Tomorrow is my dentistry exam give me 10 marks answer of each question I will send one by one
Anatomy and physiology of teeth enamel dentin pulp periodontal structures
Anatomy and Physiology of Teeth: Enamel, Dentin, Pulp, and Periodontal Structures
INTRODUCTION
1. ENAMEL
Anatomy
- Enamel covers the entire crown of the tooth.
- It is the hardest substance in the human body.
- Composed of ~96-97% inorganic material (calcium hydroxyapatite - Ca₁₀(PO₄)₆(OH)₂) and only 2-3% organic material (mainly amelogenin protein) with trace water.
- Average thickness: ~2 mm at the cusp tips.
Microstructure
- Made up of enamel rods (prisms), each ~4-8 μm in diameter, running from the dentinoenamel junction (DEJ) to the outer surface.
- Each rod has a keyhole shape in cross-section - a "head" (crystals parallel to rod axis) and a "tail" (crystals more oblique).
- Rods are tightly interlocked, giving enamel its resistance to masticatory pressures.
- Contour lines of Retzius = striations on rods representing rhythmic growth; the neonatal line marks the prenatal-postnatal transition in deciduous teeth.
Physiology
- Acellular - contains no cells, vessels, or nerves after formation. Cannot regenerate.
- Produced by ameloblasts during tooth development (via Tomes' process) - these cells are lost after eruption.
- Fluoride ions can replace OH⁻ in hydroxyapatite, forming fluorapatite, which is more resistant to acid dissolution - rationale for fluoride in toothpaste.
- Protects underlying dentin and pulp from mechanical and thermal insults.
2. DENTIN
Anatomy
- Forms the bulk of the tooth, extending from the DEJ to the pulp cavity.
- Covered by enamel in the crown and by cementum in the root.
- Yellowish in color; slightly softer than enamel but harder than bone.
Microstructure
- Contains dentinal tubules (dental canaliculi) - microscopic channels running radially from the pulp to the DEJ, giving dentin its characteristic radial striping.
- Each tubule contains an odontoblastic process (Tomes' fiber) - a cytoplasmic extension of odontoblast cells lining the pulp.
- Ground substance: organic matrix (collagen fibrils) + calcium salts (hydroxyapatite).
- No blood vessels within dentin itself.
Types of Dentin
| Type | Features |
|---|---|
| Primary dentin | Formed before tooth eruption |
| Secondary dentin | Formed slowly throughout life after eruption |
| Tertiary (reparative) dentin | Formed in response to injury/caries |
| Predentin | Unmineralized layer at the inner pulp surface |
Physiology
- Odontoblasts (lining the pulp surface) continuously synthesize new predentin even after eruption, depositing new dentin inward throughout life.
- Sensitivity - unmyelinated type C nerve fibers extend into the dentinal tubules; stimuli (cold, heat, osmotic) transmitted via hydrodynamic movement of dentinal fluid (Brannstrom's hydrodynamic theory).
3. DENTAL PULP
Anatomy
- Soft connective tissue filling the pulp cavity, which includes:
- Pulp chamber (in the crown)
- Root canal (in the root)
- Apical foramen (opening at root tip through which nerves and vessels enter)
Histology/Microstructure
- Loose connective tissue, well vascularized.
- Odontoblasts arranged in a palisade (outer layer) - specialized cells that form dentin.
- Inner layers: cell-rich zone (fibroblasts, defense cells) and cell-free zone (Weil's zone).
- Nerves: both myelinated (A-delta fibers - sharp pain) and unmyelinated (C fibers - dull, poorly localized pain). Pain of pulpitis is often poorly localized due to predominance of C fibers.
- Blood supply: enters via apical foramen (branches of superior and inferior alveolar arteries).
Physiology
- Dentinogenic function: odontoblasts produce dentin throughout life.
- Nutritive function: maintains vitality of dentin.
- Sensory function: pain transmission via nerve fibers in dentinal tubules.
- Defensive function: immune cells (macrophages, lymphocytes) protect against microbial invasion; tertiary dentin formation in response to injury.
- Inflammatory response: pulpitis (inflammation) occurs due to caries. Because pulp is enclosed in a rigid chamber, inflammation causes pressure buildup → severe pain.
4. PERIODONTAL STRUCTURES (PERIODONTIUM)
A. Cementum
- Covers the dentin of the root.
- Resembles woven bone but is avascular.
- Produced by cementoblasts.
- Thickest near the root apex.
- Contains cementocytes in lacunae (near the surface) with processes in canaliculi.
- Collagen fibers (Sharpey fibers) from the PDL are anchored into cementum, binding the tooth to the socket.
- Meets enamel at the cementoenamel junction (CEJ) or neck of the tooth.
B. Periodontal Ligament (PDL)
- Dense fibrous connective tissue between cementum and alveolar bone.
- Thickness: 150-350 μm (decreases with age).
- Contains Sharpey fibers (principal collagen fiber bundles) - anchored into cementum and alveolar bone.
| Group | Orientation | Function |
|---|---|---|
| Alveolar crest fibers | Oblique downward | Resist lateral tooth movement |
| Horizontal fibers | Right angle to root | Resist tipping forces |
| Oblique fibers | Most numerous; oblique upward | Resist vertical/axial forces |
| Apical fibers | Radiate from apex | Resist extrusion |
| Interradicular fibers | Multi-rooted teeth | Resist vertical/lateral forces |
- Supportive: suspends tooth in socket; permits slight mobility.
- Sensory: highly innervated - proprioceptive sensations guide chewing force.
- Nutritive: blood vessels supply cementum and alveolar bone.
- Formative/Remodeling: contains cementoblasts, osteoblasts, fibroblasts.
- Eruptive: plays a role in tooth eruption and positional maintenance.
