22E, 2025, p. 3318–3320
Epidemiology
- Peak incidence in middle adulthood (post-menopausal women particularly affected)
- Earlier onset in MEN-1 and MEN-2A (single germline mutation sufficient to trigger tumor)
2. Secondary Hyperparathyroidism
Caused by chronic hypocalcemia → compensatory parathyroid hyperplasia (reactive, not autonomous)
Primary driver: Chronic kidney disease (CKD)
Mechanisms in CKD:
- Inadequate 1,25(OH)₂D synthesis (loss of renal 1α-hydroxylase)
- Hyperphosphatemia → further lowers serum calcium
- Metabolic acidosis
- Calcium sensing receptor resistance
→ All four parathyroid glands enlarge diffusely (multiglandular hyperplasia, still responsive to medical therapy initially)
Robbins & Kumar Basic Pathology, p. 775
3. Tertiary Hyperparathyroidism
When long-standing, inadequately treated secondary HPT leads to autonomous clonal outgrowth of one or more previously hyperplastic parathyroid glands. PTH secretion becomes irreversible and unresponsive to medical therapy. Requires surgery.
Harrison's Principles of Internal Medicine 22E, p. 3325
Skeletal Pathology (Morphology)
Symptomatic, untreated PHPT produces three interrelated skeletal abnormalities:
1. Osteoporosis
- Generalized but most severe in phalanges, vertebrae, and proximal femur
- Predisposes to fractures and joint problems
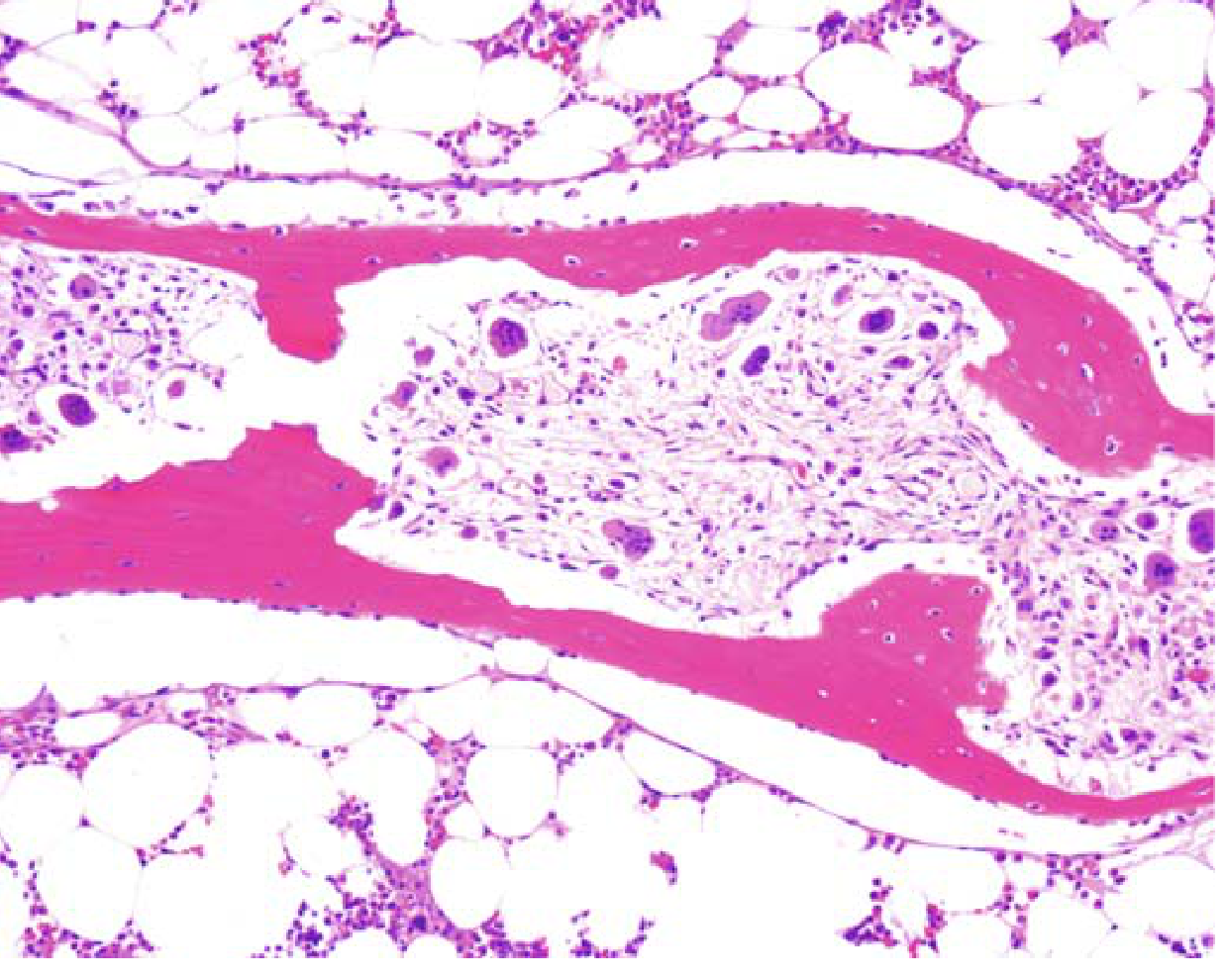
2. Dissecting Osteitis (Tunneling Resorption)
- Osteoclasts bore into and dissect along the length of trabeculae — "railroad track" appearance
