Goal directed fluid therapy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"goal-directed fluid therapy"[MeSH Terms] AND perioperative
Reading File
Reading File
Searching PubMed
"goal-directed fluid therapy" AND perioperative
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed to write a comprehensive, well-structured answer. Here it is:
Goal-Directed Fluid Therapy (GDFT)
Definition & Historical Background
Goal-directed fluid therapy (GDFT) is a strategy in which fluid administration is titrated to specific, measurable hemodynamic endpoints rather than given at fixed, weight-based rates. The concept originates from a 1983 study by Shoemaker et al. demonstrating lower mortality in critically ill patients when cardiac output and oxygen delivery were optimized to physiological goals. Since then, GDFT has been refined and widely incorporated into Enhanced Recovery After Surgery (ERAS) protocols, particularly for high-risk surgical patients.
"GDFT aims to avoid both hypovolemia and fluid excess, and it is the optimal approach for fluid administration in high-risk surgical patients."
- Morgan and Mikhail's Clinical Anesthesiology, 7e
The Core Problem GDFT Addresses
Perioperative fluid administration affects outcome in a non-linear, U-shaped fashion:
| Fluid Strategy | Adverse Outcomes |
|---|---|
| Too little (restrictive) | Acute kidney injury (shown in the RELIEF trial), tissue hypoperfusion |
| Too much (liberal) | Fluid overload: pulmonary edema, anastomotic leak, wound infection, prolonged ileus, impaired mobilization, 3-6 kg weight gain |
