Fibrous dysplasia
Reading File
Finding Sources
Searching PubMed
"fibrous dysplasia"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have enough comprehensive information now. Let me compile the full answer.
Fibrous Dysplasia
Definition
Fibrous dysplasia (FD) is a benign skeletal lesion arising from a localized developmental arrest in which normal bone and marrow are replaced by fibro-osseous tissue - disorganized, inadequately mineralized woven bone embedded in a cellular fibrous stroma. All skeletal components are present but fail to mature into normal lamellar bone. It accounts for approximately 7% of benign bone tumors.
- Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis
All forms result from somatic gain-of-function mutations in GNAS1 (encoding the stimulatory Gs-protein alpha subunit), acquired during fetal development. The same gene is mutated in pituitary neuroendocrine tumors.
-
The mutation causes constitutive activation of Gs-protein, elevating intracellular cAMP
-
Elevated cAMP alters Wnt signaling, promoting cellular proliferation and inhibiting osteoblast differentiation
-
The phenotype depends on:
- The stage of embryogenesis when the mutation occurs
- The proportion and location of mesenchymal cells carrying the mutation
-
Very early embryonic mutation → McCune-Albright syndrome; later mutation in a single osteoblast precursor → monostotic FD
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1102
Forms / Classification
| Form | Description |
|---|---|
| Monostotic | Single bone involved (~80% of cases) |
| Polyostotic | Multiple bones involved |
| McCune-Albright syndrome | Polyostotic FD + café-au-lait spots + endocrine abnormalities (especially precocious puberty in girls) |
| Mazabraud syndrome | FD (usually polyostotic) + soft-tissue myxomas |
- Grainger & Allison's Diagnostic Radiology
Epidemiology & Sites
-
No gender predilection
-
75% of cases present before age 30; ~25% diagnosed after age 30
-
Monostotic - most common sites: ribs (28%), proximal femur (23%), craniofacial bones (20%)
-
Polyostotic - femur, tibia, and pelvis most often affected; may involve up to 75% of the skeleton
-
Can affect epiphysis, metaphysis, or diaphysis; metadiaphyseal region is typical in long bones
-
Grainger & Allison's Diagnostic Radiology; Rheumatology 2-Volume Set
Morphology
Gross: Tan-white, gritty intramedullary lesional tissue; may cause cortical expansion, thinning, and bowing.
Microscopy (key features):
-
Curvilinear ("C"- or "S"-shaped) trabeculae of woven bone - often described as resembling "Chinese letters" or letters of the alphabet, arranged around vessels
-
No osteoblastic rimming (absent rim of osteoblasts around trabeculae - a hallmark distinguishing FD from ossifying fibroma)
-
Moderately cellular fibroblastic stroma with loose collagen
-