- Marrow spaces replaced by fibrovascular tissue
3. Brown Tumors & Osteitis Fibrosa Cystica
- Microfractures → hemorrhage → macrophage infiltration + reparative fibrous tissue = brown tumor (named for its vascularity + hemosiderin content)
- Can undergo cystic degeneration
- Osteitis fibrosa cystica = the full triad of increased osteoclast activity + peritrabecular fibrosis + cystic brown tumors — now rarely encountered because HPT is diagnosed early
Histology — Dissecting Osteitis (Robbins):
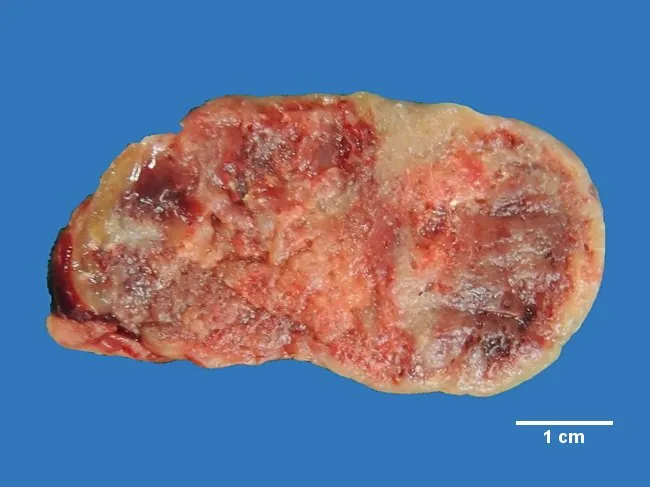
Gross pathology — parathyroid adenoma:
Clinical Features
Symptoms of Hypercalcemia (general)
The classic mnemonic: "Bones, Stones, Groans, and Psychic Moans"
| System | Manifestations |
|---|---|
| Skeletal | Bone pain, pathological fractures, deformity, arthropathy, brown tumors |
| Renal | Nephrolithiasis (calcium oxalate/phosphate stones), nephrocalcinosis, polyuria, nephrogenic DI |
| GI | Nausea, vomiting, anorexia, constipation, peptic ulcers (PTH stimulates gastrin) |
| Neuropsychiatric | Depression, fatigue, cognitive impairment, "psychic moans," weakness |
| Cardiovascular | Short QT interval on ECG, hypertension, arrhythmias (at Ca >3.2 mmol/L) |
| Soft tissue | Calcification in kidneys, skin, vessels, lungs, heart, stomach (band keratopathy in cornea) |
Symptoms are more common at calcium >2.9–3.0 mmol/L (11.6–12 mg/dL); severe manifestations at >3.2 mmol/L (12.8 mg/dL).