The RELIEF trial (the largest multicenter RCT to date comparing restrictive [≤5 mL/kg/h] vs. liberal [8 mL/kg/h] crystalloid) found more AKI with the restrictive strategy. Based on this, the target is a positive fluid balance of ~1-2 L using isotonic balanced crystalloids for major non-cardiac surgery.
GDFT replaces both extremes with a dynamic, individualized, feedback-driven approach.
Physiological Basis
Frank-Starling Mechanism
The physiological rationale comes directly from the Frank-Starling curve. On the steep (ascending) limb, small increases in preload yield large increases in stroke volume - the patient is "fluid responsive." On the flat (plateau) portion, additional fluid increases cardiac filling pressures without improving stroke volume, causing harm without benefit.
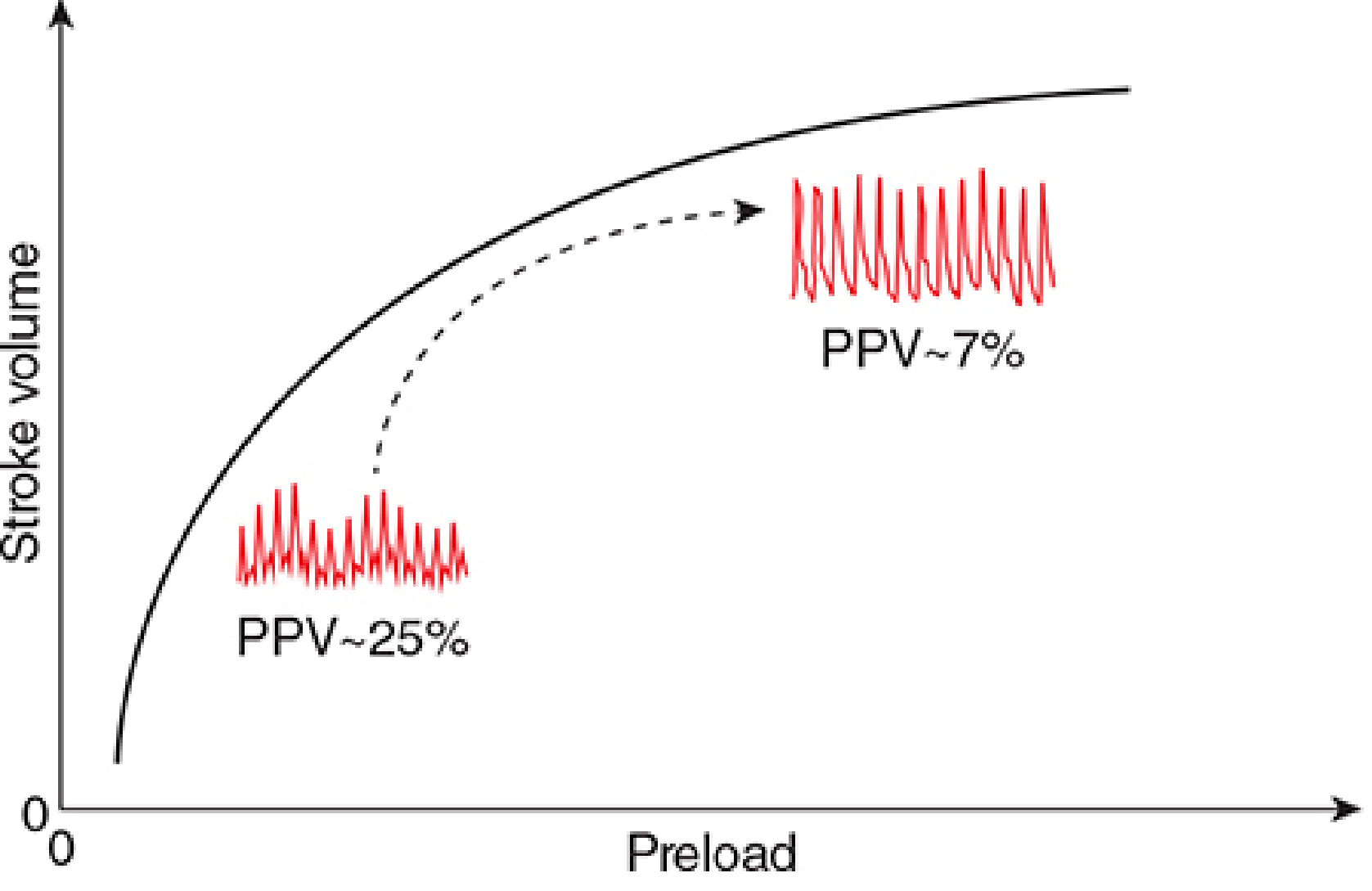
Respirophasic Hemodynamic Variation
During positive-pressure ventilation (PPV), inspiration:
- Increases intrathoracic pressure
- Reduces venous return to the right ventricle
- Decreases RV stroke volume
- This propagates to reduce LV stroke volume ~2-3 beats later (during expiration)
This cyclical variation in stroke volume - and the derived pulse pressure - is amplified in hypovolemic/preload-dependent patients (steep Starling slope) and minimal in euvolemic patients (plateau). This is the mechanistic basis for dynamic indices.
Hemodynamic Targets in GDFT
Static vs. Dynamic Parameters
| Parameter | Type | Limitation |
|---|---|---|
| CVP | Static | Poor predictor of fluid responsiveness; no longer recommended to guide fluid |
| MAP | Static | Target ≥65 mmHg (universally accepted) |
| Urine output | Static | Affected by non-volume factors; not reliable alone |
| PPV | Dynamic | Best validated predictor of fluid responsiveness |
| SVV | Dynamic | Equivalent to PPV; measured directly by pulse contour devices |
