Postnasal drip
Reading File
Finding Sources
Finding Sources
Searching PubMed
"postnasal drip" OR "upper airway cough syndrome"
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile a thorough response.
Postnasal Drip (Upper Airway Cough Syndrome)
Definition
Postnasal drip (PND), also called nasal catarrh or upper airway cough syndrome (UACS), refers to excess nasal secretions draining posteriorly into the pharynx. It is one of the most common causes of chronic cough, alongside asthma and gastroesophageal reflux disease (GERD) - this triad accounts for the majority of chronic cough cases with a normal chest radiograph.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 274
- Harrison's Principles of Internal Medicine 22E, p. 2276
Pathophysiology
Under normal conditions, humans produce approximately 2 litres of nasal mucus per day. The nasal and sinus lining is composed of ciliated respiratory epithelium that transports mucus (and trapped particulate matter) posteriorly toward the pharynx to be swallowed. When this normal mucociliary clearance is disrupted - by inflammation, infection, allergy, or structural disease - secretions accumulate and the patient perceives a posterior "drip."
Cough arises via two mechanisms:
- Stimulation of sensory receptors (cough-reflex pathway) in the hypopharynx by draining secretions
- Microaspiration of secretions into the trachea
Importantly, the term "upper airway cough syndrome" acknowledges that chronic sinonasal inflammation can trigger cough even without visible physical drainage, likely through sensitization of afferent nerve endings.
- Goldman-Cecil Medicine, p. 2217-2219
- Harrison's, p. 2276
Causes / Underlying Conditions
PND is a symptom, not a disease in itself. The underlying aetiology drives management:
| Cause | Key Features |
|---|---|
| Allergic rhinitis | Sneezing, watery rhinorrhoea, ocular itch; seasonal or perennial |
| Non-allergic (vasomotor) rhinitis | Triggered by temperature, strong smells, humidity changes; no allergic component |
| Acute viral rhinosinusitis | Common cold; resolves within 2 weeks |
| Acute bacterial rhinosinusitis | Mucopurulent discharge, facial pain/pressure, symptoms >10 days or worsening after initial improvement |
| Chronic rhinosinusitis | Nasal obstruction/drainage, hyposmia, facial pressure >12 weeks despite treatment |
| Gustatory rhinitis | Triggered by eating; clear anterior drainage |
| Nasal polyposis | Seen on speculum; associated with asthma, aspirin sensitivity |
Clinical Features
- Sensation of secretions draining down the back of the throat
- Frequent need to clear the throat
- Nasal quality to the voice (rhinolalia)
- Hoarseness
- Chronic cough (often the presenting complaint)
- Nasal obstruction, congestion, or rhinorrhoea
On examination, the pharynx may appear normal OR show:
- "Cobblestoning" of the posterior pharyngeal mucosa (lymphoid follicle hypertrophy)
- Visible secretions draining along the posterior pharyngeal wall
- Inflamed, edematous, or boggy nasal mucosa
- Polyps on anterior rhinoscopy
- Purulent secretions in bacterial disease
Note: There is no objective way to quantify postnasal drainage - the diagnosis often relies on subjective patient history.
- Murray & Nadel's, p. 274
- Harrison's, p. 2278
Investigations
| Investigation | Finding |
|---|---|
| CT sinuses/nasal passages | Mucosal thickening, sinus opacification, air-fluid levels (rhinosinusitis) |
| Nasal endoscopy | Mucosal disease, polyps, drainage from ostia |
| Allergy skin testing / specific IgE | Identifies allergen sensitization |
| Peak nasal inspiratory flow | Assesses nasal obstruction |
| Spirometry | Excludes concomitant asthma |
CT may reveal rhinosinusitis (mucosal thickening or sinus opacification) even when physical examination is unremarkable. Extrathoracic variable upper airway obstruction may occasionally be demonstrated on flow-volume loops.
