Osteosarcoma
Reading File
Finding Sources
Searching PubMed
"osteosarcoma"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative sources. Let me compile the full response.
Osteosarcoma
Definition
Osteosarcoma is a malignant bone tumor characterized by the direct production of neoplastic osteoid or mineralized bone by tumor cells. Excluding hematopoietic tumors (multiple myeloma, lymphoma), it is the most common primary malignant bone tumor.
- Robbins & Kumar Basic Pathology, p. 782
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 1212
Epidemiology
| Feature | Detail |
|---|---|
| Incidence | ~4 per million/year; ~1-3 per million/year |
| Age distribution | Bimodal - peak at 10-20 years (adolescent growth spurt); second peak in older adults (secondary OSA) |
| Sex | Male > Female (1.6:1); exception: parosteal OSA more common in females |
| Race | No significant racial difference |
| Most common site | Metaphysis of long bones: distal femur > proximal tibia > proximal humerus (~50-75% near the knee) |
The tumor arises most frequently near the growth plate of rapidly growing bones. About 75% of all cases occur in people under 20 years old.
Classification (WHO 2013)
Seven distinct categories:
- Conventional osteosarcoma (~75% of all cases) - high-grade intramedullary
- Telangiectatic osteosarcoma - lytic, blood-filled cavities; mimics aneurysmal bone cyst
- Low-grade central osteosarcoma
- Small cell osteosarcoma (~1.5%)
- Parosteal osteosarcoma - surface, low-grade; peak in 3rd-4th decade
- Periosteal sarcoma - intermediate grade
- High-grade surface osteosarcoma
Grainger & Allison's Diagnostic Radiology, p. 1048
Predisposing Conditions
Primary (de novo): Most common in adolescents with no underlying disease.
Secondary osteosarcomas (constitute ~half of OSA in patients >50 years):
- Paget disease - most common secondary cause; incidence ~1% (5-10% in advanced polyostotic disease); pelvis most common location; patients in 6th-8th decades
- Prior radiation therapy - occurs in ~1% of patients receiving >2500 cGy; latency 10-15 years (range 3 years to decades)
- Li-Fraumeni syndrome (TP53 germline mutation)
- Hereditary retinoblastoma (RB germline mutation - 1000-fold increased risk)
- Rothmund-Thomson syndrome
- Less commonly: fibrous dysplasia, bone infarcts, chronic osteomyelitis, osteochondromas
Pathogenesis & Molecular Biology
Osteosarcomas are characterized by complex karyotypes with numerous chromosomal aberrations:
| Gene | Alteration | Significance |
|---|---|---|
| RB | Mutated in ~70% of sporadic cases | Germline mutation → 1000x increased risk |
| TP53 | Germline mutation = Li-Fraumeni syndrome | Somatic mutations common in sporadic tumors |
| MDM2 / CDK4 | Overexpressed in low-grade OSA | Inhibit p53 and RB function respectively |
| CDKN2A (INK4a) | Inactivated in many OSA | Encodes p16 and p14 tumor suppressors |
| MYC | Amplified in ~50% | Associated with particularly poor prognosis |
Robbins & Kumar Basic Pathology, p. 782-783
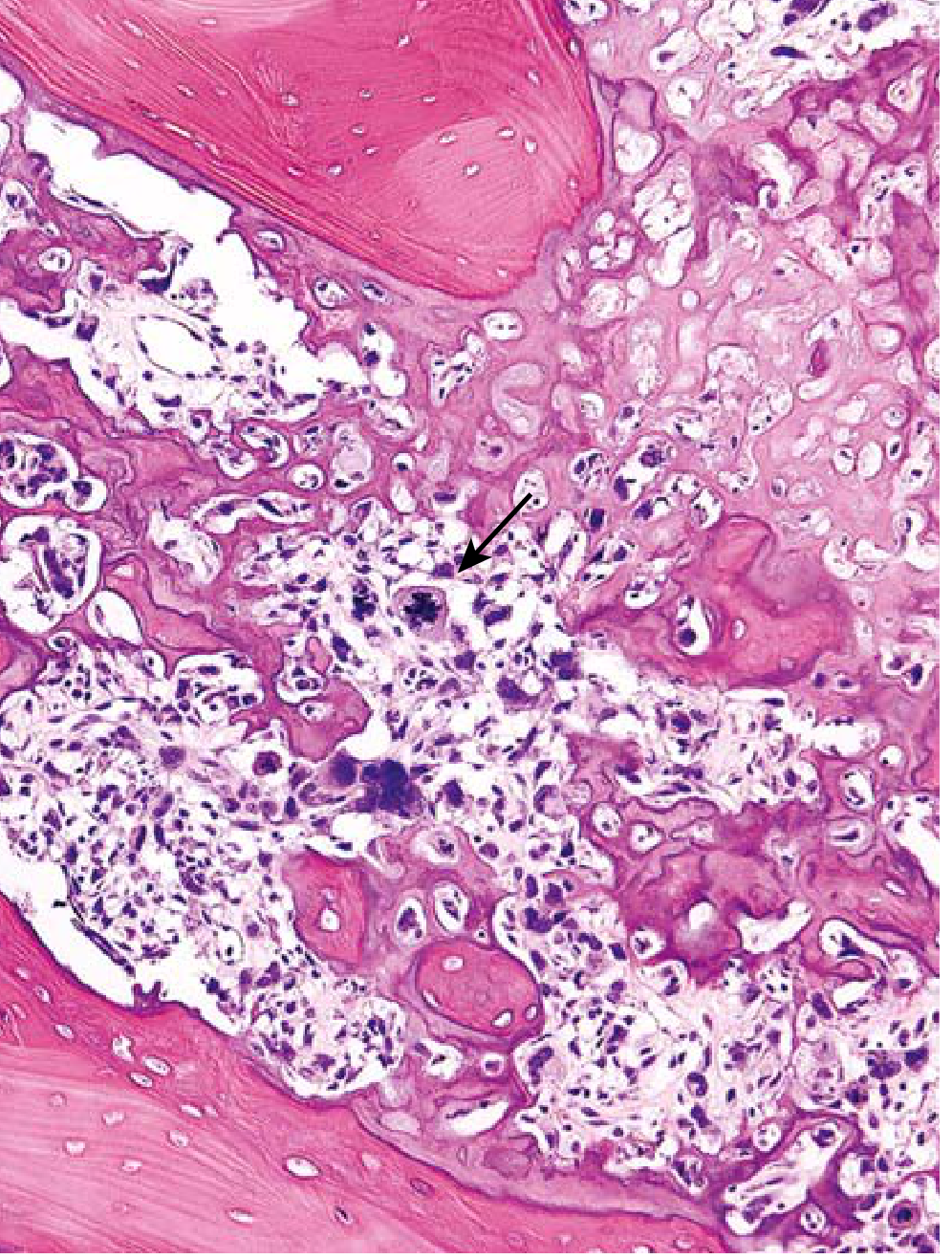
Morphology / Histopathology
Gross: Bulky, gritty, tan-white tumor; areas of hemorrhage; destroys cortex and invades soft tissue. Intramedullary spread replaces marrow. Rarely penetrates epiphyseal plate.
Microscopy:
- Pleomorphic tumor cells with large hyperchromatic nuclei
- Bizarre tumor giant cells
- Abundant mitoses including abnormal (bipolar) forms
- Extensive necrosis and intravascular invasion
