Anti diabetes drug pharmacology
"antidiabetic drugs" AND "pharmacology"
Antidiabetic Drug Pharmacology
Treatment Algorithm (Type 2 Diabetes)
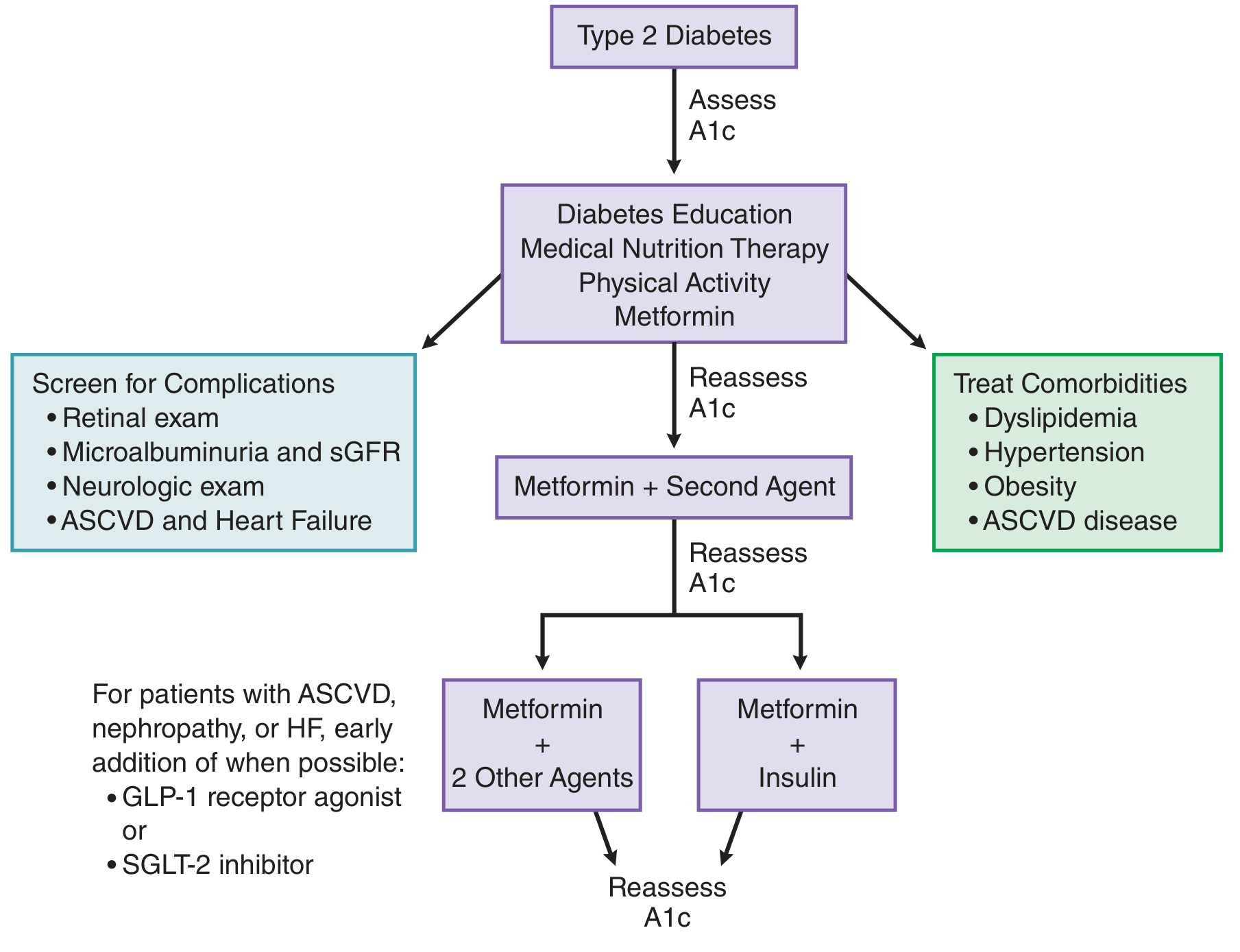
1. Insulin
Types and Pharmacokinetics
| Type | Examples | Onset | Peak | Duration |
|---|---|---|---|---|
| Short-acting (regular) | Human insulin | 30-45 min (inject before meal) | 2-4 h | 5-8 h |
| Rapid-acting analogues | Lispro, Aspart, Glulisine | <15 min | 1-2 h | 3-4 h |
| Intermediate-acting | NPH (isophane) | 1-3 h | 4-8 h | 12-18 h |
| Long-acting analogues | Glargine, Detemir, Degludec | 1-2 h | Flat/peakless | 20-24+ h |
- Lispro: B28-B29 residues swapped (Pro-Lys → Lys-Pro) - prevents hexamer formation, rapid monomer absorption
- Aspart: Proline at B28 replaced with aspartic acid - reduces self-association
- Glulisine: Glu at B29, Lys at B3 - rapid dissociation
- Glargine: Two Arg added to C-terminus of B chain + Asn21→Gly substitution on A chain; pH 4.0 solution precipitates at neutral subcutaneous pH → peakless 24-h coverage; cannot be mixed with short-acting insulins
- Detemir: Acylated with a C14 fatty acid chain → binds albumin → prolonged action
2. Metformin (Biguanide)
- First-line for type 2 diabetes at diagnosis
- Weight neutral or modest weight loss
- Does not cause hypoglycemia
- Reduces cardiovascular mortality (UKPDS data)
- Can be combined with any other antidiabetic agent
- GI (nausea, diarrhea, metallic taste) - common, mitigated by taking with food or using extended-release
- Lactic acidosis - rare but serious; risk increased in renal impairment (hold if eGFR <30), hepatic failure, acute illness, iodinated contrast exposure
- Vitamin B12 malabsorption with long-term use
3. Sulfonylureas (KATP Channel Modulators - Insulin Secretagogues)
- Type 2 diabetes only (require functioning β-cells)
- Average A1c reduction: 1-2%
- Effective as monotherapy or in combination
- Hypoglycemia - the main risk, especially with glyburide; prolonged episodes can occur
- Weight gain (1-2 kg)
- Glyburide generally not recommended due to higher hypoglycemia risk and putative adverse cardiac effects during ischemia (blocks KATP channels in cardiac muscle)
- Rare: hemolytic anemia, cholestatic jaundice
4. Meglitinides (Rapid-Acting Insulin Secretagogues)
5. Thiazolidinediones (TZDs) - "Glitazones" (Insulin Sensitizers)
- Reduce A1c by 0.5-1.4%
- Pioglitazone reduces triglycerides 10-15%, raises HDL
- Used as monotherapy or with metformin, sulfonylurea, or insulin
