Lefort fracture and management
Reading File
Finding Sources
Searching PubMed
"LeFort fracture" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Searching the Web
LeFort fracture classification management surgical treatment guidelines 2024
Reading Web Page
https://iowaprotocols.medicine.uiowa.edu/protocols/facial-fr…
I now have comprehensive information to write a thorough answer. Let me compile everything.
LeFort Fractures: Classification and Management
Background
In 1901, René LeFort of Lille, France, conducted cadaveric experiments applying force to the midface and described the predictable lines along which the facial skeleton fractures. All three LeFort patterns share one constant feature: involvement of the pterygoid plates of the sphenoid bone, which is mandatory for the diagnosis of any LeFort fracture.
The middle third of the facial skeleton is particularly vulnerable because forces applied to the midface do not follow normal vectors of dispersion - instead they create shearing forces that can tear the facial skeleton from the cranial skeleton and extend into the skull base. - Barash Clinical Anesthesia, 9e
Classification
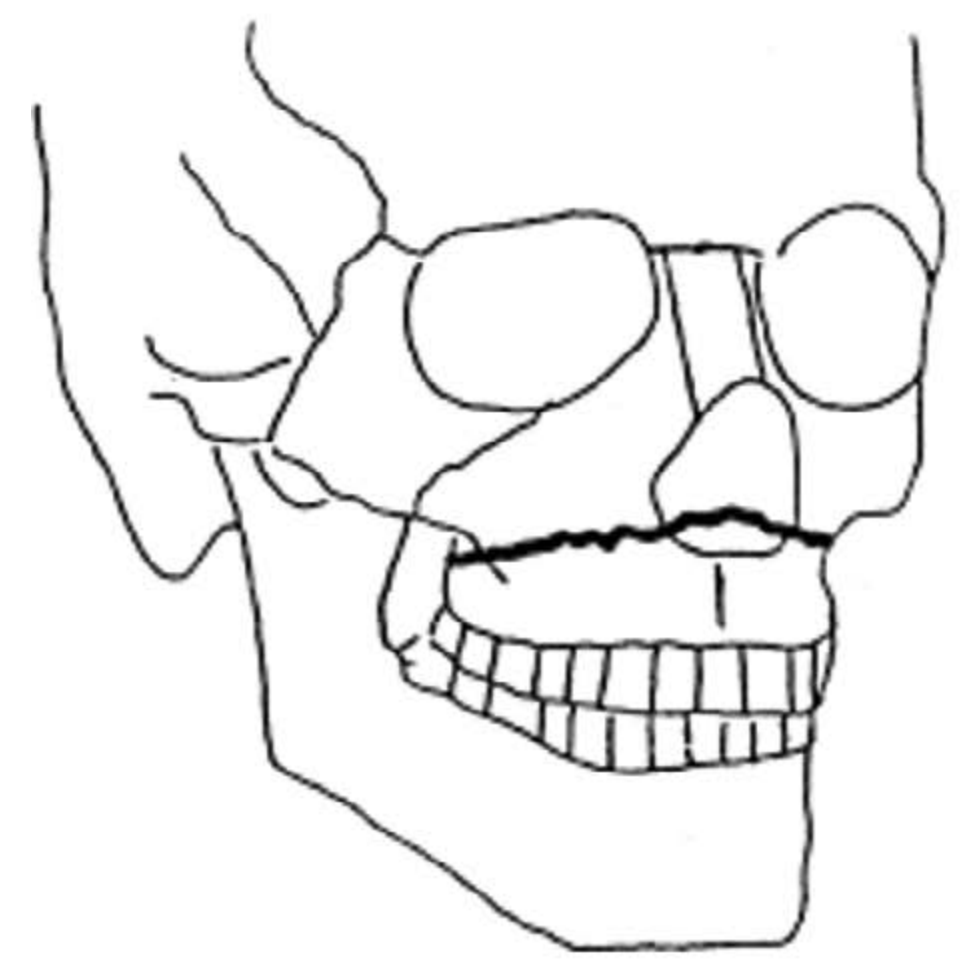
LeFort I (Horizontal / "Floating Palate")
A transverse (horizontal) fracture of the maxilla passing above the apices of the teeth, through:
- Nasal septum
- Maxillary sinuses
- Palatine bones
- Lower third of the pterygoid plates
Result: The palate, maxillary alveolar process, and upper dentition are separated from the upper midface. The fragment may be displaced posteriorly, laterally, or rotated about a vertical axis.
Mechanism: Force directed downward just below the nose and above the teeth.