| SPV | Dynamic | Earlier described; less precise than PPV |
Pulse Pressure Variation (PPV)
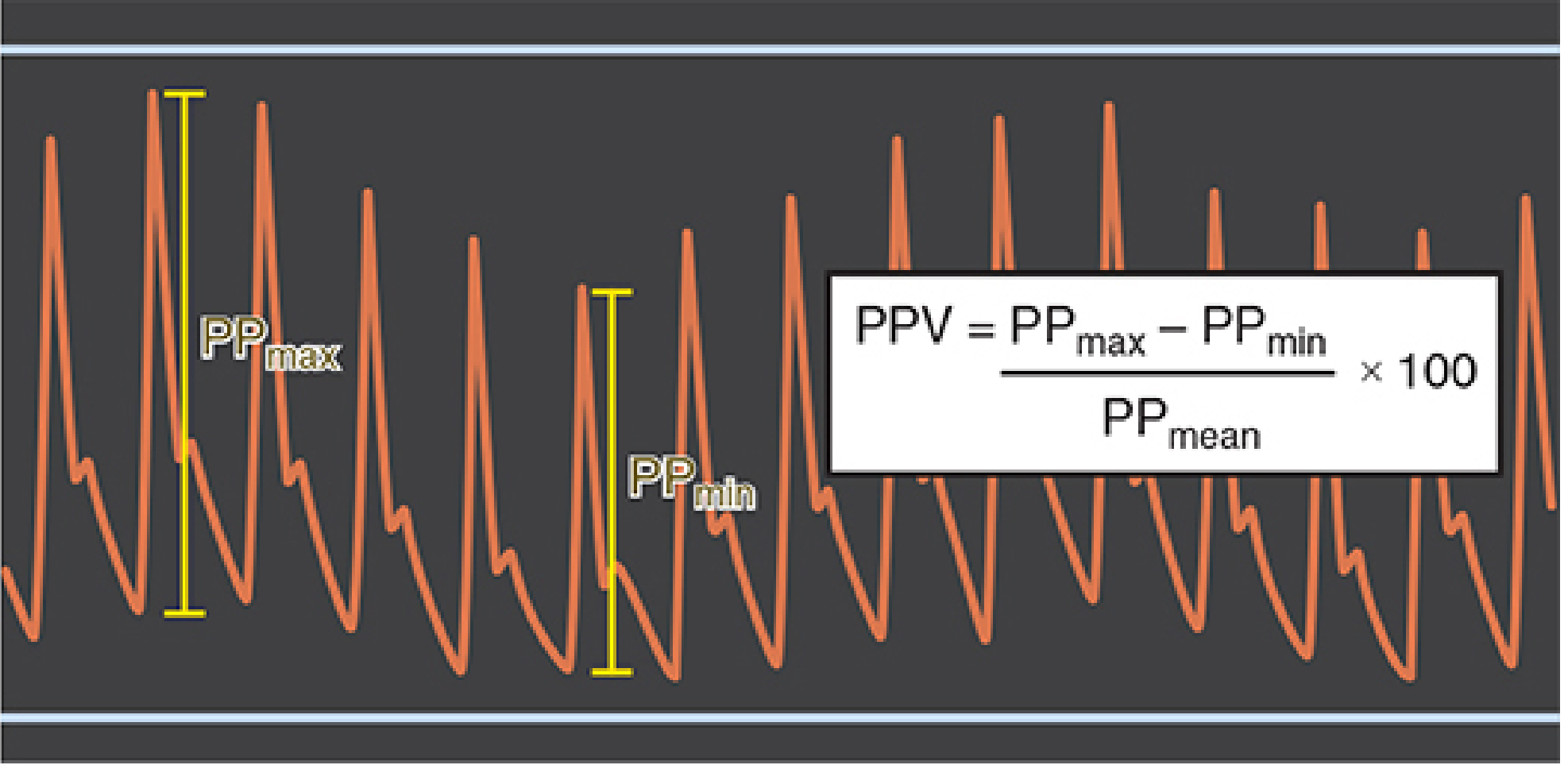
Formula:
PPV = [(PP_max - PP_min) / PP_mean] × 100
- PPV >12-13% = fluid responsive (predicts >15% increase in CO with a 500 mL crystalloid bolus)
- PPV <10% = euvolemic; further fluid unlikely to benefit
- Administer fluid boluses until PPV falls below 10%
(Morgan and Mikhail's Clinical Anesthesiology, 7e; Tintinalli's Emergency Medicine)
Limitations of PPV/SVV:
- Valid ONLY in mechanically ventilated patients with tidal volume ≥8 mL/kg
- Requires sinus rhythm (atrial fibrillation/ectopy invalidates the metric)
- Patients must be synchronous with the ventilator (not actively breathing)
- Unreliable with open chest (not with open abdomen)
- Less studied at modern low tidal volumes (6 mL/kg)
(Barash et al., Clinical Anesthesia, 9e)
Monitoring Devices
| Device | Principle | Invasiveness |
|---|---|---|
| Pulmonary artery catheter (PAC) | Thermodilution; measures CO, PCWP | Highly invasive |
| PiCCO system | Transpulmonary thermodilution + pulse contour analysis; provides CO, SVV | Arterial + CVC |
| LiDCO | Lithium dilution + pulse contour analysis | Arterial + peripheral IV |
| Esophageal Doppler | Aortic blood flow velocity Doppler; estimates CO and SV | Minimally invasive |
| TEE | Direct visualization of LV filling and outflow | Minimally invasive |
| Pleth Variability Index (PVI) | Photoplethysmographic variation; non-invasive equivalent of PPV | Non-invasive |
| TTE | Echocardiographic LVOT diameter + PW Doppler for SV | Non-invasive |
Recent meta-analysis (Felippe et al., 2025; PMID 40778974) evaluates non-invasive GDFT with PVI as a viable alternative in lower-risk patients.