- Weight gain (2-4 kg) and edema (fluid retention) - dose related
- Heart failure risk increased ~2-fold (volume expansion); contraindicated in moderate-severe HF
- Increased fracture risk (especially distal limb fractures in women)
- Macular edema
- Pioglitazone: slight increased risk of bladder cancer
- Rosiglitazone: previously restricted due to cardiovascular signal (MI risk); FDA restrictions were lifted in 2013 after RECORD trial reanalysis
6. GLP-1 Receptor Agonists (Incretin Mimetics)
- Exenatide: Exendin-4 peptide (from Gila monster saliva), 53% homology to GLP-1; resistant to DPP-4 cleavage; t1/2 ~2-4 h (twice daily) or once weekly in extended-release polymer
- Liraglutide: Lys34Arg substitution + C16 fatty acid chain via glutamate spacer → albumin binding → t1/2 ~13 h → once daily injection
- Dulaglutide: GLP-1 fused to IgG Fc → t1/2 ~5 days → once weekly
- Semaglutide: Extended fatty acid modification; t1/2 ~7 days; available SC (weekly) and as oral formulation (taken fasting with water)
- A1c reduction ~1-1.5%
- Significant weight loss (2-5 kg; semaglutide up to 10-15% body weight)
- Cardiovascular benefit: Liraglutide (LEADER trial) and semaglutide (SUSTAIN-6) reduce major adverse cardiovascular events (MACE) - approved for cardiovascular risk reduction
- Renal protective effects
- Preferred add-on to metformin in patients with ASCVD
- Nausea, vomiting, diarrhea - common, improve over time; start at low dose and titrate
- Injection site reactions
- Risk of pancreatitis (rare, monitor)
- Contraindicated in personal/family history of medullary thyroid carcinoma or MEN2 (C-cell hyperplasia in rodents at high doses)
- Gallbladder disease (cholelithiasis)
7. DPP-4 Inhibitors ("Gliptins")
- A1c reduction ~0.5-0.8%
- Weight neutral
- Low hypoglycemia risk
- Well tolerated - useful in elderly and those with multiple comorbidities
- Nasopharyngitis, upper respiratory tract infections
- Rare but serious: pancreatitis, severe arthralgia (joint pain)
- Saxagliptin/alogliptin: possible increased heart failure hospitalization risk (SAVOR-TIMI, EXAMINE trials) - use caution in HF
8. SGLT2 Inhibitors ("Gliflozins")
- A1c reduction ~0.5-1.0%
- Weight loss (~2-3 kg from caloric loss in urine)
- Blood pressure reduction (~2-4 mmHg systolic)
- Heart failure benefit: Empagliflozin (EMPA-REG OUTCOME) and dapagliflozin (DAPA-HF) reduce HF hospitalization and CV death, even in non-diabetic patients. Empagliflozin approved for both HFrEF and HFpEF; dapagliflozin approved for HFrEF.