C. Alveolar Bone
- The bone of the jaw that forms the tooth sockets (alveoli).
- Has two layers: cortical plate (outer) + cancellous bone (inner) + alveolar bone proper (lamina dura - socket wall).
- Unlike typical lamellar bone, alveolar bone proper has osteoblasts and osteocytes engaged in continuous remodeling.
- Dependent on tooth presence - resorbs after tooth extraction.
D. Gingiva
- Oral mucosa covering alveolar bone and tooth necks.
- Junctional epithelium: specialized epithelium attaching to enamel/cementum at the CEJ via hemidesmosomes and a thick basal lamina.
- Gingival sulcus: shallow groove between tooth surface and gingival margin (normal depth 1-3 mm).
- Deepening of sulcus → periodontal pockets → bacterial colonization → periodontitis.
SUMMARY TABLE
| Structure | Composition | Key Cells | Special Feature |
|---|---|---|---|
| Enamel | 96% hydroxyapatite | Ameloblasts (lost post-eruption) | Hardest body substance; acellular |
| Dentin | 70% hydroxyapatite + collagen | Odontoblasts | Dentinal tubules; sensitive |
| Pulp | Loose CT, vessels, nerves | Odontoblasts, fibroblasts | Enclosed; pulpitis = pressure pain |
| Cementum | Bone-like; avascular | Cementoblasts | Anchors Sharpey fibers |
| PDL | Collagen fibers | Fibroblasts, cementoblasts | Proprioception; 150-350 μm thick |
| Alveolar bone | Lamellar bone | Osteoblasts | Resorbs without teeth |
| Gingiva | Stratified squamous epithelium | - | Junctional epithelium at CEJ |
- Enamel = hardest, acellular, cannot regenerate - ameloblasts lost after eruption.
- Dentin sensitivity = hydrodynamic theory (Brannstrom).
- Pulp pain = poorly localized (C fibers predominate).
- PDL = 5 principal fiber groups; oblique group is the most numerous.
- Periodontitis = deepened sulcus → bacterial pockets → bone loss.
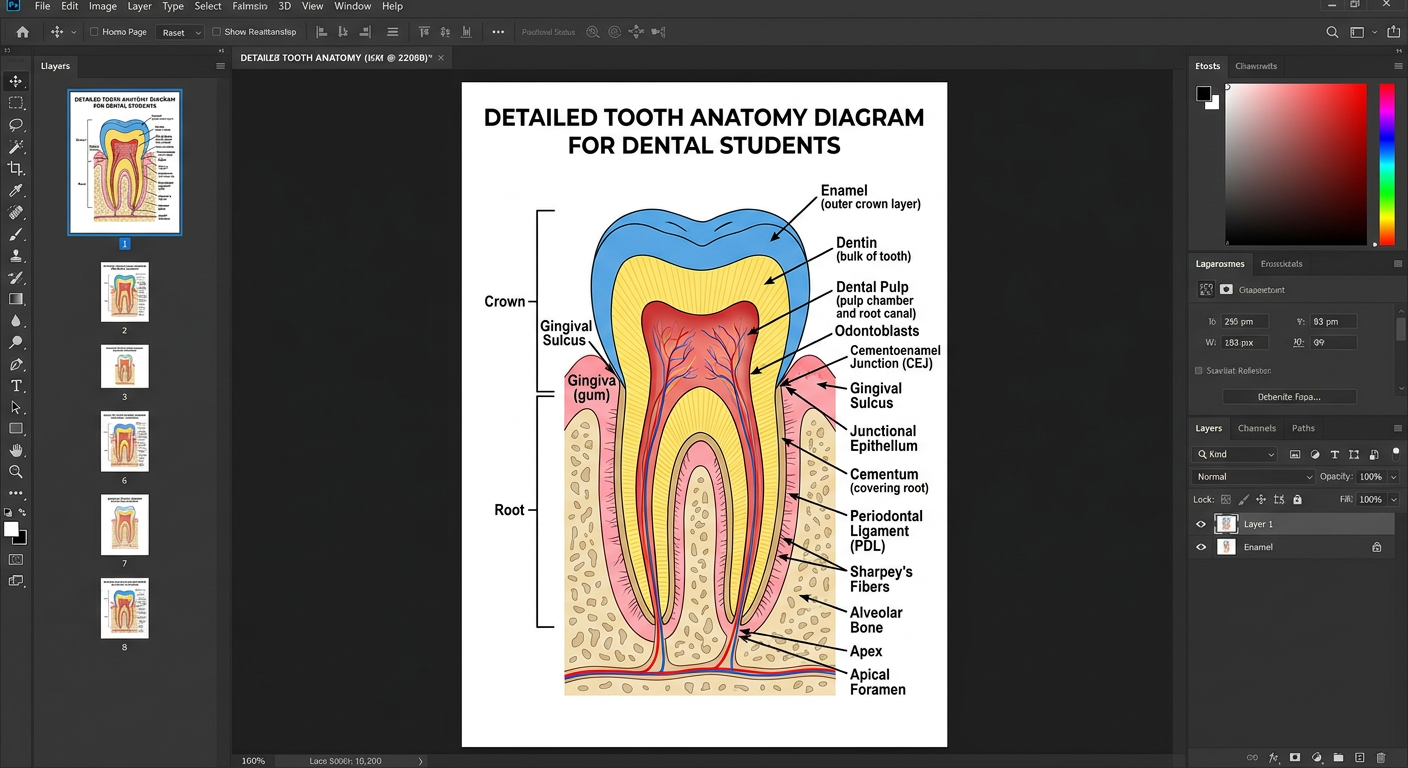
Make a labeled tooth anatomy diagram poster
Detailed labeled tooth anatomy diagram poster for dental students. Large cross-section of a tooth showing all anatomical structures with clear labels and arrows. Labels include: Enamel (outer crown layer), Dentin (bulk of tooth), Dental Pulp (pulp chamber and root canal), Cementum (covering root), Periodontal Ligament (PDL), Alveolar Bone, Gingiva (gum), Crown, Root, Apex, Apical Foramen, Dentinoenamel Junction (DEJ), Cementoenamel Junction (CEJ), Gingival Sulcus, Junctional Epithelium, Odontoblasts, Sharpey's Fibers, Blood vessels and nerves in pulp. Clean medical illustration style with white background, color-coded layers (blue for enamel, yellow for dentin, red for pulp, tan for cementum, pink for gingiva, beige for alveolar bone), professional dental textbook quality, clear annotation lines.