Treatment
Treatment is directed at the underlying cause. Specific approaches include:
1. Topical intranasal corticosteroids (first line)
- Applied in the head-down position to maximise delivery to the sinus ostia
- Provide local anti-inflammatory effect with minimal systemic side effects
- Effective for allergic and non-allergic rhinitis, chronic rhinosinusitis
2. Antihistamines
- Particularly useful in allergic rhinitis
- Older (sedating) antihistamines may have some drying benefit via anticholinergic effects; newer non-sedating agents are preferred for most patients
3. Ipratropium bromide nasal spray (anticholinergic)
- Reduces excessive nasal secretions (hypersecretion/rhinorrhoea)
- Useful adjunct, especially in vasomotor/gustatory rhinitis
4. Combination therapy
- A combination of topical corticosteroid + antihistamine + anticholinergic has been shown to benefit the chronic cough from PND, along with improving nasal discharge and endoscopic appearances
5. Short course of oral corticosteroids
- For severe disease to gain initial control; followed by topical maintenance therapy
6. Topical decongestants (e.g. oxymetazoline)
- Useful for a few days only as adjunct therapy
- Avoid prolonged use - rebound nasal congestion (rhinitis medicamentosa) develops
7. Antibiotics
- Indicated for acute bacterial sinusitis with mucopurulent secretions persisting for at least 10 days
- Not indicated for viral rhinosinusitis
8. Allergen avoidance / immunotherapy
-
For confirmed allergic rhinitis with identifiable triggers
-
Murray & Nadel's, p. 276-293
-
Goldman-Cecil, p. 2412
PND as Part of the "Chronic Cough Triad"
PND, asthma, and GERD together account for the vast majority of chronic cough cases (>8 weeks) with a normal chest radiograph. In clinical practice:
-
Start by identifying and treating PND
-
If cough persists, evaluate for asthma and GERD
-
Consider ACE inhibitor-induced cough (affects 5-30% of patients on these agents)
-
Emerging concept: cough hypersensitivity syndrome - sensitized sensory nerve endings as a neuropathic-type cause of refractory cough after other etiologies are excluded
-
Fishman's Pulmonary Diseases, p. 3934
-
Harrison's, p. 2272-2276
Special Populations
- Older adults: Nasal drainage and PND are among the most common nasal complaints, along with sneezing, coughing, olfactory loss, and gustatory rhinitis (Cummings Otolaryngology).
- Children: PND with recurrent rhinosinusitis and/or adenoid hypertrophy may warrant adenoidectomy as an intervention.
- Unilateral PND with other features (epistaxis, facial swelling, proptosis): Raises concern for sinonasal tumour and warrants imaging and biopsy.
Paradoxical breathing
Finding Sources
Finding Sources
Searching PubMed
"paradoxical breathing" OR "paradoxical chest wall movement"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full response.
Paradoxical Breathing
Definition
Paradoxical breathing refers to an abnormal pattern of chest wall movement in which the chest or abdominal wall moves in the opposite direction to normal during the respiratory cycle:
- Normal: Chest wall moves outward on inspiration, inward on expiration
- Paradoxical: Chest wall (or a segment of it) moves inward on inspiration, outward on expiration
The term is also used more broadly to describe loss of synchronicity between chest and abdominal movements during respiration - specifically, abnormal sinking of the abdomen during inspiration, which is an unequivocal sign of diaphragmatic failure.
- Bradley and Daroff's Neurology in Clinical Practice, p. 3292
- Fishman's Pulmonary Diseases and Disorders, p. 3782
Causes
Paradoxical breathing arises from two fundamentally different mechanisms:
1. Chest Wall Disruption - Flail Chest
Flail chest is the classic mechanical cause and represents the most severe form of blunt thoracic injury.
- Anatomic definition: Three or more consecutive ribs fractured in two or more locations, creating a segment that loses continuity with the rest of the chest wall
- Clinical definition: The flail segment demonstrates paradoxical motion - collapsing inward during inspiration and moving outward during expiration
Mechanism (Fishman's):
During inspiration, intrapleural pressure becomes subatmospheric. In an intact chest, this negative pressure drives rib cage expansion. In flail chest, the disconnected segment is no longer coupled to rib-expanding forces, so it responds directly to pleural pressure - it is sucked inward as the rest of the chest expands. During expiration, rising pleural pressure pushes it back outward.