- CKD protection: Slow progression of diabetic nephropathy; dapagliflozin approved for CKD
- Preferred add-on to metformin in patients with established ASCVD or HF
- Urogenital infections - most common: mycotic (candidal) genital infections (more in women), UTIs
- Diabetic ketoacidosis (DKA) - can occur even with near-normal glucose ("euglycemic DKA") - especially in type 1 DM or peri-operative settings
- Fournier's gangrene (necrotizing fasciitis of the perineum) - rare but serious
- Bone fractures (canagliflozin)
- Polyuria, volume depletion, hypotension (especially in elderly)
- Increase in LDL cholesterol (~5%)
- Genital amputations: Canagliflozin carries an FDA black box warning for increased risk of lower limb amputation
9. Alpha-Glucosidase Inhibitors
- A1c reduction ~0.5-0.8% (modest)
- No hypoglycemia risk
- Mild weight loss
- Most useful for postprandial hyperglycemia
- Flatulence, bloating, diarrhea, abdominal pain - very common (fermentation of undigested carbohydrates in colon); often limits use
- If hypoglycemia occurs in combination therapy, must treat with glucose (dextrose), not sucrose (sucrose requires the inhibited enzyme to be absorbed)
- Contraindicated in IBD, hepatic cirrhosis
10. Miscellaneous Agents
Amylin Analogue - Pramlintide
- Synthetic analogue of amylin (co-secreted with insulin from β-cells)
- Slows gastric emptying, reduces postprandial glucagon, increases satiety
- Given as SC injection at meals; used adjunctively with insulin in T1DM and T2DM
- Main AE: nausea, hypoglycemia (insulin dose must be reduced)
Bile Acid Sequestrant - Colesevelam
- Approved for T2DM; mechanism of glucose-lowering is incompletely understood (possibly increases GLP-1 secretion or reduces bile acid-mediated hepatic glucose production)
- A1c reduction ~0.5%; reduces LDL as primary effect
- Can raise triglycerides; interferes with absorption of many drugs
Dopamine Agonist - Bromocriptine
- Low-dose (Cycloset formulation) approved for T2DM
- Thought to reset hypothalamic circadian dopamine rhythms that regulate glucose and lipid metabolism
- Modest A1c reduction ~0.5%
- AEs: nausea, orthostatic hypotension, fatigue
Summary Table
| Drug Class | Mechanism | HbA1c Reduction | Hypoglycemia Risk | Weight Effect | Key Benefit | Key Risk |
|---|---|---|---|---|---|---|
| Insulin | GLUT4 translocation, suppresses HGO | Variable (most potent) | Yes (dose-dependent) | Gain | Any DM type | Hypoglycemia, lipodystrophy |
| Metformin | ↓ Hepatic gluconeogenesis, AMPK activation | 1-2% | No | Neutral/loss | First-line, CV benefit | Lactic acidosis (rare), GI SE |
| Sulfonylureas | Block KATP → β-cell depolarization → insulin release | 1-2% | Yes | Gain | Cheap, effective | Hypoglycemia |
| Meglitinides | Block KATP (different site) - short acting | 0.5-1.5% | Yes (lower) | Gain | Prandial flexibility | Hypoglycemia |
| Thiazolidinediones | PPARγ agonist → insulin sensitization | 0.5-1.4% | No | Gain | Dyslipidemia (pioglitazone) | HF, fractures, edema |
| GLP-1 agonists | Glucose-dependent insulin↑, glucagon↓, satiety | 1-1.5% | No (mono) | Loss | CV benefit, weight loss | Nausea, pancreatitis, MTC risk |
| DPP-4 inhibitors | Prevent GLP-1/GIP degradation | 0.5-0.8% | No | Neutral | Well tolerated, elderly | Pancreatitis, arthralgia |
| SGLT2 inhibitors | Renal glucose excretion | 0.5-1% | No | Loss | HF benefit, renal protection | Genital infections, euglycemic DKA |