Fluid Choice in GDFT
From Morgan and Mikhail's structured approach (Table 48-3):
| Physiological Loss | Replace With | Notes |
|---|---|---|
| Insensible perspiration - closed abdomen | Balanced crystalloid | 0.5 mL/kg/h |
| Insensible perspiration - open abdomen | Balanced crystalloid | 1 mL/kg/h |
| Urine output | Balanced crystalloid | Match measured output |
| Blood loss | Iso-oncotic colloid (balanced) | 1:1 ratio |
| Further preload deficit (preload optimization) | Colloid | Per dynamic monitoring |
Key principle: Crystalloids (isotonic, balanced, e.g., Lactated Ringer's or PlasmaLyte) replace extracellular losses; iso-oncotic colloids maintain intravascular volume.
GDFT Algorithm (Typical Perioperative Protocol)
Start with baseline crystalloid 3-5 mL/kg/h
↓
Measure PPV or SVV continuously
↓
PPV >12-13%? → Give colloid bolus 250-500 mL
↓
Reassess PPV after bolus
↓
PPV still >12% → repeat bolus
PPV <10% → maintain; no further bolus
↓
If MAP <65 despite adequate preload → add vasopressor (norepinephrine)
If low CO despite euvolemia → consider inotrope (dobutamine)
GDFT in Context: When is it Beneficial?
| Setting | Recommendation |
|---|---|
| High-risk patients, major open surgery (blood loss >1000 mL) | GDFT clearly indicated and beneficial |
| ERAS pathway, laparoscopic/robotic procedures | Benefit less clear; minimally invasive surgery reduces fluid shifts; aim for "zero balance" with 3-5 mL/kg/h baseline |
| Established critical illness (ICU) | GDT generally NOT effective (unlike perioperative context) |
| Elderly undergoing major surgery | Meta-analysis (Lasanudin & Mauna, 2024; PMID 40994091) supports GDFT for reducing complications |
| Oncologic surgery | Meta-analysis (Jin et al., 2025; PMID 40305698) supports intraoperative GDFT |
| Thoracic surgery / one-lung ventilation | Meta-analysis (Li et al., 2023; PMID 37723513) shows reduction in postoperative complications |
"Goal-directed fluid therapy is a good example of an intervention that is effective in the perioperative phase, but ineffective in established critical illness."
- Miller's Anesthesia, 10e
Blood Loss Management Within GDFT
- Replace blood loss with crystalloid at 3-4:1 ratio OR colloid at 1:1 until transfusion trigger reached
- Transfusion trigger: Hb <7 g/dL in healthy patients; higher threshold (Hb 8-9 g/dL) for elderly, cardiac/pulmonary disease, reduced mixed venous O₂ saturation + tachycardia
- Allowable blood loss = (RBCVpreop - RBCV₃₀%) × 3
Key Takeaways
- GDFT individualizes fluid administration using hemodynamic endpoints, avoiding the harms of both under- and over-resuscitation.
- PPV and SVV are the best-validated dynamic predictors of fluid responsiveness, but only in fully mechanically ventilated, arrhythmia-free patients.
- Fluid boluses (typically 250-500 mL colloid) are given when PPV >12-13% and stopped when PPV falls below 10%.
- In low-risk and laparoscopic ERAS patients, a simple "zero-balance" strategy with 3-5 mL/kg/h balanced crystalloid is sufficient.
- MAP <65 mmHg despite optimized preload should prompt vasopressors, not more fluid.
- GDT is effective perioperatively but has not shown benefit in established critical illness.
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Miller's Anesthesia, 10e
- Barash et al., Clinical Anesthesia, 9e
- Current Surgical Therapy, 14e
- Tintinalli's Emergency Medicine
Recent evidence:
- Jin et al. 2025, Anesth Analg - GDFT in oncologic surgery (PMID 40305698)
- Lasanudin & Mauna 2024 - GDFT in elderly (PMID 40994091)
- Li et al. 2023 - GDFT in thoracic surgery (PMID 37723513)
- Felippe et al. 2025 - Non-invasive GDFT with PVI (PMID 40778974)
Go on
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Excellent - I now have rich content on advanced fluid responsiveness techniques, echocardiographic indices, closed-loop systems, and special clinical contexts. Here is the continuation:
Goal-Directed Fluid Therapy - Advanced Topics
1. Fluid Responsiveness: The Core Concept
A patient is fluid responsive if their cardiac output (or stroke volume) increases by ≥10-15% in response to a fluid challenge. The key clinical question GDFT tries to answer continuously is: "Is this patient on the ascending limb of the Frank-Starling curve right now?"