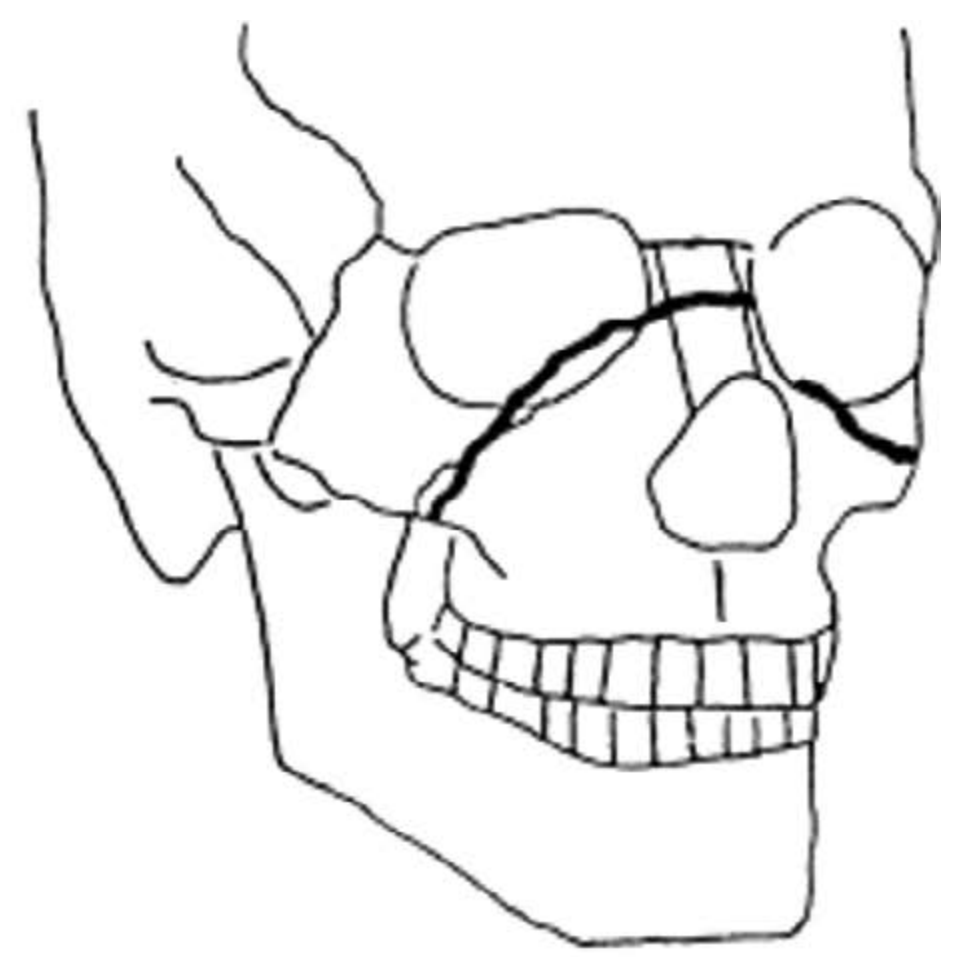
LeFort II (Pyramidal)
A pyramidal fracture beginning at the junction of the nasal bones, crossing:
- Medial wall of the orbit (including lacrimal bone)
- Inferior orbital rim
- Below the zygomaticomaxillary suture
- Lateral wall of the antrum (maxillary sinus)
- Posteriorly through the pterygoid plates
Result: A pyramid-shaped midface segment (nose + maxilla) is separated. CSF rhinorrhoea may occur. The fractured segment can be displaced posteriorly or inferiorly.
Mechanism: Trauma to the lower or mid maxilla.