- Diagnostic requirement: malignant tumor cells producing unmineralized osteoid or mineralized bone - typically fine and lacelike, but can appear as broad sheets or primitive trabeculae
Histological subtypes of conventional OSA:
- Osteoblastic (most common)
- Chondroblastic - abundant cartilaginous matrix
- Fibroblastic - spindle cell predominant
Clinical Presentation
- Pain - progressive, initially intermittent; may initially improve with conservative measures (causing diagnostic delay)
- Night pain - present in ~25% of patients
- Palpable mass - progressively enlarging
- Pathologic fracture - may be the first presentation
- Low-grade surface tumors (parosteal) may present as a painless mass
- Mean diagnostic delay: ~15 weeks (patient delay ~6 weeks + physician delay ~9 weeks)
- Common misdiagnoses: growing pains, trauma, tendinitis
Campbell's Operative Orthopaedics 15th Ed 2026, p. 1212
Imaging
Plain Radiograph (most valuable initial test)
Most common appearance: aggressive metaphyseal lesion with:
- Mixed lytic and sclerotic pattern (range: purely lytic 13% to purely sclerotic)
- Cortical destruction with eccentric soft-tissue mass
- Periosteal reaction patterns:
- Sunburst/spiculated (perpendicular)
- Onion-skin (lamellated)
- Codman triangle - triangular wedge of reactive subperiosteal bone at tumor margin (indicates aggressive tumor; not pathognomonic)

MRI
- Mandatory for local surgical staging (even though contributes little to diagnosis)
- Defines tumor extent within bone and soft tissues
- Assesses joint involvement and neurovascular structures
- Must image the entire affected bone - to exclude skip metastases (tumor foci separated from the main mass within same bone)
CT Chest
- Essential to search for pulmonary metastases (lungs are the most common site of metastases)
FDG PET-CT
- Clinically superior to bone scan for detecting bone metastases
- Recommended if resources available
Grainger & Allison's Diagnostic Radiology, p. 1048-1050
Specific Variant Features
Telangiectatic Osteosarcoma
- Rare (<4%), very high-grade
- Blood-filled cavities - mimics aneurysmal bone cyst (ABC) on imaging and histology
- MRI: multiple fluid-fluid levels; distinguishing feature is nodular/solid areas with irregular walls and post-contrast enhancement
- Purely lytic on plain radiograph
- On histology: frankly malignant cells in septa of blood-filled spaces
Parosteal Osteosarcoma
- Low-grade surface tumor
- Arises from posterior cortex of distal femur (most common)
- Peak incidence 3rd-4th decades; more common in females
- Marrow cavity typically not involved (confirmed on MRI/CT)
- Slightly atypical spindle cells producing relatively normal-appearing trabeculae on histology
- Treated with wide resection (NO chemotherapy for pure low-grade lesions)
Small Cell Osteosarcoma
- ~1.5% of cases
- Small blue cells - may resemble Ewing sarcoma or lymphoma
- Requires cytogenetics and immunohistochemistry for differentiation
- Clinical/radiological features identical to conventional OSA
Multicentric Osteosarcoma
- Synchronous: multiple sclerotic metaphyseal lesions simultaneously; typically children/adolescents; prognosis as poor as metastatic disease
- Metachronous: second lesion appears >5 months later; relatively better prognosis
Staging
The Enneking (Musculoskeletal Tumor Society) system is commonly used:
- Stage I: low-grade (IA = intracompartmental; IB = extracompartmental)
- Stage II: high-grade (IIA = intracompartmental; IIB = extracompartmental)
- Stage III: any grade with metastases
Most conventional osteosarcomas present as Stage IIB (high-grade, extracompartmental).