Asymptomatic PHPT (modern presentation)
Most cases are now detected incidentally on routine blood testing as asymptomatic hypercalcemia. Osteitis fibrosa cystica and brown tumors are now rare.
Diagnosis & Laboratory Findings
| Test | PHPT | Secondary HPT |
|---|---|---|
| Serum calcium | ↑ | ↓ or normal |
| PTH (immunometric assay) | ↑ (inappropriately elevated) | ↑↑ (appropriate response) |
| Serum phosphate | ↓ (phosphaturia) | ↑ (in CKD) |
| Urine calcium | ↑ | ↓ |
| Serum creatinine | May be ↑ | ↑ (in CKD) |
| Vitamin D (1,25(OH)₂D) | Often ↑ | ↓ |
| ALP | ↑ (if bone involvement) | Variable |
Key diagnostic tool: Immunometric PTH assay — distinguishes PTH-mediated hypercalcemia from non-PTH causes (malignancy, vitamin D toxicity, sarcoidosis, etc.)
Differentiating PHPT from malignancy-associated hypercalcemia:
- Asymptomatic hypercalcemia lasting >1 year → malignancy unlikely
- Malignancy-related hypercalcemia: PTHrP elevated (not PTH), malignancy usually clinically apparent
- Familial hypocalciuric hypercalcemia (FHH): benign mutation in calcium-sensing receptor — urine calcium/creatinine ratio <0.01 distinguishes it from PHPT
Harrison's Principles of Internal Medicine 22E, p. 3317
Indications for Surgery (PHPT)
Parathyroidectomy is the definitive therapy. Surgical indications (guidelines-based):
- Age <50 years
- Serum calcium >1 mg/dL above upper limit of normal
- Bone mineral density (BMD) T-score ≤ −2.5 at any site, or vertebral fracture
- Renal involvement: CrCl <60 mL/min, 24-hour urine Ca >400 mg/day, nephrolithiasis or nephrocalcinosis on imaging
- Patient preference for surgery over surveillance
Evidence favoring surgery is growing due to concerns about skeletal, cardiovascular, and neuropsychiatric disease even in mild PHPT. — Harrison's 22E, p. 3322
Surgical Approach
- Conventional neck exploration (general anesthesia) — standard
- Minimally invasive parathyroidectomy (local anesthesia, focused approach) — gaining traction
- Preoperative imaging: Neck ultrasound, ⁹⁹ᵐTc-sestamibi SPECT, C-11 choline PET/CT, 4D-CT
- Intraoperative PTH monitoring: Rapid PTH assay; >50% fall to normal confirms successful removal
- Familial/multiglandular disease: Subtotal parathyroidectomy or total PTX with forearm autotransplantation
Post-Operative Complications
- "Hungry bone" syndrome: Rapid calcium influx into demineralized bone → hypocalcemia; requires IV calcium replacement
- Transient hypoparathyroidism: Usually resolves in days–months
- Permanent hypoparathyroidism: Risk if PTH <15 pg/mL at 12–24 h post-op
- Hypomagnesemia can complicate recovery (impairs PTH secretion)
Medical Management of PHPT
For patients who decline surgery or are not surgical candidates:
| Drug | Effect | Notes |
|---|---|---|
| Bisphosphonates (alendronate) | Increase BMD | Do not lower serum calcium |
| Cinacalcet (calcimimetic) | Lowers PTH, reduces serum calcium | Does not improve BMD; also used in dialysis patients |