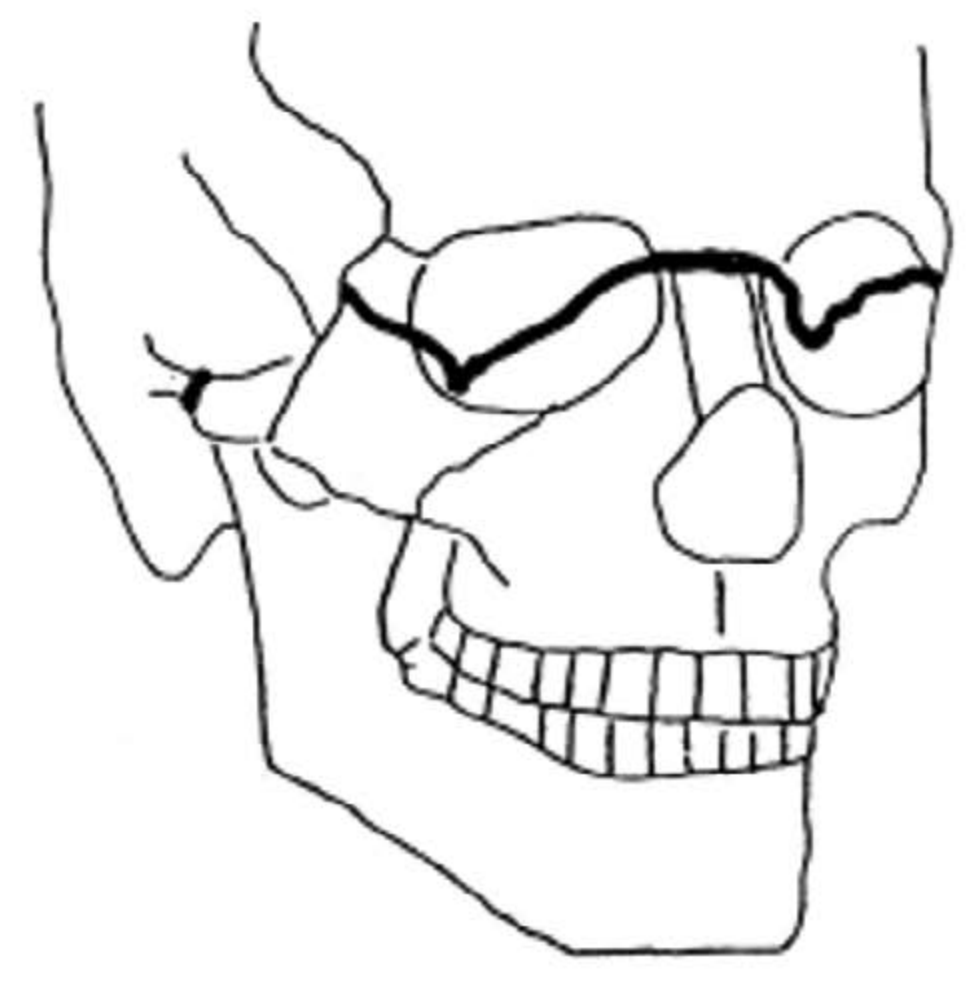
LeFort III (Craniofacial Disjunction / "Floating Face")
A high transverse fracture completely detaching the entire midface from the cranial vault, passing through:
- Nasofrontal suture
- Medial orbital wall (including ethmoids)
- Frontozygomatic sutures
- Zygomatic arches
- Sphenoid bone
Result: The entire midfacial skeleton floats free from the skull base. This is the most severe pattern; naso-orbito-ethmoid (NOE) complex fractures are commonly associated. High risk of CSF leak and intracranial injury.
Mechanism: High-velocity impact to the upper midface.
Key Comparison Table
| Feature | LeFort I | LeFort II | LeFort III |
|---|---|---|---|
| Level | Low (dentoalveolar) | Mid (pyramidal) | High (craniofacial) |
| Fracture line | Horizontal through maxilla | Pyramid through orbits & nose | Through all orbital walls + zygomatic arches |
| Structures mobilized | Palate + upper teeth | Nose + maxilla + inferior orbit | Entire midface |
| Pterygoid plates | Lower third | Full length | Full length |
| CSF leak | Rare | Possible | Common |
| Malocclusion | Yes | Yes | Yes |
| Enophthalmos | No | Possible | Common |
| "Floating face" | No | No | Yes |
Clinical Features
- Facial elongation ("dish face" or "long face" deformity)
- Malocclusion - open bite, posterior teeth contact only
- Midface mobility - classic sign: grasping upper teeth and rocking them shows movement of the midfacial segment
- Periorbital ecchymosis (bilateral "raccoon eyes") - especially LeFort II and III
- Epistaxis - often profuse
- CSF rhinorrhoea - in LeFort II and III (cribriform plate involvement)
- Subconjunctival hemorrhage
- Anaesthesia of the infraorbital nerve (LeFort II)
- Palpable "step" deformity along fracture lines
Diagnosis
Clinical: Bimanual examination - stabilize the forehead with one hand, grasp the upper dentition or anterior maxilla with the other and apply gentle anteroposterior force. Movement indicates a LeFort fracture.