Jaw tumours
Jaw Tumours - 10 Marks
INTRODUCTION & CLASSIFICATION
Classification Overview
JAW TUMOURS
├── ODONTOGENIC
│ ├── Cysts (inflammatory & developmental)
│ └── Tumours (benign & malignant)
└── NON-ODONTOGENIC
├── Bone tumours (osteoma, osteosarcoma)
├── Fibro-osseous lesions
└── Metastatic tumours
A. ODONTOGENIC CYSTS
TABLE: Classification of Odontogenic Cysts
| Type | Sub-type | Key Feature |
|---|---|---|
| Inflammatory | Radicular (periapical) cyst | Most common; at tooth apex; due to pulpitis/caries |
| Paradental cyst | Adjacent to partially erupted tooth | |
| Developmental | Dentigerous cyst | Around crown of unerupted tooth |
| Odontogenic keratocyst (OKC) | Aggressive; high recurrence | |
| Gingival cyst | In gingiva | |
| Lateral periodontal cyst | Lateral to tooth root | |
| Calcifying odontogenic cyst | Also called Gorlin cyst |
1. Radicular (Periapical) Cyst
- Most common jaw cyst.
- Arises from chronic pulpitis (usually due to caries) → pulp necrosis → inflammation exits at apex → granulation tissue → epithelialization → cyst.
- Lined by non-keratinized stratified squamous epithelium.
- X-ray: Periapical radiolucency.
- Treatment: Root canal treatment or tooth extraction + curettage.
2. Dentigerous Cyst
- Most common developmental odontogenic cyst; commonest jaw cyst in children.
- Surrounds the crown of an unerupted tooth (most often mandibular 3rd molar or maxillary canine).
- Cyst wall attaches at the cementoenamel junction.
- X-ray: Unilocular radiolucency around crown of unerupted tooth. Follicular space >4mm is diagnostic.
- Treatment: Marsupialization or enucleation with bone grafting for large lesions.
3. Odontogenic Keratocyst (OKC)
- Now termed keratocystic odontogenic tumour by WHO.
- Characteristic parakeratinized stratified squamous epithelium lining.
- Locally aggressive - high recurrence (up to 60%) if inadequately removed.
- Multiple OKCs → suspect Gorlin syndrome (Nevoid Basal Cell Carcinoma Syndrome - PTCH gene mutation).
- X-ray: Multilocular or unilocular radiolucency, often in mandibular ramus.
- Treatment: Excision; careful margins needed due to high recurrence.
B. ODONTOGENIC TUMOURS
TABLE: WHO Classification of Odontogenic Tumours (Key Ones)
| Origin | Benign | Malignant |
|---|---|---|
| Epithelium only | Ameloblastoma, Adenomatoid odontogenic tumour (AOT), Calcifying epithelial odontogenic tumour (CEOT/Pindborg tumour) | Ameloblastic carcinoma, Primary intraosseous SCC |
| Mesenchyme only | Odontogenic fibroma, Odontogenic myxoma, Cementoblastoma | - |
| Epithelium + Mesenchyme | Odontoma (compound/complex), Ameloblastic fibroma | Ameloblastic fibrosarcoma |
1. AMELOBLASTOMA (Most Important - Most Common Odontogenic Tumour)
- Benign but locally aggressive neoplasm arising from odontogenic epithelium (remnants of enamel organ / dental lamina).
- Does not show ectomesenchymal differentiation.
- Conventional (Solid/Multicystic) - most common
- Unicystic - less aggressive; 10-20% recurrence
- Peripheral (Extraosseous) - on gingiva, low recurrence
- Metastasizing - rare, malignant behavior
- Usually >20 years of age.
- 85% in mandible - most commonly molar/ramus region.
- Slow, painless expansion of jaw.
- MAPK pathway mutation (BRAF V600E) in ~90% of lesions.
- Multilocular "soap bubble" or "honeycomb" radiolucency.
- Root resorption + cortical bone expansion.
- Well-demarcated.
- Follicular pattern: Islands of epithelium; peripheral columnar cells with reversed nuclear polarization + central stellate reticulum-like cells resembling enamel organ.
- Plexiform pattern: Epithelial strands in anastomosing network.
- Other subtypes: acanthomatous, granular cell, desmoplastic, basal cell.
- Classic description: "Piano key" appearance of columnar cells.
- Wide surgical resection with 1 cm margin beyond radiographic extent.
- Recurrent cases with confirmed BRAF mutation: BRAF-targeted therapy (e.g., dabrafenib).
- Prognosis: Good with surveillance; high recurrence if marginally excised.
2. ODONTOMA (Most Common Odontogenic Tumour Overall)
- Arises from both epithelium and mesenchyme; likely a hamartoma not true neoplasm.
- Contains enamel, dentin, cementum, and pulp in disorganized (complex) or recognizable tooth-like structures (compound).
| Type | Appearance | Location |
|---|---|---|
| Compound | Multiple small tooth-like structures (denticles) | Anterior maxilla |
| Complex | Disorganized mass of dental tissue | Posterior mandible |
- X-ray: Radiopaque mass.