Importantly, only ~50% of hemodynamically unstable ICU patients are actually fluid responsive at any given time. This means giving fluid empirically carries a 50% chance of causing harm without benefit - the main rationale for dynamic monitoring over fixed protocols.
2. Dynamic Tests of Fluid Responsiveness
A. Passive Leg Raise (PLR) - The Universal Test
PLR is a reversible, functional fluid challenge that transfers ~300-400 mL of venous blood from the lower limbs and abdomen into the thorax.
Technique:
- Start semi-recumbent (45°)
- Lower head to horizontal, raise legs to 45° simultaneously
- Measure CO or SV change within 60-90 seconds (the effect is transient)
- Positive: ≥10% increase in CO/SV = fluid responsive
Advantages:
- Works in spontaneously breathing patients (PPV/SVV cannot)
- Works in arrhythmia
- Works in low tidal volume ventilation
- Completely reversible - if the patient deteriorates, lowering the legs returns the fluid
The PLR must be coupled with a real-time CO measure (not just BP alone, which is unreliable). Validated CO measures for PLR include: esophageal Doppler VTI, LVOT VTI on TTE, pulse contour CO, or bioreactance.
(Current Surgical Therapy 14e; Miller's Anesthesia 10e; Surviving Sepsis Campaign 2021)
B. Fluid Challenge (Mini-Challenge)
A traditional fluid challenge of 250-500 mL is increasingly replaced by a mini-fluid challenge of 100-150 mL administered over 1 minute to reduce the risk of fluid overload from non-responders.
- Positive response: ≥10% increase in SV or CO
- Sensitivity and specificity are comparable to larger challenges when CO is measured continuously
- Closed-loop GDFT systems by Cannesson et al. use 100 mL mini-challenges to maximize SV index while minimizing total fluid given
(Miller's Anesthesia 10e)
C. End-Expiratory Occlusion (EEO) Test
In mechanically ventilated patients receiving high PEEP or low tidal volumes (where PPV/SVV are unreliable):
- Maneuver: Pause the ventilator at end-expiration for 15 seconds
- This temporarily interrupts the cyclic decrease in venous return caused by PPV
- Acts as a sustained preload increase
- Positive: ≥5% increase in pulse pressure or CO = fluid responsive
The EEO can be combined with an end-inspiratory occlusion to further characterize responsiveness.
(Miller's Anesthesia 10e)
D. Tidal Volume Challenge
In patients ventilated at low tidal volumes (6 mL/kg) where PPV is unreliable:
- Transiently increase tidal volume from 6 to 8 mL/kg for one minute
- Measure change in PPV or SVV
- A significant increase in PPV/SVV predicts fluid responsiveness
(Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e)
3. Echocardiographic Indices of Fluid Responsiveness
POCUS/TEE has become central to real-time GDFT, particularly in the ICU. All echo-derived dynamic indices require the same preconditions as PPV/SVV (full mechanical ventilation, sinus rhythm, adequate tidal volumes) unless otherwise stated.