Imaging:
- CT face with thin cuts and 3D reconstruction - gold standard; delineates all fracture lines, pterygoid plate involvement, orbital floor integrity, and NOE injuries
- Plain films (Waters' view) have limited sensitivity and are largely replaced by CT
- CT cervical spine should be obtained simultaneously - cervical spine fractures occur in ~1.2% of high-velocity facial injuries, and incidence of significant head injury can be as high as 88.7%
Management
1. Immediate / Emergency Priorities (ABCDEs)
Airway is the most urgent concern:
- LeFort II and III fractures can cause posterior displacement of the midface, resulting in nasopharyngeal obstruction
- Blood, edema, and displaced teeth further compromise the airway
- Nasotracheal intubation is contraindicated in LeFort II and III fractures (risk of passing the tube intracranially via a skull base defect)
- Preferred methods: video laryngoscopy, awake fiberoptic bronchoscopy, or surgical airway (tracheostomy) for severe cases
- Avoid positive-pressure ventilation until tube placement is confirmed to prevent insufflation into false passages
Other priorities:
- Control hemorrhage (maxillofacial trauma can cause significant blood loss)
- Cervical spine immobilization until cleared
- Evaluate for intracranial injury and CSF leak
- Assess for associated injuries (ocular, mandibular, NOE)
2. Non-Operative Management
Reserved for non-displaced LeFort fractures that do not disrupt occlusion. Observation with soft diet and follow-up imaging.
3. Definitive Surgical Management
The two goals of surgery are:
- Restoration of functional occlusion (correct bite)
- Reconstruction of stable bony facial contour (restore facial buttresses)
Step-wise approach:
Step 1 - Maxillomandibular Fixation (MMF)
- Erich arch bars, MMF screws, or hybrid systems are applied to the upper and lower dentition
- The maxilla is adjusted until the upper dentition fits into the mandibular wear facets (centric relation)
- Jaws are wired together, establishing the occlusal plane
- For edentulous patients, dentures are fixated to maxilla and mandible to serve as occlusal guides
- If a palatal fracture is present, it should be reduced and plated before MMF
Step 2 - Surgical Exposure
- All fractures are exposed before reduction to prevent misalignment of bone fragments
- LeFort I: Upper gingivolabial sulcus (sublabial) incision from first molar to first molar, ~5 mm superior to the gingival margin; a periosteal elevator exposes the anterior maxilla and transverse fracture lines
- LeFort II: Sublabial incision + subciliary or transconjunctival incisions for orbital floor and malar access
- LeFort III: Sublabial + subciliary/transconjunctival + brow incision for lateral orbital wall; occasionally hemicoronal incision for zygomatic arch
Step 3 - Reduction and Internal Fixation
- Rowe disimpaction forceps may be used to mobilize an impacted maxillary segment
- Facial buttresses are reconstructed using titanium miniplates and screws:
- Vertical buttresses: nasomaxillary, zygomaticomaxillary, pterygomaxillary, and mandibular rami
- Horizontal buttresses: supraorbital bar, infraorbital rim, maxillary alveolus
- LeFort II and III fractures also require accurate reduction of comminuted zygomatic and nasal bones
- Plates are applied from stable bone to the fractured segment
Step 4 - MMF release (when appropriate)
- After rigid plate fixation, MMF may be released intraoperatively to confirm occlusion
- If intermaxillary wires alone are used (selected LeFort I without significant comminution), they remain in place for 6 weeks; patients must be given wire cutters in case of emergency
4. Special Considerations
| Situation | Consideration |
|---|---|
| CSF rhinorrhoea | Usually resolves spontaneously; neurosurgical consult; prophylactic antibiotics are controversial |
| Orbital involvement | Check for diplopia, enophthalmos, globe injury; orbital floor may need mesh reconstruction |
| Palate split | Fix with plates/lag screws before MMF |
| Edentulous patient | Use dentures as occlusal guide; fix with circumzygomatic wires if needed |
| Associated NOE fracture | Medial canthal ligament repair; lacrimal system evaluation |
| Vascular injury | LeFort II or III raises risk of carotid artery injury - CTA if clinical suspicion |
Summary Mnemonic
- I = Low (1 level, palate separated) - "floating palate"
- II = Mid (pyramidal, nose + maxilla) - "floating maxilla"
- III = High (all of midface off skull) - "floating face"
Sources: Barash, Cullen & Stoelting's Clinical Anesthesia 9e (pp. 4119-4122) | DiMaio's Forensic Pathology 3e (pp. 126-127) | Iowa Head & Neck Protocols - Facial Fracture Management Handbook | StatPearls - LeFort Fractures
This is a shared conversation. Sign in to Orris to start your own chat.