| Surveillance | Monitor serum Ca, creatinine, BMD annually | Acceptable if asymptomatic and meets no surgical criteria |
A Scandinavian RCT of parathyroidectomy vs. observation in mild PHPT showed no difference in morbidity or mortality at 10 years. — Harrison's 22E, p. 3323
Treatment of Secondary Hyperparathyroidism (CKD)
Goal: Control hyperphosphatemia, restore vitamin D, suppress PTH:
- Dietary phosphate restriction
- Phosphate binders: Calcium carbonate (avoid in hypercalcemia), sevelamer (preferred — no aluminum, no excess calcium loading)
- Active vitamin D: Calcitriol 0.25–2 μg/day or IV pulse calcitriol/paricalcitol
- Cinacalcet: Reduces PTH and calcium; effective in dialysis patients
- Parathyroidectomy for tertiary HPT (autonomous, unresponsive to medical therapy)
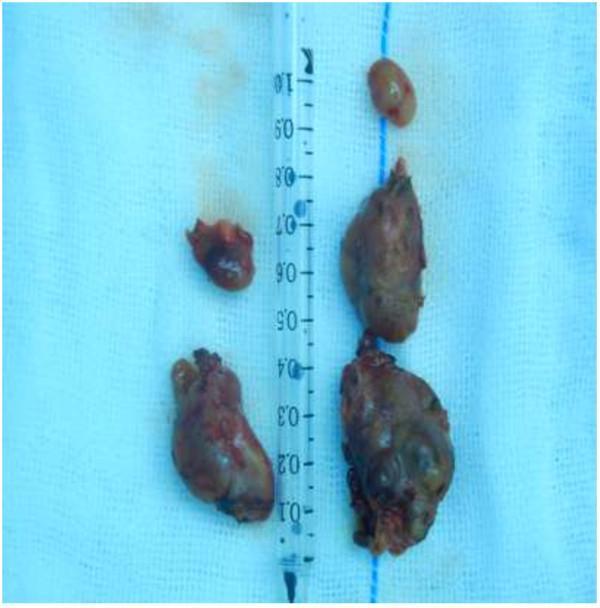
Gross pathology — secondary HPT (post-total parathyroidectomy specimens):
Special Situations
Lithium-Induced Hyperparathyroidism
- ~10% of lithium-treated patients develop hypercalcemia
- Lithium shifts the PTH secretion set-point to the right (requires higher Ca²⁺ to suppress PTH)
- Usually resolves on stopping lithium; cinacalcet effective
- Surgery only if HPT persists after lithium discontinuation
Post-Renal Transplant HPT
- Residual hyperparathyroidism is very common in the first post-transplant year
- Risk factors: degree of pre-transplant HPT, duration of dialysis
- Managed with paricalcitol or cinacalcet
- Surgery (subtotal PTX) if persistent hypercalcemia ≥12 mg/dL after >1 year, or calciphylaxis
MEN Syndromes
| Syndrome | HPT Features |
|---|---|
| MEN-1 | HPT is most common manifestation; multiglandular hyperplasia; earlier onset |
| MEN-2A | HPT occurs but less prominent than medullary thyroid ca + pheo |
| MEN-4 | Similar to MEN-1; CDKN1B mutation |
Summary Table: PHPT vs Secondary HPT vs Tertiary HPT
| Feature | Primary | Secondary | Tertiary |
|---|---|---|---|
| Cause | Adenoma/hyperplasia (autonomous) | CKD, vitamin D deficiency | Long-standing secondary HPT |
| Calcium | ↑ | ↓ or normal | ↑ |
| PTH | ↑ (inappropriate) | ↑↑ (appropriate) | ↑↑ (autonomous) |
| Phosphate | ↓ | ↑ | Variable |
| Glands | Single (usually) | All 4 enlarged | Autonomous clone |
| Treatment | Parathyroidectomy / medical | Calcitriol, phosphate binders, cinacalcet | Parathyroidectomy |
Recent Evidence (2024)
- A 2024 systematic review (PMID 38551756) evaluated quality of clinical practice guidelines for PHPT management — evidence base continues to be refined.
- A 2024 meta-analysis (PMID 38583772) found parathyroidectomy superior to medical treatments for secondary HPT in dialysis patients in reducing PTH, calcium, and phosphate.
- A 2024 meta-analysis (PMID 38536478) showed calcimimetics reduce fracture risk in dialysis patients with secondary HPT.
Sources: Robbins & Kumar Basic Pathology (9780323790185), pp. 763–775 | Harrison's Principles of Internal Medicine 22E (9781265977061), pp. 3317–3325 | Brenner and Rector's The Kidney (9780323532655)
This is a shared conversation. Sign in to Orris to start your own chat.