Paradoxical motion is worsened when:
- Lung compliance is reduced (pulmonary contusion, atelectasis)
- Airway resistance is increased (secretions, bronchospasm)
- These factors amplify the normal swings in pleural pressure
Locations of flail chest:
| Location | Notes |
|---|---|
| Lateral (most common) | Anterolateral or posterolateral flail segment from blunt trauma |
| Anterior | Sternum-rib dissociation via costal cartilage/sternal fractures |
| Posterior | Least severe clinically - splinted by paravertebral muscles |
Paradoxical motion may be absent despite anatomical flail if fractures are undisplaced, in early muscle splinting, or segment lies under the scapula.
- Rockwood and Green's Fractures in Adults, p. 711-720
- Fishman's, p. 1756-1764
2. Respiratory Muscle Failure - Neuromuscular Causes
Paradoxical breathing here reflects loss of diaphragmatic and/or intercostal muscle coordination:
- Diaphragm failure: The abdomen sinks inward during inspiration (instead of moving outward as the diaphragm descends). This pattern is the classic sign of diaphragmatic paralysis.
- Intercostal + diaphragm imbalance: Seen in cervical spinal cord injury (intercostals paralysed, diaphragm partially preserved) and in conditions like spinal muscular atrophy (SMA), where intercostal weakness relative to preserved diaphragm strength produces a bell-shaped chest deformity with paradoxical breathing over time.
- Respiratory muscle fatigue: Fatigue of both diaphragm and intercostal muscles sufficient to disturb coordinated contractions can produce paradoxical breathing as a herald of impending respiratory failure.
Common neuromuscular causes include:
-
High cervical spinal cord injury (C3-C5 or higher - phrenic nerve involvement)
-
Guillain-Barré syndrome
-
Myasthenia gravis (severe)
-
Amyotrophic lateral sclerosis (ALS)
-
Spinal muscular atrophy (SMA)
-
Critical illness polyneuropathy/myopathy
-
Severe electrolyte disturbances (hypophosphataemia, hypomagnesaemia)
-
Bradley and Daroff's, p. 3292
-
Thompson & Thompson Genetics, p. 1115
-
Fishman's, p. 3782
3. Upper Airway Obstruction
During complete or near-complete upper airway obstruction, the patient's vigorous inspiratory effort against a closed airway generates extreme negative intrathoracic pressure. This causes:
- Retraction of the sternal notch
- Exaggerated abdominal muscle activity / protrusion of the abdomen
- Collapse of the chest wall with inspiratory effort
The resulting "rocking motion" (chest in, abdomen out during inspiration) becomes more prominent as obstruction worsens. This pattern is particularly seen with:
- Obstructive sleep apnoea (OSA)
- Upper airway resistance syndrome (UARS) in children
- Post-extubation/post-anaesthesia pharyngeal collapse (loss of pharyngeal tone)
- Laryngospasm
- Foreign body or epiglottitis
Relief is achieved by opening the airway (chin lift, jaw thrust, CPAP, or airway adjuncts), which abolishes the pattern.