Treatment
Overview
Historically, treatment was immediate wide/radical amputation - yet 80% of patients died of distant metastases, establishing that most high-grade OSA patients have occult micrometastases at presentation.
Modern treatment: Neoadjuvant chemotherapy → Surgery → Adjuvant chemotherapy
Chemotherapy
Standard regimens include:
- High-dose methotrexate
- Doxorubicin (adriamycin)
- Cisplatin
- Ifosfamide (added in many protocols)
Histologic response to neoadjuvant chemotherapy is the strongest prognostic factor:
- Good response (>90% tumor necrosis): 5-year survival ~75-80%
- Poor response (<90% necrosis): 5-year survival ~40-45%
- This guides whether to alter adjuvant chemotherapy
Surgery
Goals: Wide surgical margins (no tumor at margins); limb salvage preferred when oncologically safe.
Limb-salvage surgery (now performed in ~85-90% of patients):
- Wide resection with endoprosthetic reconstruction
- Osteoarticular allograft
- Allograft-prosthetic composite
- Rotationplasty (in young children)
- Survival equivalent to amputation when adequate margins are achieved
Amputation indications:
- Inability to achieve wide margins with limb salvage
- Major neurovascular involvement
- Pathologic fracture through contaminated hematoma (relative indication)
Surgical Margins (Enneking classification)
| Margin Type | Definition |
|---|---|
| Wide | Normal tissue cuff around entire specimen |
| Marginal | Plane within reactive zone |
| Intralesional | Tumor entered during resection |
| Radical | Entire compartment removed |
Patients with wide or marginal (Enneking-appropriate) resections have longer survival and fewer recurrences than those with intralesional or contaminated margins.
Campbell's Operative Orthopaedics 15th Ed 2026, p. 1216
Prognosis
| Factor | Impact |
|---|---|
| Presence of metastases at diagnosis | Most important adverse factor; 5-year survival ~20-30% |
| Histologic necrosis post-chemo | >90% necrosis = good prognosis |
| Tumor location | Axial > appendicular (worse in axial); distal femur better than proximal femur |
| Surgical margins | Wide/marginal = better than intralesional |
| Size | Larger tumors = worse prognosis |
| MYC amplification | Associated with poor prognosis |
| Age | <40 years = positive prognostic effect |
Overall 5-year survival:
- Non-metastatic extremity OSA with modern chemotherapy + surgery: ~60-70%
- Metastatic disease: ~20-30%
- Spinal OSA: 5-year survival ~20% (even in age <40)
- 2-year survival with wide excision + adjuvant therapy for spinal OSA: ~60%
Metastatic Pattern
- Lungs - most common site (calcified lung metastases are characteristic on chest X-ray)
- Bone (other sites) - via hematogenous spread
- Skip metastases within same bone (intraosseous)
- Lymph node spread is rare
Follow-up
All osteosarcomas are assumed to have occult metastases at diagnosis. Structured follow-up includes:
- Chest CT every 3 months for 2 years, then every 6 months (lungs = primary metastatic site)
- Plain radiographs and MRI of primary site
- Bone scan or FDG PET-CT for skeletal surveillance
Sources:
- Robbins & Kumar Basic Pathology, pp. 782-783
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 1212-1216
- Grainger & Allison's Diagnostic Radiology, pp. 1048-1050
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 2586-2587 (spinal OSA)
This is a shared conversation. Sign in to Orris to start your own chat.