Cystic degeneration, hemorrhage, and foamy macrophages may be present
-
No periosteal reaction (unless fracture is present)
-
Robbins & Kumar Basic Pathology; Rheumatology 2-Volume Set
Radiological Features
Plain X-ray:
- "Ground-glass" appearance - most characteristic; caused by mineralized woven bone spicules within fibrous tissue
- Elongated lesion causing symmetric cortical thinning and expansion - classic "long lesion in a long bone"
- Geographic lytic lesion; thick sclerotic margin ("rind sign") is characteristic
- Purely lytic variants reflect extensive cystic degeneration
- Periosteal reaction is absent unless fracture has occurred

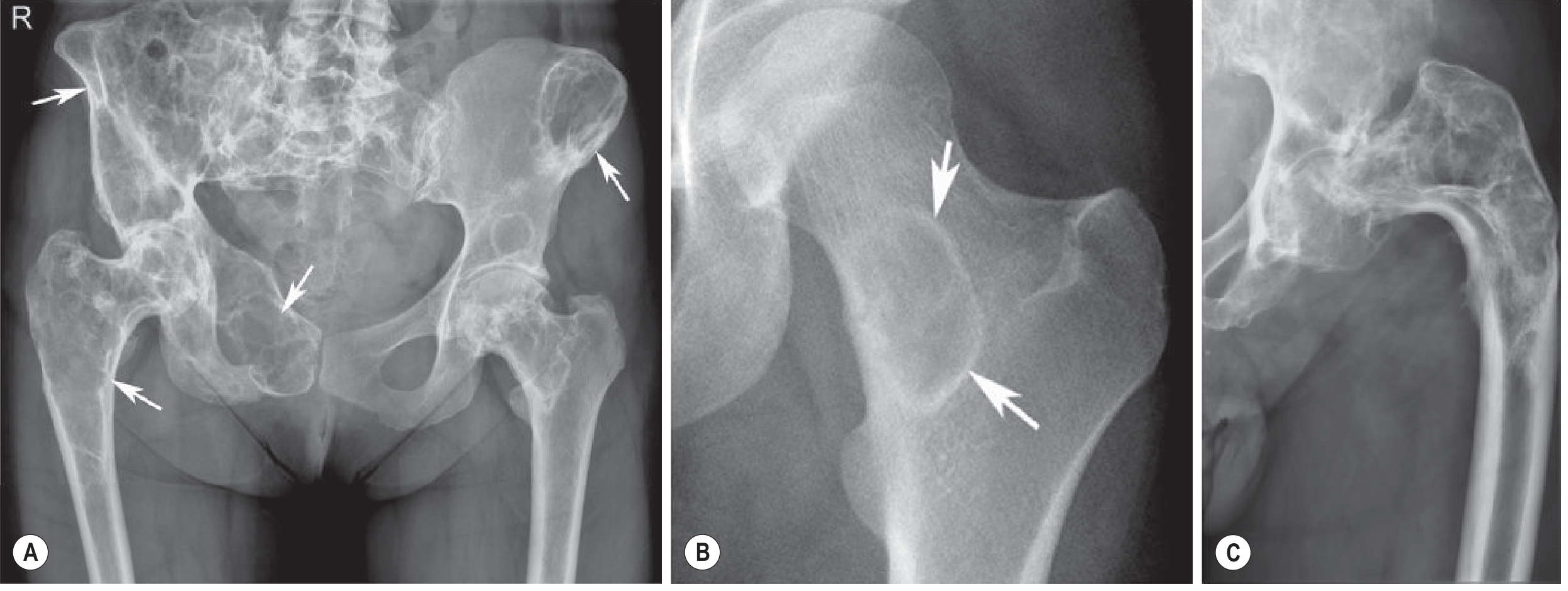
Polyostotic FD - pelvis and hip:
Clinical Features
- Often asymptomatic - discovered incidentally on X-ray
- May present with: pain, pathologic fracture, and bone deformity
- Monostotic FD frequently stops enlarging at growth plate closure
- Polyostotic FD with weight-bearing bone involvement leads to deformity from repeated fractures - the classic "shepherd's crook" deformity of the proximal femur
- In severe polyostotic disease, FD may produce FGF-23 causing secondary osteomalacia
- Malignant transformation is extremely rare but recognized (with or without prior radiotherapy)
Syndromes Summary
McCune-Albright Syndrome
- Polyostotic FD (typically unilateral) + ipsilateral café-au-lait spots + endocrine dysfunction
- Most common endocrine abnormality: precocious puberty (girls)
- Other endocrine manifestations: hyperthyroidism, Cushing syndrome, acromegaly
- Usually symptomatic before age 10
- Not inherited - mosaic activating GNAS1 mutation acquired in early embryogenesis
Mazabraud Syndrome
- FD (usually polyostotic) + intramuscular myxomas
Treatment
-
Asymptomatic monostotic FD: observation; often stabilizes after skeletal maturity
-
Symptomatic lesions: curettage (recurrence is common)
-
Extensive polyostotic disease: pain management + surgery + bone-strengthening measures
-
Bisphosphonates (e.g., pamidronate, zoledronic acid): used for pain control and to reduce fracture risk, particularly in polyostotic and McCune-Albright cases
-
Surgical stabilization for impending or actual pathologic fractures; intramedullary rodding for shepherd's crook deformity
-
Rheumatology 2-Volume Set; Campbell's Operative Orthopaedics 15th Ed 2026
Key Summary Table
| Feature | Detail |
|---|---|
| Mutation | GNAS1 gain-of-function (somatic, mosaic) |
| Pathology | Woven bone trabeculae, no osteoblast rimming, fibrous stroma |
| X-ray | Ground-glass, rind sign, long lesion in long bone |
| Hallmark deformity | Shepherd's crook (proximal femur) |
| Associated syndromes | McCune-Albright, Mazabraud |
| Malignant potential | Extremely rare |
| Treatment | Curettage, bisphosphonates, surgical stabilization |
This is a shared conversation. Sign in to Orris to start your own chat.