| Index | Measurement | Threshold | Notes |
|---|---|---|---|
| ΔIVC (distensibility) | IVC diameter change with PPV: (Dmax - Dmin)/Dmin × 100 | ≥18% = responsive | Higher specificity; less accurate at Vt <8 mL/kg or PEEP >5 cmH₂O |
| ΔSVC (collapsibility) | SVC collapses on inspiration with PPV: (Dmax - Dmin)/Dmax × 100 | >36% = responsive | Requires TEE; high specificity in septic shock |
| ΔVmax Ao | Variation in peak aortic velocity with respiration via PWD | ≥12% = responsive | Highest sensitivity among echo indices |
| ΔLVOT VTI | Variation in LVOT velocity-time integral per breath | ≥10% = responsive | High sensitivity (95%), specificity 78% even at low VT with 100 mL challenge |
| SVV by echo | Direct SV variation across respiratory cycle | >12-14% = responsive | Strong positive predictive value; <10% has strong negative predictive value |
VExUS Score (Venous Congestion Assessment)
A newer echocardiographic tool that identifies over-resuscitation rather than under-resuscitation:
- IVC diameter >2 cm + abnormal hepatic vein / portal vein Doppler patterns
- Graded 0-3; higher scores predict AKI risk
- Helps decide when to stop fluids or initiate de-resuscitation
(Miller's Anesthesia 10e)
4. GDFT in Sepsis
The approach to GDFT in sepsis has evolved substantially:
Initial Resuscitation Phase (0-3 hours)
- 30 mL/kg balanced crystalloid within the first 3 hours (Surviving Sepsis)
- MAP target: >65 mmHg (vasopressors if not met with volume)
- Dynamic tests (PLR, fluid challenge) recommended over static CVP targets
- Albumin may supplement crystalloids if large volumes required; other colloids not recommended
Established Sepsis / Later Phase
- Fluid responsiveness becomes decoupled from oxygen delivery due to cytopathic hypoxia (cellular inability to utilize O₂)
- Elevating global DO₂ may give no benefit while increasing harm
- A less-positive fluid balance is associated with improved outcomes
- ARDS + sepsis: conservative fluid strategy reduces ventilator days
"In established sepsis, there is uncoupling of the O₂ delivery and consumption relationship as a result of cellular inability to use O₂ (cytopathic hypoxia). Because of this, strategies to elevate global O₂ delivery may be of little benefit while exposing patients to potential side effects of excessive fluid."
- Miller's Anesthesia, 10e
5. Fluid Type Selection
The Crystalloid Debate: Balanced vs. Normal Saline
High-chloride solutions (0.9% NaCl) cause hyperchloremic metabolic acidosis and reduce renal perfusion through afferent arteriolar vasoconstriction. Pre-post studies and subsequent RCTs (SMART trial, SALT-ED trial) demonstrated that balanced crystalloids (LR, PlasmaLyte) reduce the incidence of major adverse kidney events vs. normal saline in critically ill patients.
| Solution | Chloride (mEq/L) | pH | Notes |
|---|---|---|---|
| 0.9% NaCl | 154 | ~5 | Hyperchloremic acidosis with large volumes |
| Lactated Ringer's | 109 | 6.5 | Balanced; safe in most settings |
| PlasmaLyte 148 | 98 | 7.4 | Most physiologically similar to plasma |
In GDFT: always use balanced crystalloids for maintenance and volume replacement.
Colloids in GDFT
| Colloid | Role | Caveat |
|---|---|---|
| Albumin 4-5% (iso-oncotic) | Intravascular expansion in high-risk surgery, large-volume resuscitation | Preferred colloid when needed in sepsis |
| Albumin 20% (hyperoncotic) | Selective use in liver failure, hypoalbuminemia | May worsen AKI if used excessively |
| HES (hydroxyethyl starch) | Formerly used for rapid volume expansion | Contraindicated in sepsis and ICU patients - associated with increased AKI and mortality |
| Gelatins | Common in Europe | Evidence of increased renal injury; avoid in ICU |
6. Closed-Loop GDFT: The Next Frontier
Closed-loop (automated) GDFT systems represent the frontier of perioperative fluid management:
- Developed primarily by Cannesson et al. (University of California)
- The system monitors PPV/SVV continuously, administers 100 mL mini-fluid challenges when SVV exceeds a threshold, and simultaneously titrates vasopressors (norepinephrine) to keep MAP within ±10% of baseline
- In case-control studies, closed-loop GDFT during major abdominal surgery:
- Reduced intraoperative net fluid balance
- Reduced postoperative complications
- Shortened hospital length of stay
- Closed-loop vasopressor systems maintained MAP within ±5 mmHg of target for 91.6% of the intraoperative period vs. lower precision with manual control
- Currently used within research settings only; FDA is formulating regulatory proposals