- Treatment: Simple enucleation; low recurrence; excellent prognosis.
3. ODONTOGENIC MYXOMA
- Arises from odontogenic mesenchyme (dental papilla/follicle).
- Slow-growing, locally invasive, no capsule.
- X-ray: Multilocular radiolucency with "tennis racket" or "soap bubble" pattern.
- Histology: Stellate cells in loose myxoid stroma.
- Treatment: Resection; 25% recurrence.
4. ADENOMATOID ODONTOGENIC TUMOUR (AOT)
- Called "2/3 tumour": 2/3 in females, 2/3 in maxilla, 2/3 associated with impacted canine.
- Well-encapsulated; low recurrence.
- Histology: Duct-like structures + calcifications.
- Treatment: Simple enucleation.
5. CALCIFYING EPITHELIAL ODONTOGENIC TUMOUR (CEOT/Pindborg Tumour)
- Rare; locally invasive.
- Histology: Polyhedral epithelial cells + amyloid deposits + Liesegang ring calcifications ("driven snow" appearance on X-ray).
C. NON-ODONTOGENIC TUMOURS OF THE JAW
| Tumour | Features |
|---|---|
| Osteoma | Benign; dense radiopaque. Multiple = Gardner syndrome |
| Central Giant Cell Granuloma | Benign, aggressive; radiolucency; F>M; mandible |
| Osteosarcoma | Malignant; "sunray" pattern on X-ray; aggressive |
| Fibrous Dysplasia | Ground-glass appearance; monostotic/polyostotic |
| Burkitt's Lymphoma | Jaw mass in children; EBV-associated; "floating teeth" sign |
| Metastatic deposits | Breast, lung, prostate, thyroid - via haematogenous spread |
SUMMARY TABLE FOR RAPID REVISION
| Tumour | Age | Site | X-Ray | Key Histology | Treatment |
|---|---|---|---|---|---|
| Radicular cyst | Any | Apex of root | Periapical radiolucency | Non-keratinized epithelium | RCT / extraction |
| Dentigerous cyst | Children/Young | Around unerupted crown | Unilocular around crown | Thin flat epithelium | Enucleation |
| OKC | 20-40 | Mandible ramus | Multilocular | Parakeratinized epithelium | Wide excision |
| Ameloblastoma | >20 | Mandible (85%) | Soap-bubble multilocular | Reversed polarization, stellate reticulum | Resection 1cm margin |
| Odontoma | Young | Compound-anterior, Complex-posterior | Radiopaque | Enamel + dentin + cementum | Enucleation |
| Odontogenic Myxoma | 20-40 | Mandible | Tennis racket multilocular | Stellate cells, myxoid stroma | Resection |
| AOT | Young female | Maxillary canine | Unilocular | Duct-like structures | Enucleation |
KEY EXAM POINTS
- Most common jaw cyst = Radicular (periapical) cyst.
- Most common odontogenic tumour = Odontoma (hamartoma).
- Most clinically significant odontogenic tumour = Ameloblastoma.
- Ameloblastoma histology = Reversed nuclear polarization + stellate reticulum = "piano keys."
- OKC + multiple cysts = Gorlin syndrome (PTCH gene mutation).
- AOT mnemonic = "2/3 rule" (2/3 female, 2/3 maxilla, 2/3 canine).
- Burkitt's lymphoma in jaw = EBV, "floating teeth" on X-ray, in children.
- BRAF V600E mutation in ameloblastoma = target for recurrent disease therapy.
Pathogenesis diagnosis and treatment.
Pathogenesis, Diagnosis and Treatment of Jaw Tumours - 10 Marks
I. PATHOGENESIS
A. Odontogenic Remnants - The Core Concept
| Remnant | Origin | Tumour/Cyst Derived |
|---|---|---|
| Rests of Malassez | Hertwig's epithelial root sheath | Radicular cyst, Cementoblastoma |
| Reduced enamel epithelium | Enamel organ | Dentigerous cyst |
| Dental lamina rests (Rests of Serres) | Dental lamina | Odontogenic keratocyst, Ameloblastoma |
| Cell rests of Serre | Oral epithelium | Gingival cyst |
B. Pathogenesis of Specific Tumours
1. Radicular (Periapical) Cyst
Dental caries → Pulpitis → Pulp necrosis
↓
Bacteria/toxins exit apical foramen
↓
Periapical inflammation → Periapical granuloma
↓
Stimulation of Rests of Malassez (epithelial cell rests in PDL)
↓
Epithelial proliferation + Cystic degeneration
↓
Radicular cyst formation
- Epithelium proliferates under influence of inflammatory cytokines (IL-1, IL-6, TNF-α, EGF).
- Central liquefaction due to accumulation of cellular debris, cholesterol crystals, and increased osmotic pressure → cyst expansion.
2. Dentigerous Cyst
- Arises from accumulation of fluid between the crown of an unerupted tooth and the reduced enamel epithelium.
- The enlarged follicular space >4mm from crown surface confirms cyst formation.
- Risk: Can transform into ameloblastoma or rarely squamous cell carcinoma if left untreated.
3. Odontogenic Keratocyst (OKC)
- Arises from dental lamina rests or from basal cells of overlying oral epithelium.
- Has intrinsic growth potential - proliferates independently (not merely from fluid pressure like other cysts).
- Associated with PTCH1 (Patched) gene mutation - a tumour suppressor gene in the Hedgehog signalling pathway.
- Multiple OKCs = Gorlin-Goltz Syndrome (PTCH germline mutation + basal cell naevi + calcification of falx cerebri).