| Alpha-glucosidase inhibitors | Delay intestinal glucose absorption | 0.5-0.8% | No | Neutral/loss | Postprandial control | Flatulence, GI distress |
Recent Evidence (2024-2026)
Create flashcards
Medical pharmacology flashcard for Insulin. Clean, professional design with dark blue header. Front shows the question: "INSULIN - Mechanism of Action & Types". Back shows: Mechanism: Binds insulin receptor (tyrosine kinase) → PI3K/Akt signaling → GLUT4 translocation → glucose uptake in muscle/adipose; suppresses hepatic glucose output. Types table: Rapid-acting (Lispro, Aspart, Glulisine) onset 15min; Short-acting (Regular) onset 30-45min; Intermediate (NPH) onset 1-3h; Long-acting (Glargine, Detemir, Degludec) 24h peakless. Key points: Glargine pH 4.0 → precipitates at neutral SC pH → cannot mix with other insulins. Card style: white background, colored sections, bold headings, bullet points, medical education style.
Medical pharmacology flashcard for Metformin (Biguanide). Clean professional design with dark green header. Title: "METFORMIN — Biguanide". Content sections: Mechanism: Inhibits mitochondrial Complex I → ↓ ATP → ↑ AMPK activation → inhibits hepatic gluconeogenesis → ↓ hepatic glucose output. Also improves peripheral insulin sensitivity. ADME: Oral, not hepatically metabolized, renally excreted unchanged, t½ ~5h. Clinical: HbA1c ↓ 1-2%, weight neutral/loss, NO hypoglycemia, first-line T2DM. Adverse Effects: GI (nausea, diarrhea), Lactic acidosis (rare — hold if eGFR <30, contrast dye), B12 deficiency. Bold callout box: "Does NOT cause hypoglycemia". White background, green accents, medical flashcard style.
Medical pharmacology flashcard for Sulfonylureas. Clean professional design with orange header. Title: "SULFONYLUREAS — Insulin Secretagogues". Content: Examples: 1st gen (Tolbutamide, Chlorpropamide), 2nd gen (Glipizide, Glyburide, Glimepiride). Mechanism: Bind SUR1 subunit of KATP channel on β-cell → channel closes → membrane depolarization → Ca2+ influx → insulin exocytosis. Glucose-INDEPENDENT secretion. ADME: Oral, hepatically metabolized. Glyburide has active metabolites — avoid in renal failure. Clinical: HbA1c ↓ 1-2%, T2DM only (need functioning β-cells). Adverse Effects: HYPOGLYCEMIA (main risk), weight gain. Red warning box: "Glyburide NOT recommended — highest hypoglycemia risk + blocks cardiac KATP channels". White background, orange accents, medical flashcard style.
Medical pharmacology flashcard for Thiazolidinediones (TZDs / Glitazones). Clean professional design with purple header. Title: "THIAZOLIDINEDIONES (TZDs) — Insulin Sensitizers". Content: Examples: Pioglitazone, Rosiglitazone. Mechanism: Bind and activate PPARγ (nuclear receptor) → ↑ expression of insulin-sensitive genes → ↑ GLUT4 → improved insulin sensitivity in muscle, adipose, liver. Requires endogenous insulin — ineffective in T1DM. ADME: Once daily, hepatic metabolism (CYP2C8/3A4). Slow onset 1-3 months. Drug interactions: Rifampin ↓ levels; gemfibrozil ↑ levels 2x. Clinical: HbA1c ↓ 0.5-1.4%. Pioglitazone ↓ TG, ↑ HDL. Adverse Effects: Weight gain + edema, Heart failure risk ↑ 2x, Fractures (women), Bladder cancer (pioglitazone). Red warning box: "CONTRAINDICATED in moderate-severe heart failure". White background, purple accents, medical flashcard style.