(Miller's Anesthesia 10e)
7. GDFT Across Clinical Contexts
| Clinical Scenario | GDFT Approach | Key Consideration |
|---|---|---|
| Major open abdominal surgery | Full GDFT with CO monitor (esophageal Doppler or pulse contour); fluid boluses to max SV | Strongest evidence base; greatest benefit |
| Laparoscopic / ERAS surgery | Simplified: 3-5 mL/kg/h balanced crystalloid; aim zero balance; GDFT for high-risk patients | Minimal fluid shifts; pneumoperitoneum alters PPV validity |
| Cardiac surgery (on-pump) | Complex; cardiopulmonary bypass alters all dynamic indices; TEE for direct LV assessment preferred | Post-bypass: fluid-restrictive approach reduces respiratory complications |
| Thoracic / one-lung ventilation | PLR or EEO preferred (OLV alters PPV reliability); lung-protective co-management | Meta-analysis 2023 (PMID 37723513) shows GDFT reduces pulmonary complications |
| Septic shock | PLR + CO measure; reassess after each bolus; avoid fluid after preload optimization; vasopressors early | Later phase: fluid balance over-rides fluid responsiveness |
| ARDS | Conservative strategy; avoid positive balance after initial resuscitation | FACTT trial: fluid conservation reduces ventilator days |
| Obstetrics (spinal anesthesia) | Closed-loop phenylephrine infusions; co-loading with colloid over crystalloid pre-loading preferred | Vasopressor > fluid for spinal hypotension |
| Elderly patients | Lower threshold for GDT monitoring; more sensitive to overload; diastolic dysfunction reduces compliance | Meta-analysis 2024 (PMID 40994091) supports GDT benefit |
| Open chest | PPV/SVV invalid; use esophageal Doppler VTI, PLR, or TEE instead | Intrathoracic pressure dynamics fundamentally altered |
8. Limitations and Controversies
1. The RELIEF Trial Problem
The RELIEF trial (3000 patients, major abdominal surgery) found no difference in disability-free survival between restrictive and liberal strategies, but the restrictive arm had more AKI (8.6% vs. 5.0%) and potentially more surgical site infections. This raised concern that "zero balance" targets can be harmful. GDFT avoids this by being individualized rather than protocol-fixed.
2. PPV/SVV Validity Concerns
- Only validated at Vt ≥8 mL/kg; modern lung-protective ventilation uses 6 mL/kg
- Requires passive mechanical ventilation (no spontaneous breathing)
- Requires sinus rhythm
- Intra-abdominal hypertension, right heart failure, and open chest all impair accuracy
3. GDT in ERAS - Diminishing Returns
Evidence increasingly shows that GDFT does not add benefit in the context of a well-run ERAS pathway with minimally invasive surgery, oral pre-operative hydration, and early post-op oral intake. The fluid shifts that justify GDFT are simply not present in these patients.
4. Monitoring Device Agreement
Pulse contour and bioreactance devices tend to lose accuracy during active volume resuscitation - exactly when they are most needed. Agreement with thermodilution gold standard is variable, especially in hemodynamically unstable states.
5. GDT is Perioperative, Not ICU-Wide
A key principle from Miller's Anesthesia: GDFT is effective in the perioperative phase but not in established critical illness. This distinction prevents inappropriate application in ICU patients.
9. Summary Framework: Choosing Your GDFT Approach
Patient undergoing surgery
│
├─► Low risk / laparoscopic / ERAS
│ → 3-5 mL/kg/h balanced crystalloid
│ → No advanced monitoring needed
│ → Aim zero fluid balance
│
└─► High risk / major open surgery / expected blood loss >1L
│
├─► Mechanically ventilated, sinus rhythm, Vt ≥8 mL/kg?
│ → Use PPV/SVV (pulse contour device)
│ → Bolus if PPV >12%, stop if PPV <10%
│
├─► Spontaneous breathing / arrhythmia / low Vt?
│ → PLR + real-time CO measure (echo, Doppler)
│ → Or EEO test
│
└─► All settings
→ MAP ≥65 mmHg (vasopressor if not met by volume)
→ Replace blood loss: crystalloid 1:3 or colloid 1:1
→ Transfuse if Hb <7 (or <8-9 in high-risk cardiac pts)
→ Balanced crystalloid always (not 0.9% NaCl in large volumes)
Sources for this section:
- Miller's Anesthesia, 10e (Fluid Responsiveness, Sepsis, Closed-Loop, Perioperative Fluid)
- Morgan and Mikhail's Clinical Anesthesiology, 7e (GDFT, PPV, Fluid Tables)
- Barash et al., Clinical Anesthesia, 9e (Dynamic Respiratory Indices)
- Current Surgical Therapy, 14e (ERAS, Hemodynamic Management)
- Tintinalli's Emergency Medicine (PPV in mechanical ventilation)
This is a shared conversation. Sign in to Orris to start your own chat.