- High recurrence (up to 60%) because daughter cysts ("satellite cysts") remain in bone after incomplete removal.
4. Ameloblastoma
- Arises from:
- Remnants of dental lamina
- Reduced enamel epithelium
- Lining of dentigerous cysts
- Basal cells of oral mucosa
- Molecular pathogenesis: Mutations in the MAPK signalling pathway found in ~90% of all lesions:
- BRAF V600E mutation - most common
- Less common: RAS mutations (NRAS, KRAS), FGFR2 mutations, SMO mutations
- These mutations → uncontrolled cell proliferation + local bone invasion
- Growth mechanism: Invades medullary (cancellous) bone trabeculae - extends histologically beyond the radiographic margin, explaining high recurrence.
- Tumour does not show ectomesenchymal differentiation (distinguishes it from ameloblastic fibroma).
5. Odontogenic Myxoma
- Arises from odontogenic ectomesenchyme (dental papilla or follicular mesenchyme).
- Stellate cells embedded in loose myxoid stroma (rich in glycosaminoglycans).
- No true capsule → locally invasive growth.
6. Non-Odontogenic Mechanisms
- Fibrous dysplasia: GNAS gene mutation (Gs-alpha protein) → abnormal osteoblast differentiation → replacement of normal bone by fibrous tissue + disorganized woven bone.
- Central Giant Cell Granuloma: Reactive/neoplastic; osteoclast-like giant cells driven by RANKL signalling; aggressive form shows SH3BP2 or RAS mutations.
- Osteosarcoma of jaw: Radiation exposure, Paget's disease, fibrous dysplasia malignant transformation, or de novo.
II. DIAGNOSIS
Step 1 - Clinical Assessment
- Age, gender (AOT: young females; ameloblastoma: >20 years)
- Duration and rate of growth
- Pain (usually absent in benign tumours; present in infections/malignancy)
- Loosening of teeth, paraesthesia (numbness = aggressive/malignant behaviour)
- Family history (Gorlin syndrome)
- Site, size, shape of swelling
- Consistency: bony hard (osteoma), rubbery (myxoma), soft (cyst)
- Expansion: buccal/lingual cortical plate
- Egg-shell crackling (beaten copper appearance)
- Tooth mobility, sensibility testing
- Regional lymphadenopathy (malignancy)
- Skin: basal cell naevi (Gorlin syndrome)
Step 2 - Radiological Investigations
| Investigation | Finding | Use |
|---|---|---|
| Intraoral periapical X-ray (IOPA) | Periapical radiolucency (radicular cyst); root resorption | First-line for single tooth/local lesion |
| Orthopantomogram (OPG/Panoramic) | Full jaw view; multilocular radiolucency (ameloblastoma); extent of lesion | Standard for all jaw lesions |
| Occlusal X-ray | Buccal/lingual expansion | Supplementary |
| CT Scan (CBCT or MDCT) | 3D bone expansion, cortical destruction, root resorption, extent | Best for pre-surgical planning |
| MRI | Soft tissue extension, nerve involvement, recurrence | Malignancy/myxoma/large lesions |
| Bone scan | Multicentricity, metastases | Rare; malignant cases |
| Lesion | X-ray Pattern |
|---|---|
| Radicular cyst | Periapical unilocular radiolucency |
| Dentigerous cyst | Unilocular around unerupted crown |
| OKC | Multilocular ± scalloped margins in ramus |
| Ameloblastoma | "Soap bubble"/"Honeycomb" multilocular radiolucency; root resorption |
| Odontoma | Radiopaque mass (calcified structures) |
| Odontogenic myxoma | "Tennis racket"/"Soap bubble" multilocular |
| Osteosarcoma | "Sunray" pattern + periosteal reaction |
| Fibrous dysplasia | "Ground glass" appearance |
Step 3 - Laboratory / Special Investigations
- Aspiration of cyst: Straw-coloured fluid (dentigerous/radicular cyst); cheesy white material (OKC - keratin); blood (aneurysmal bone cyst/vascular lesion).
- Incisional biopsy: Mandatory before definitive treatment; confirms histological type.
- Fine Needle Aspiration Cytology (FNAC): For associated soft tissue masses.
- Immunohistochemistry (IHC): BRAF V600E staining in ameloblastoma.
- Molecular testing: MAPK/BRAF mutation analysis for recurrent ameloblastoma (guides targeted therapy).
- Blood tests: CBC, LFT, RFT; serum ALP elevated in fibrous dysplasia/Paget's; serum Ca/PO4.
Histopathological Diagnosis (Definitive)
| Tumour | Key Histological Feature |
|---|---|
| Radicular cyst | Non-keratinized stratified squamous epithelium; cholesterol clefts; Rushton bodies |
| OKC | Parakeratinized corrugated epithelium; palisaded basal layer |
| Ameloblastoma | Reversed nuclear polarization of columnar cells; stellate reticulum |
| Odontoma | Enamel + dentin + cementum + pulp |
| Odontogenic myxoma | Stellate cells in loose myxoid stroma |
| AOT | Duct-like rosettes + calcifications |
| CEOT (Pindborg) | Polyhedral cells + amyloid deposits + Liesegang calcifications |
| Osteosarcoma | Malignant spindle cells + osteoid production |
III. TREATMENT
A. Odontogenic Cysts
| Cyst | Treatment | Notes |
|---|---|---|
| Radicular cyst | Root canal treatment (RCT) + apicectomy OR tooth extraction + curettage | Eliminate source of infection first |
| Dentigerous cyst | Small: Enucleation + removal of associated tooth; Large: Marsupialization first, then enucleation | Bone grafting for large defects |
| OKC | Wide excision with peripheral ostectomy; chemical cauterization (Carnoy's solution) | High recurrence (60%) demands aggressive surgery |
B. Benign Odontogenic Tumours
1. Ameloblastoma
- Gold standard: En bloc resection with 1 cm margin of normal bone beyond radiographic extent.