Medical pharmacology flashcard for GLP-1 Receptor Agonists. Clean professional design with teal header. Title: "GLP-1 RECEPTOR AGONISTS — Incretin Mimetics". Content: Examples: Exenatide (twice daily/weekly), Liraglutide (daily), Semaglutide (weekly SC or oral), Dulaglutide (weekly). Mechanism: Mimic GLP-1 from intestinal L-cells → GLUCOSE-DEPENDENT insulin secretion ↑ → glucagon ↓ → gastric emptying slows → satiety ↑ (hypothalamic). Clinical: HbA1c ↓ 1-1.5%, significant weight loss, CV benefit (MACE reduction — LEADER trial liraglutide, SUSTAIN-6 semaglutide). Adverse Effects: Nausea/vomiting (common, improve with titration), pancreatitis (rare), gallbladder disease. Big red box: "CONTRAINDICATED: Personal/family history of Medullary Thyroid Carcinoma or MEN2". Key point: Low hypoglycemia risk (glucose-dependent). White background, teal accents, medical flashcard style.
Medical pharmacology flashcard for DPP-4 Inhibitors (Gliptins). Clean professional design with navy blue header. Title: "DPP-4 INHIBITORS — Gliptins". Content: Examples: Sitagliptin, Saxagliptin, Alogliptin, Linagliptin, Vildagliptin. Mechanism: Inhibit DPP-4 enzyme → prevent degradation of endogenous GLP-1 and GIP (t½ normally only 1-2 min) → ↑ active incretin levels → glucose-dependent insulin ↑, glucagon ↓. ADME: Oral once daily. Sitagliptin — renally excreted (dose-reduce in CKD). Linagliptin — biliary/fecal (NO dose adjustment in renal or hepatic impairment). Clinical: HbA1c ↓ 0.5-0.8%, weight neutral, low hypoglycemia, well-tolerated. Adverse Effects: Nasopharyngitis/URI, rare pancreatitis, severe arthralgia. Yellow caution box: "Saxagliptin/Alogliptin — possible ↑ HF hospitalization risk (use caution in HF)". White background, navy accents, medical flashcard style.
Medical pharmacology flashcard for SGLT2 Inhibitors (Gliflozins). Clean professional design with red-orange header. Title: "SGLT2 INHIBITORS — Gliflozins". Content: Examples: Empagliflozin, Dapagliflozin, Canagliflozin, Ertugliflozin. Mechanism: Inhibit SGLT2 in proximal renal tubule → prevent glucose reabsorption → glycosuria (~70g/day). Insulin-independent. Also cause natriuresis. Cardiac: NHE inhibition + shift to ketone/FA oxidation → heart failure benefit. Clinical: HbA1c ↓ 0.5-1%, weight loss 2-3kg, BP ↓ 2-4mmHg. Heart failure: Empagliflozin (HFrEF + HFpEF), Dapagliflozin (HFrEF). Renal protection. Adverse Effects: Genital mycotic infections (most common), Euglycemic DKA (especially T1DM), Fournier's gangrene (rare). Red box: "Canagliflozin BLACK BOX: ↑ risk lower limb amputation". White background, red-orange accents, medical flashcard style.
Medical pharmacology flashcard for Alpha-Glucosidase Inhibitors and Miscellaneous antidiabetic drugs. Clean professional design with brown/gold header. Title: "OTHER ANTIDIABETIC AGENTS". Section 1 — Alpha-Glucosidase Inhibitors (Acarbose, Miglitol): Mechanism: Inhibit intestinal α-glucosidase → delay carbohydrate absorption → blunted postprandial glucose. Taken with first bite of meal. HbA1c ↓ 0.5-0.8%. AE: Flatulence, bloating, diarrhea (very common). Important: Treat hypoglycemia with GLUCOSE (not sucrose — needs the inhibited enzyme). Section 2 — Pramlintide (Amylin analogue): Slows gastric emptying, ↓ postprandial glucagon, ↑ satiety. Adjunct to insulin in T1DM/T2DM. AE: Nausea. Section 3 — Colesevelam (Bile acid sequestrant): HbA1c ↓ 0.5%, also lowers LDL. Can ↑ triglycerides. Section 4 — Bromocriptine (Dopamine agonist, low dose): CNS mechanism, modest HbA1c ↓ 0.5%. AE: Nausea, orthostatic hypotension. White background, gold accents, medical flashcard style.