- Miller's Anesthesia, p. 1267-1268
- Cummings Otolaryngology, p. 3245
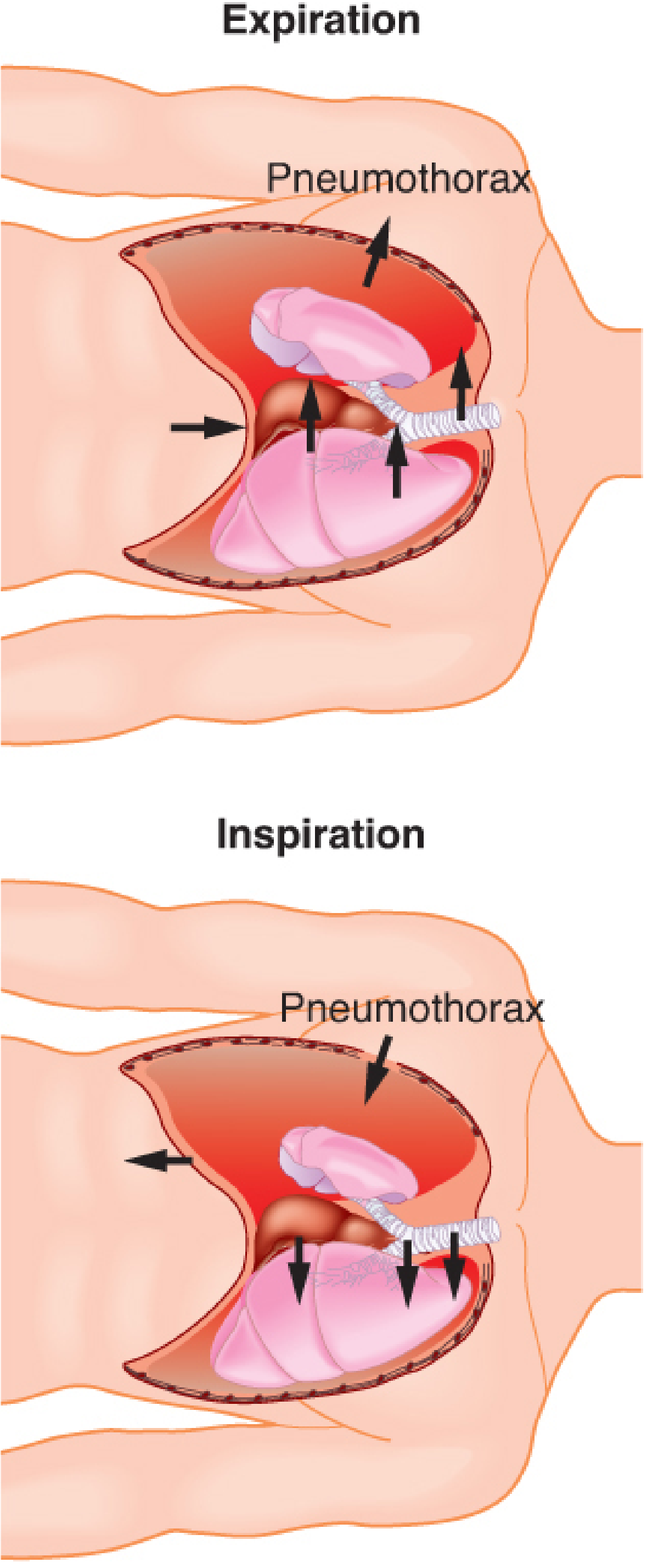
4. Open Chest / Thoracotomy Setting
When the thoracic cavity is surgically opened in a spontaneously breathing patient:
-
Atmospheric pressure enters the open hemithorax, while the intact hemithorax remains at negative pressure
-
During inspiration, air moves from the open lung into the intact lung rather than in from outside
-
During expiration, the reverse occurs
-
This intra-thoracic gas movement (historically called pendelluft) represents wasted ventilation and impairs gas exchange
-
This is abolished by positive pressure ventilation (PPV) or adequate sealing of the chest
-
Barash's Clinical Anesthesia, p. 757-758
Clinical Significance
| Context | What Paradoxical Breathing Signals |
|---|---|
| Trauma patient | Flail chest - look for underlying pulmonary contusion and ARDS |
| Neurology ICU | Impending neuromuscular respiratory failure - consider early intubation |
| Post-anaesthesia recovery | Upper airway obstruction, possibly residual neuromuscular blockade |
| Sleeping child | Upper airway resistance syndrome, OSA |
| General examination | Diaphragmatic paralysis (unilateral or bilateral) |
Pathophysiology of Respiratory Failure in Flail Chest
An important conceptual update (from Murray & Nadel's and Fishman's):
The paradoxical wall movement itself is NOT the primary cause of respiratory failure. Rather, the respiratory impairment is driven by the underlying pulmonary contusion, pain-induced splinting, atelectasis, and increased work of breathing.
The old "pendelluft" theory - that gas shuttled back and forth between lungs causing hypoxia - has been largely disproven. Modern management targets the underlying lung injury and pain control, not simply the chest wall mechanics.