- Tumour infiltrates cancellous bone trabeculae - extends beyond what X-ray shows.
- Simple enucleation alone = NOT acceptable (high recurrence ~22% even with en bloc; much higher with curettage alone).
- Mandible: Segmental mandibulectomy ± marginal resection; lingual/buccal cortical plates sacrificed.
- Maxilla: More aggressive surgery due to proximity to vital structures (orbit, skull base).
- Reconstruction: Immediate or delayed reconstruction with:
- Titanium plates + iliac crest bone graft
- Free fibula flap (gold standard for large mandibular defects)
- Recurrent ameloblastoma with BRAF V600E mutation: BRAF inhibitor dabrafenib ± MEK inhibitor trametinib.
- Unicystic type: Less aggressive; enucleation with clear margins; 10-20% recurrence.
- Peripheral type: Local excision; very low recurrence.
- Surveillance: Regular clinical + OPG/CT follow-up (recurrence can appear years later).
2. Odontoma
- Simple enucleation - curative; extremely low recurrence; excellent prognosis.
3. Odontogenic Myxoma
- Resection (locally aggressive, no capsule); 25% recurrence; close follow-up.
4. AOT
- Simple enucleation; rarely recurs; excellent prognosis.
5. OKC (Keratocystic Odontogenic Tumour)
- Enucleation + Carnoy's solution (chemical fixation of satellite cysts) + peripheral ostectomy.
- Some surgeons prefer resection for large/recurrent lesions.
- Gorlin syndrome patients: lifelong surveillance.
C. Malignant Odontogenic Tumours / Jaw Malignancies
| Tumour | Treatment |
|---|---|
| Ameloblastic carcinoma | Wide resection + neck dissection + adjuvant radiotherapy |
| Primary intraosseous SCC | Resection + neck dissection + radiotherapy ± chemotherapy |
| Osteosarcoma | Radical resection + chemotherapy (neo-adjuvant + adjuvant) |
| Burkitt's lymphoma (jaw) | Chemotherapy (CHOP-R / high-dose methotrexate) |
| Metastatic tumours | Palliative; treat primary + bisphosphonates for bone lesions |
D. Reconstructive Considerations After Jaw Resection
- Titanium reconstruction plate - temporary/permanent.
- Iliac crest bone graft - for small to medium defects.
- Free fibula flap - gold standard for large mandibular reconstruction.
- Dental rehabilitation with implants after osseointegration.
SUMMARY
DIAGNOSIS PATHWAY FOR JAW TUMOUR
History + Examination
↓
OPG (Panoramic X-ray) - first imaging
↓
CT/CBCT for detailed bone assessment
↓
Aspiration biopsy (cyst fluid)
↓
Incisional biopsy + histopathology (DEFINITIVE)
↓
MRI / molecular tests if malignancy suspected
↓
Multidisciplinary treatment planning
- Pathogenesis = odontogenic epithelial remnants (Rests of Malassez, dental lamina rests) + MAPK/BRAF mutations in ameloblastoma + PTCH mutation in OKC.
- Gold standard diagnosis = incisional biopsy + histopathology.
- Ameloblastoma treatment = 1 cm en bloc resection + free fibula flap for reconstruction.
- OKC = most aggressive cyst; Carnoy's solution to destroy satellite cysts; related to Gorlin syndrome.
- Recurrent ameloblastoma = BRAF inhibitor (dabrafenib).
- Soap bubble X-ray = Ameloblastoma; Ground glass = Fibrous dysplasia; Sunray = Osteosarcoma.
Epulis def pathogeneis management types if there diagram animated
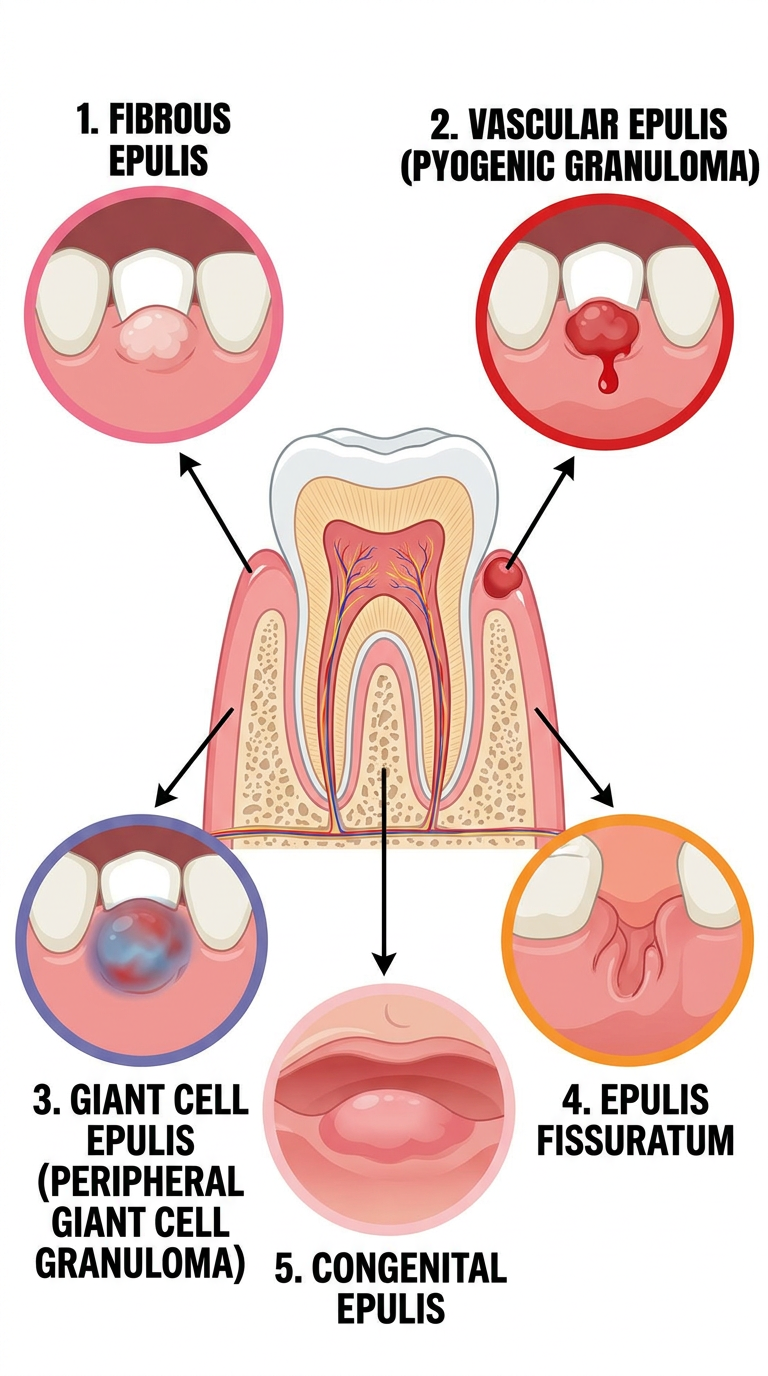
Colorful educational dental diagram poster showing 5 types of Epulis on the gingiva (gum). Each type shown as a separate labeled illustration around a central tooth cross-section diagram. Types shown: 1. Fibrous Epulis - firm pale pink nodule on gingiva between teeth, 2. Vascular Epulis (Pyogenic Granuloma) - red soft bleedy nodule on gingiva, 3. Giant Cell Epulis (Peripheral Giant Cell Granuloma) - bluish-red nodule on gingiva, 4. Epulis Fissuratum - fissured fold of gum tissue around denture flange, 5. Congenital Epulis - smooth pink mass on newborn gum ridge. Arrows pointing from each type to the gingival location. Color-coded: fibrous=pink, vascular=red, giant cell=purple-blue, fissuratum=orange, congenital=light pink. Clean medical illustration style, white background, bold labels, dental education poster.
EPULIS - Definition, Types, Pathogenesis & Management (10 Marks)
DEFINITION
Epulis is defined as any benign, localised swelling or tumour-like growth arising from the gingiva (gum tissue). It is not a single pathological entity but a clinical term covering a group of reactive, inflammatory, or neoplastic lesions originating from the gingiva or periodontal tissues.
TYPES OF EPULIS
| # | Type | Also Called | Nature |
|---|---|---|---|
| 1 | Fibrous Epulis | Peripheral fibroma / Fibrous hyperplasia | Reactive/Inflammatory |
| 2 | Vascular Epulis | Pyogenic granuloma / Pregnancy epulis | Reactive/Vascular |
| 3 | Giant Cell Epulis | Peripheral giant cell granuloma (PGCG) | Reactive |
| 4 | Epulis Fissuratum | Denture granuloma | Reactive/Irritation |
| 5 | Congenital Epulis | Granular cell tumour of newborn | Hamartoma/Tumour |
DIAGRAM
DETAILED DESCRIPTION OF EACH TYPE
1. FIBROUS EPULIS (Most Common Type)
- Chronic local irritation: dental calculus, rough tooth edges, ill-fitting crowns, orthodontic appliances
- Poor oral hygiene
- Firm, pale pink, sessile or pedunculated nodule on the gingiva
- Usually between teeth (interdental papilla region)
- Painless, slow-growing
- Surface may be ulcerated (from biting)
- Size: few mm to >1 cm
- Does NOT bleed easily
- Dense fibrous connective tissue
- Variable chronic inflammatory cell infiltrate (lymphocytes, plasma cells)
- Covered by stratified squamous epithelium
- May contain calcifications (ossifying variant = Peripheral Ossifying Fibroma)
Chronic irritation (calculus/trauma)
↓
Stimulation of gingival fibroblasts
↓
Excessive collagen/fibrous tissue production
↓
Fibrous epulis
- Remove causative irritant (scaling and root planing)
- Surgical excision down to periosteum + curettage of underlying bone
- Recurrence: 15-20% if cause not removed
2. VASCULAR EPULIS (Pyogenic Granuloma)
- Minor trauma, poor oral hygiene, dental calculus
- Pregnancy - due to elevated oestrogen/progesterone → increased vascular proliferation
- Hormonal medications (OCP)
- BRAF/RAS mutations identified in some cases
- Pregnancy Epulis (Granuloma Gravidarum): Occurs in ~1% of pregnant women; usually in 1st trimester; commonly on anterior maxillary gingiva; may spontaneously regress postpartum.