Consequences of flail chest:
-
VC and FRC reduced by up to 50% of predicted
-
Pain impairs cough effectiveness → secretion retention → pneumonia
-
Increased elastic and resistive load on respiratory muscles
-
Inspiratory muscles shorten excessively (extra work not captured by standard measurements)
-
Shortened mean operating length reduces inspiratory muscle efficiency
-
Combined: respiratory muscle fatigue → respiratory failure
-
Murray & Nadel's, p. 2321-2323
-
Fishman's, p. 1764-1766
Management
Flail Chest:
- Pain control is paramount - thoracic epidural analgesia (TEA) is the preferred modality (Eastern Association for Surgery of Trauma guidelines); if epidural is contraindicated, thoracic paravertebral block (TPVB)
- Mild-moderate respiratory compromise: trial of non-invasive ventilation (NIV/CPAP) with TEA before intubation
- Endotracheal intubation + mechanical ventilation for abnormal gas exchange - not merely for paradoxical motion
- Mechanical ventilation to treat chest wall motion alone is not recommended
- Surgical rib fixation improves long-term outcomes (returns VC to normal in ~3 months); underused in the US
Neuromuscular:
- Serial monitoring of respiratory parameters (VC <20 mL/kg, MIP <-30 cmH₂O, MEP <40 cmH₂O = "20-30-40 rule" for intubation threshold in GBS)
- Early non-invasive ventilation; anticipate mechanical ventilation
- Treat underlying cause where possible
Upper Airway Obstruction:
-
Chin lift / jaw thrust
-
Oral or nasal airway adjunct
-
CPAP via face mask
-
Laryngeal mask airway or endotracheal intubation for refractory cases
-
Murray & Nadel's, p. 2323-2324
-
Miller's Anesthesia, p. 1268

photo-1784267388430.jpg
Exaplain grunting
analyse_media
Finding Sources
Finding Sources
Reading File
Reading File
Excellent - I have comprehensive data from authoritative sources. I can now give a thorough, well-cited explanation that also addresses what the textbook in the image states.
Grunting - Explained
What the book in your image says
Your textbook states:
"Grunting: In this condition, expiration occurs with a partially closed glottis. This occurs in patients with decreased or absent pulmonary surfactant. When the alveoli collapse, the walls of the alveoli stick to each other with each respiratory cycle. The work of breathing will be enormous to release those alveoli. Hence, as an adaptive mechanism, the child maintains a positive-end expiratory pressure at the end of the expiratory phase. This causes an expiratory grunt."
This is an accurate and well-summarized clinical description. Here is the full physiology behind it:
Definition
Grunting is a low-pitched expiratory sound produced when an infant (or occasionally an adult) breathes out against a partially closed glottis. It is a sign of significant respiratory distress and always warrants urgent evaluation.
The Physiological Problem: Surfactant Deficiency
To understand grunting, you must first understand what surfactant does:
- Surfactant is a phospholipid-protein mixture (mainly dipalmitoylphosphatidylcholine, DPPC) lining the alveoli
- It reduces surface tension at the air-liquid interface inside alveoli
- By Laplace's law (P = 2T/r), small alveoli have higher collapsing pressure; surfactant reduces this by lowering T
- Without surfactant, alveoli collapse at end-expiration (atelectasis)
In neonates - particularly premature infants - surfactant production is insufficient, causing Respiratory Distress Syndrome (RDS / Hyaline Membrane Disease).
The consequence: lung compliance is extremely low. The PTP-VL (transpulmonary pressure - volume) curve is shifted such that generating a breath from a collapsed alveolus requires enormous inspiratory effort. The walls of collapsed alveoli stick together (due to high surface tension), and enormous pressure is needed to re-open them with each breath.
- Medical Physiology (Boron & Boulpaep), p. 139
The Adaptive Mechanism: Self-Generated PEEP
The infant's respiratory system responds with a clever compensatory strategy:
- At end-expiration, rather than letting the lungs deflate all the way to their true (very low) FRC, the infant adducts the vocal cords to partially close the glottis
- This creates resistance to airflow out of the lungs
- The result: expiration halts at a higher lung volume than the true FRC - a "pseudo-FRC" or auto-PEEP effect
- The next inspiration now begins from a higher volume, where lung compliance is much greater (the pressure-volume curve is non-linear; compliance is higher at higher volumes)
- This dramatically reduces the work needed to open alveoli for the next breath
In essence, grunting = the baby generating its own CPAP using the glottis as the valve.
"Grunting is the sound made by closure of the glottis as the infant halts expiration at a lung volume (VL) that is considerably higher than the true functional residual capacity (FRC) to which the lungs would deflate without grunting... One might think of the relatively high VL at the point of grunting as a 'pseudo-FRC' from which the infant can begin the next inspiration with much less effort."
- Medical Physiology, p. 139
Clinical Context
| Condition | Mechanism of Grunting |
|---|---|
| Neonatal RDS (prematurity, surfactant deficiency) | Classic cause - prevents alveolar collapse at end-expiration |
| Transient Tachypnoea of the Newborn (TTN) | Prominent grunting; can mimic RDS but has different aetiology (retained fetal lung fluid) |
| Meconium aspiration syndrome | Obstruction + inflammation → atelectasis → grunting |
| Neonatal pneumonia / sepsis | Inflammatory lung injury, reduced compliance |
| Congenital heart disease (pulmonary oedema) | Reduced compliance due to oedema |
| Non-pulmonary causes | Hypothermia, hypoglycaemia, anaemia, polycythaemia, metabolic acidosis |
Grunting in a neonate is part of the neonatal respiratory distress syndrome constellation:
- Tachypnoea (RR >60/min)
- Expiratory grunting
- Nasal flaring
- Intercostal and subcostal retractions
- Cyanosis
- Apnoeic episodes (in severe cases)
- Creasy & Resnik's Maternal-Fetal Medicine, p. 2514
- Pye's Surgical Handicraft, p. 9440
Why the Grunt Sound is Produced
The audible grunt occurs because:
- Air is forced through a narrowed glottic opening under the pressure of the elastic recoil of the lungs
- This produces turbulent airflow and the characteristic low-pitched sound
- The sound is heard at the end of expiration
Think of it like partially blocking the end of a balloon as you release it - you hear a sound, and the balloon deflates more slowly and stops at a higher volume.
Clinical Importance
Grunting is a red flag sign - it indicates the infant is working very hard just to maintain adequate lung volume. Without intervention:
- Respiratory muscle fatigue will develop
- Progressive atelectasis and hypoxaemia
- Respiratory failure
Treatment targets the underlying cause and mimics what the grunt achieves:
- Exogenous surfactant therapy (intratracheal) - restores normal compliance and eliminates the need for grunting
- CPAP - externally provides the distending pressure the grunt was generating
- Mechanical ventilation with PEEP if severe
- Antenatal corticosteroids accelerate fetal lung maturation and surfactant production (given to mothers at risk of preterm delivery)
"The characteristic expiratory grunt is secondary to expiration through a partially closed glottis, providing continuous distending airway pressure to maintain functional residual capacity (thereby preventing alveolar collapse)."
- Creasy & Resnik's Maternal-Fetal Medicine, p. 2514
Summary in One Sentence
Grunting = expiration against a partially closed glottis → auto-PEEP → prevents alveolar collapse in surfactant-deficient lungs → reduces the catastrophic work of breathing that would otherwise be needed to re-open collapsed alveoli.