- Bright red to reddish-purple, soft, smooth or lobulated nodule
- Bleeds easily (even with gentle touch)
- Grows rapidly
- Usually painless
- Most common on anterior maxillary gingiva
- Can reach 1-2 cm size
- Lobular proliferation of capillaries (lobular capillary haemangioma)
- Loose oedematous stroma
- Abundant inflammatory cells
- Ulcerated surface common
Local trauma / Hormonal influence (pregnancy)
↓
Inflammatory mediators + VEGF ↑
↓
Capillary proliferation + granulation tissue
↓
Vascular Epulis / Pyogenic Granuloma
- Oral hygiene improvement + remove irritant
- Surgical excision - most reliable; include base + periosteum
- Alternatives: Laser (Nd:YAG, Er:YAG, pulsed dye), cryosurgery, electrocautery
- In pregnancy: conservative management initially; excise if large, bleeding, or persists postpartum
- Recurrence: ~15% (especially if incomplete excision)
3. GIANT CELL EPULIS (Peripheral Giant Cell Granuloma - PGCG)
- Bluish-red to purple, soft nodule (due to haemosiderin deposits + vascularity)
- Size: 10-20 mm (can be larger)
- Located between or around the teeth - especially anterior mandible/maxilla
- Can cause superficial bone resorption ("cupping" of underlying alveolar bone on X-ray)
- May be associated with dental implants
- Occurs at any age; slight female predilection
- Associated with cherubism (autosomal dominant; SH3BP2 mutation) when multiple
- Multinucleated osteoclast-like giant cells scattered throughout fibrovascular stroma
- Spindle-shaped mesenchymal cells
- Haemosiderin deposits + inflammatory infiltrate
- Resembles giant cell tumour of tendon sheath histologically
Local trauma / tooth extraction / ill-fitting denture
↓
RANKL-mediated osteoclast recruitment
↓
Multinucleated giant cell proliferation
↓
Giant Cell Epulis
- Must be distinguished from Central Giant Cell Granuloma (which is intraosseous) and Brown tumour of hyperparathyroidism (systemic - check PTH, Ca, PO4).
- Surgical excision + peripheral ostectomy (curettage of underlying bone)
- Check serum calcium and PTH (to rule out hyperparathyroidism)
- Recurrence: 10-15%
4. EPULIS FISSURATUM (Denture Epulis)
- Firm, fissured, whitish-pink folds of hyperplastic tissue
- Located in the labio-alveolar sulcus (vestibular fold)
- Usually fits around the denture flange like a clamp
- Painless usually; may be tender if ulcerated
- Chronic condition in elderly edentulous patients
- Dense fibrous connective tissue
- Chronic inflammatory infiltrate
- Hyperplastic epithelium; may show pseudoepitheliomatous hyperplasia
- Sometimes called granuloma fissuratum in skin literature
Worn/old/ill-fitting denture
↓
Chronic repetitive trauma to sulcus mucosa
↓
Reactive fibrous hyperplasia
↓
Epulis Fissuratum
- New well-fitting denture - mandatory first step
- Surgical excision of excess tissue (once new denture fabricated)
- Small lesions may resolve with new denture alone
- Biopsy to rule out squamous cell carcinoma (chronic irritation = risk factor)
5. CONGENITAL EPULIS (Granular Cell Tumour of Newborn)
- Present at birth (congenital)
- Smooth, pink, pedunculated nodule on the anterior maxillary or mandibular alveolar ridge
- Female predominance (8:1 female:male)
- Can interfere with feeding/breathing if large
- Regresses spontaneously in many cases
- Large polygonal cells with abundant granular eosinophilic cytoplasm
- Unlike adult granular cell tumour - S-100 negative (differentiates it)
- Exact origin unclear - possibly from primitive mesenchymal cells or undifferentiated neural crest cells of alveolar ridge
- Regresses spontaneously - suggests hormonal influence (oestrogen receptor positive in some)
- Small lesions: observe (may regress spontaneously)
- Large/symptomatic lesions: surgical excision
- Excellent prognosis; no recurrence after excision
COMPARISON TABLE
| Feature | Fibrous | Vascular (Pyogenic G.) | Giant Cell | Epulis Fissuratum | Congenital |
|---|---|---|---|---|---|
| Colour | Pale pink | Bright red/purple | Bluish-red | Whitish-pink | Pink |
| Consistency | Firm | Soft | Soft-moderate | Firm | Soft |
| Bleeding | Minimal | Profuse | Moderate | Minimal | Minimal |
| Special association | Calculus | Pregnancy | Hyperparathyroidism | Ill-fitting denture | Newborn |
| Histology | Dense fibrous CT | Lobular capillary haemangioma | Multinucleated giant cells | Dense fibrous CT | Granular cells (S-100 -ve) |
| Bone involvement | Rare | No | "Cupping" erosion | No | No |
| Recurrence | 15-20% | 15% | 10-15% | Low if cause removed | None |
| Treatment | Excision + remove irritant | Excision / Laser | Excision + ostectomy | New denture + excision | Observe / Excise |
GENERAL MANAGEMENT PRINCIPLES
STEP 1: History (irritant? pregnancy? denture? newborn?)
STEP 2: Clinical examination + X-ray (OPG/periapical)
STEP 3: Remove causative factor (calculus, ill-fitting denture)
STEP 4: Oral hygiene instruction
STEP 5: Surgical excision (under LA) + histopathological examination
STEP 6: Regular follow-up (watch for recurrence)
- Conventional scalpel excision (most common)
- Electrocautery
- Laser excision (Er:YAG, Nd:YAG, CO₂) - less bleeding, better healing
- Cryosurgery
- Peripheral ameloblastoma
- Squamous cell carcinoma
- Brown tumour of hyperparathyroidism (for giant cell epulis)
- Kaposi sarcoma (in HIV patients)
KEY EXAM POINTS
- Epulis = clinical term for ANY benign gingival swelling - not a single diagnosis.
- Most common = Fibrous epulis.
- Bleeds most = Vascular (pyogenic granuloma); especially in pregnancy.
- Bluish-red + bone cupping on X-ray = Giant cell epulis → rule out hyperparathyroidism (check PTH, serum Ca).
- Around denture flange in elderly = Epulis fissuratum → new denture first, then excise.
- Newborn + maxillary alveolar ridge + female = Congenital epulis (S-100 negative).
- Always send excised tissue for histopathology - to rule out malignancy.
- Pregnancy epulis may regress spontaneously postpartum - conservative initially.