Create a comparison chart of RDS vs TTN in neonates
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the data needed. Here is the comprehensive comparison chart:
RDS vs TTN in Neonates - Comparison Chart
| Feature | RDS (Respiratory Distress Syndrome) | TTN (Transient Tachypnoea of the Newborn) |
|---|---|---|
| Also known as | Hyaline Membrane Disease (HMD) | "Wet lungs" |
| Primary cause | Surfactant deficiency | Delayed clearance of fetal lung fluid |
| Pathophysiology | Insufficient surfactant → high alveolar surface tension → alveolar collapse → atelectasis → poor compliance → respiratory failure | Retained fetal lung fluid not cleared via ENaC-mediated sodium reabsorption → interstitial/alveolar fluid → reduced compliance |
| Typical gestation | Preterm (<34 weeks most commonly; risk inversely proportional to GA) | Term and late preterm (>34 weeks); especially 34-37 weeks |
| Mode of delivery risk | Prematurity (any mode) | Caesarean section without labour (no catecholamine surge, no vaginal squeeze) |
| Onset | In delivery room or shortly after birth | Within hours of birth |
| Severity | Moderate-severe; can be life-threatening | Generally mild; self-limiting |
| Symptoms shared | Tachypnoea, grunting, nasal flaring, intercostal/subcostal retractions, cyanosis | Same triad, but typically milder |
| Grunting | Prominent - classic sign (auto-PEEP against collapsed alveoli) | Can be prominent - sometimes misdiagnosed as RDS |
| Clinical course | Worsens over first 2-3 days, then improves (or improves rapidly with surfactant) | Improves rapidly within 24-48 hours of birth |
| Recurrence risk | Risk in subsequent preterm births | No recurrence risk; no residual pulmonary dysfunction |
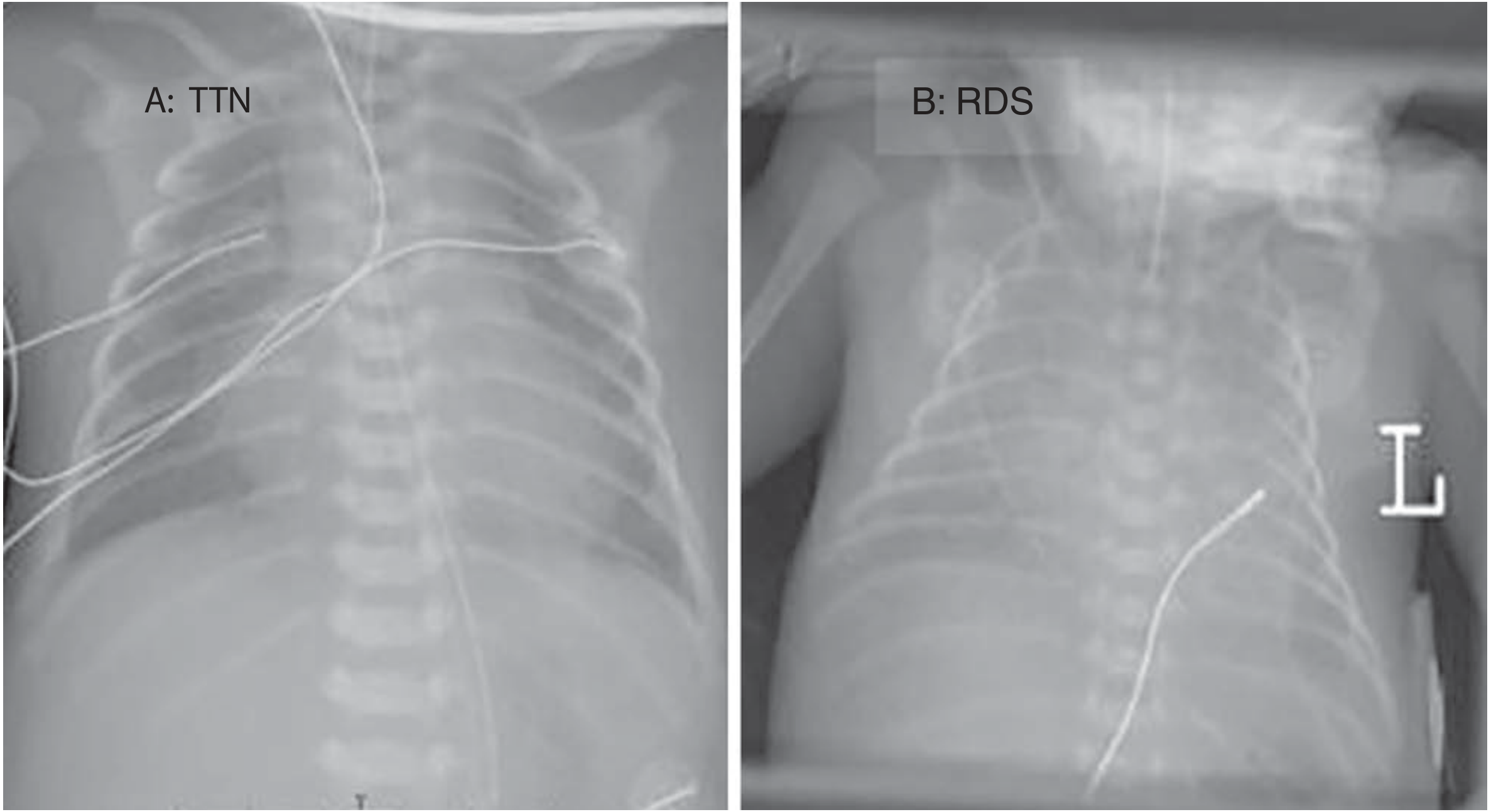
| CXR lung volumes | Low volume (hypoinflated) - atelectasis | Normal to hyperinflated (good aeration) |
| CXR pattern | Diffuse reticulogranular / ground-glass opacity; prominent air bronchograms; cardiothymic silhouette indistinct | Prominent perihilar streaking (engorged pulmonary lymphatics and vessels); fluid in fissures (esp. right minor fissure); mild haziness |
| Key CXR difference | Lungs white and collapsed, heart border obscured | Lungs aerated/expanded, perihilar congestion |
| Lung ultrasound | Increasing use in Europe - shows diffuse B-lines, absent A-lines | Shows "double lung point" - pathognomonic finding on ultrasound |
| Surfactant levels | Decreased / absent | Normal |
| Blood gases | Hypoxaemia + hypercapnia (type 2 respiratory failure) | Usually mild hypoxaemia only |
| Histology | Hyaline membranes in alveoli (proteinaceous exudate); atelectasis | Fluid in peribronchiolar lymphatics and alveolar spaces |
| Complications | Pneumothorax (air leak), PPHN, BPD (bronchopulmonary dysplasia), IVH, sepsis, death | Rarely - PPHN; delayed oral feeding; association with asthma/wheezing in later childhood |
| Mortality | Significant without treatment | Very low - self-limiting |
| Antenatal prevention | Corticosteroids (betamethasone/dexamethasone) at 24-34 weeks if preterm delivery anticipated; accelerates surfactant production | Antenatal betamethasone before late preterm/elective CS; schedule elective CS after 39 completed weeks (AAP guideline) |
| Specific treatment | Exogenous surfactant (intratracheal) - most effective intervention; CPAP/mechanical ventilation; broad-spectrum antibiotics (to rule out sepsis) | Supportive only - supplemental O₂ (SpO₂ >90%); IV fluids; nil by mouth until tachypnoea resolves; CPAP rarely needed |
| Role of CPAP | Core treatment - prevents atelectasis, preserves surfactant function | Rarely needed; reserved for persistent/severe cases |
| Mechanical ventilation | Often required in severe cases | Not typically required |
| Diuretics | Not first-line | Not effective |
| Feeding | Delayed until stabilised | Withheld until tachypnoea resolves |
| Long-term outcome | Risk of BPD; neurodevelopmental complications in very preterm | Normal; no residual lung dysfunction; possible increased asthma risk |
Key Distinguishing Points at a Glance
| Clinical clue | Think RDS | Think TTN |
|---|---|---|
| Gestational age | Very preterm | Term or late preterm |
| Delivery | Any | Elective CS without labour |
| Course | Worsening then recovery | Improves within 24-48 h |
| CXR | Low volume, ground-glass, air bronchograms | Normal/high volume, perihilar streaking, fissure fluid |
| Surfactant | Deficient | Normal |
| Response to treatment | Rapid with surfactant | Spontaneous resolution |
Key Memory Hook
RDS = lungs can't inflate (no surfactant, alveoli collapse) → gets worse firstTTN = lungs won't dry (retained fluid) → gets better fast, on its own
- Creasy & Resnik's Maternal-Fetal Medicine, p. 2425-2464, 2512-2524
- Harriet Lane Handbook 23rd Ed, p. 5767-5769
- Tintinalli's Emergency Medicine, p. 3069
This is a shared conversation. Sign in to Orris to start your own chat.