Blood supply of heart
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced information. Let me compile the full answer.
Blood Supply of the Heart
The myocardium is supplied entirely by the right coronary artery (RCA) and left coronary artery (LCA), both arising from the ascending aorta just above the aortic valve in the aortic sinuses. Blood flows from epicardial to endocardial vessels, and returns via the coronary venous system.
Arterial Supply
Diagram - Coronary Arteries (Anterior View)
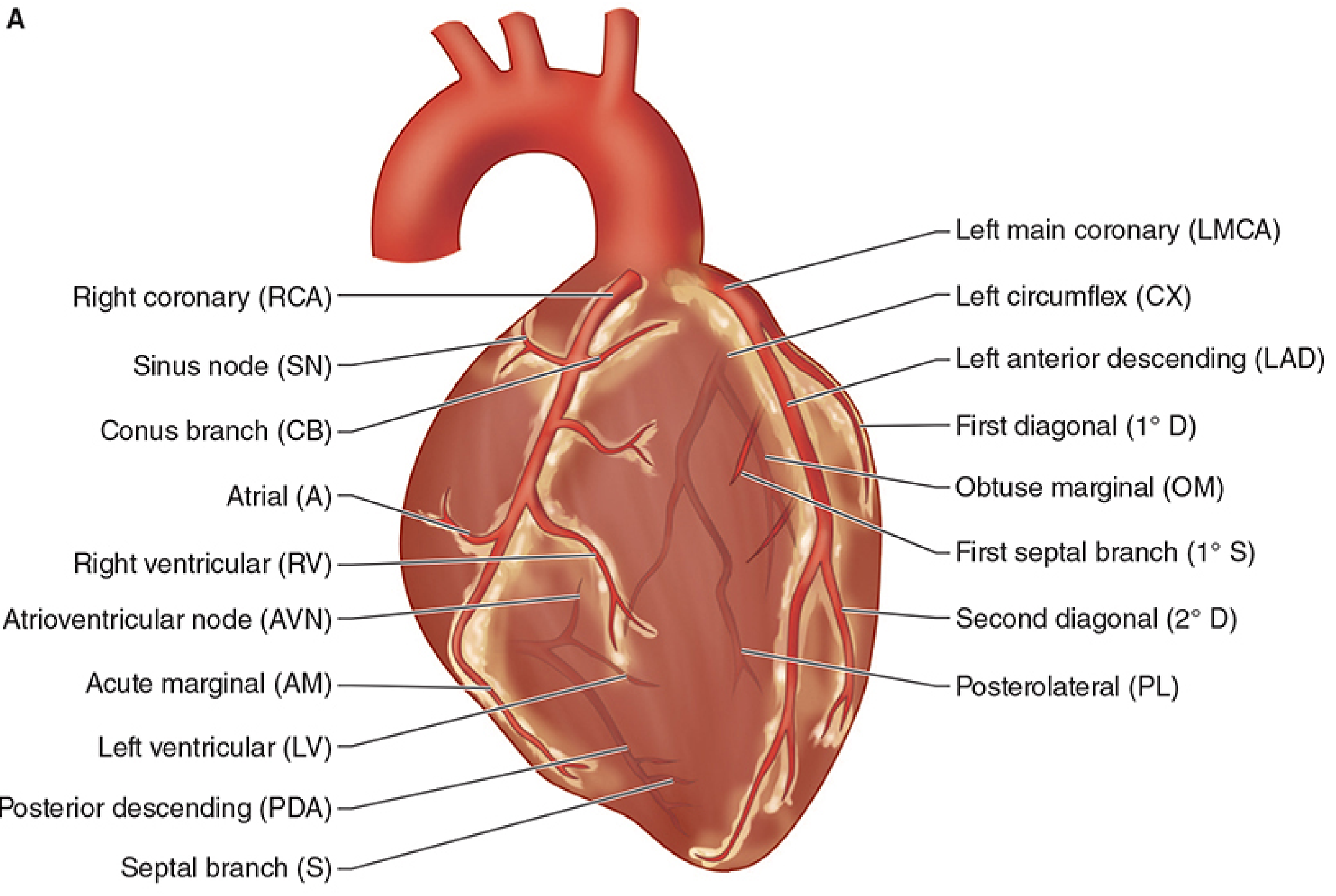
1. Right Coronary Artery (RCA)
-
Arises from the right aortic sinus, passes behind the pulmonary trunk, and runs in the right atrioventricular (coronary) sulcus.
-
Major branches:
- Sinu-atrial (SA) nodal branch - given off early, passes posteriorly around the superior vena cava to supply the SA node (in ~60% of people it comes from RCA; in ~40% from the LAD)
- Right marginal branch - arises near the inferior (acute) border; supplies the anterior surface of the right ventricle and posterior third of the interventricular septum
- AV nodal branch - small branch before the final major branch; supplies the AV node (in 85-90% of people)
- Posterior descending artery (PDA) - the terminal major branch, runs in the posterior interventricular sulcus; supplies the posteroinferior septum and inferior wall of the left ventricle
-
Territory supplied by RCA: right atrium, most of the right ventricle, SA and AV nodes, interatrial septum, a portion of the left atrium, posteroinferior 1/3 of the interventricular septum, and a portion of the posterior left ventricle.
In right dominant circulation (85% of individuals), the RCA gives rise to the PDA. In the remaining 15%, the PDA arises from the left circumflex - this is left dominant circulation.
2. Left Coronary Artery (LCA)
- Arises from the left aortic sinus of the ascending aorta, passes between the pulmonary trunk and left auricle, then enters the coronary sulcus.
- The left main coronary artery (LMCA) is short - it bifurcates quickly into two major branches:
a. Left Anterior Descending (LAD) / Anterior Interventricular Artery
- Descends in the anterior interventricular sulcus toward the apex.
- Gives off diagonal branches across the anterior surface of the left ventricle.
- Gives off septal perforating branches to the anterior 2/3 of the interventricular septum.
- Supplies: anterior wall of left ventricle, anterior 2/3 of interventricular septum, apex, and bundle of His/bundle branches.
- Called the "artery of sudden death" - most commonly occluded.
b. Circumflex (CX) Artery
-
Courses to the left in the coronary (AV) sulcus and onto the diaphragmatic surface.
-
Gives off the left marginal artery (obtuse marginal) across the rounded left border.
-
Normally ends before reaching the posterior interventricular sulcus (in right dominant circulation).
-
Supplies: left atrium, lateral and posterior walls of the left ventricle.
-
In left dominant circulation, the CX continues as the PDA.
-
Total territory of LCA: most of the left atrium and left ventricle (septal, anterior, and lateral walls), and most of the interventricular septum including the bundle of His and its branches.
Blood Supply to the Conduction System
| Structure | Artery |
|---|---|
| SA node | RCA (60%) or LAD (40%) |
| AV node | RCA (85-90%) or CX (10-15%) |
| Bundle of His | Dual supply - PDA + LAD septal perforators |
| Right bundle branch | LAD (septal perforators) |
| Left bundle branch | Dual - LAD + PDA |
| Anterior papillary muscle | Dual - LAD diagonals + CX marginals |
| Posterior papillary muscle | PDA only (most vulnerable to ischemia) |
Coronary Dominance
| Type | Prevalence | PDA Origin |
|---|---|---|
| Right dominant | 85% | RCA |
| Left dominant | ~10% | Circumflex |
| Co-dominant / Balanced | ~5% | Both |
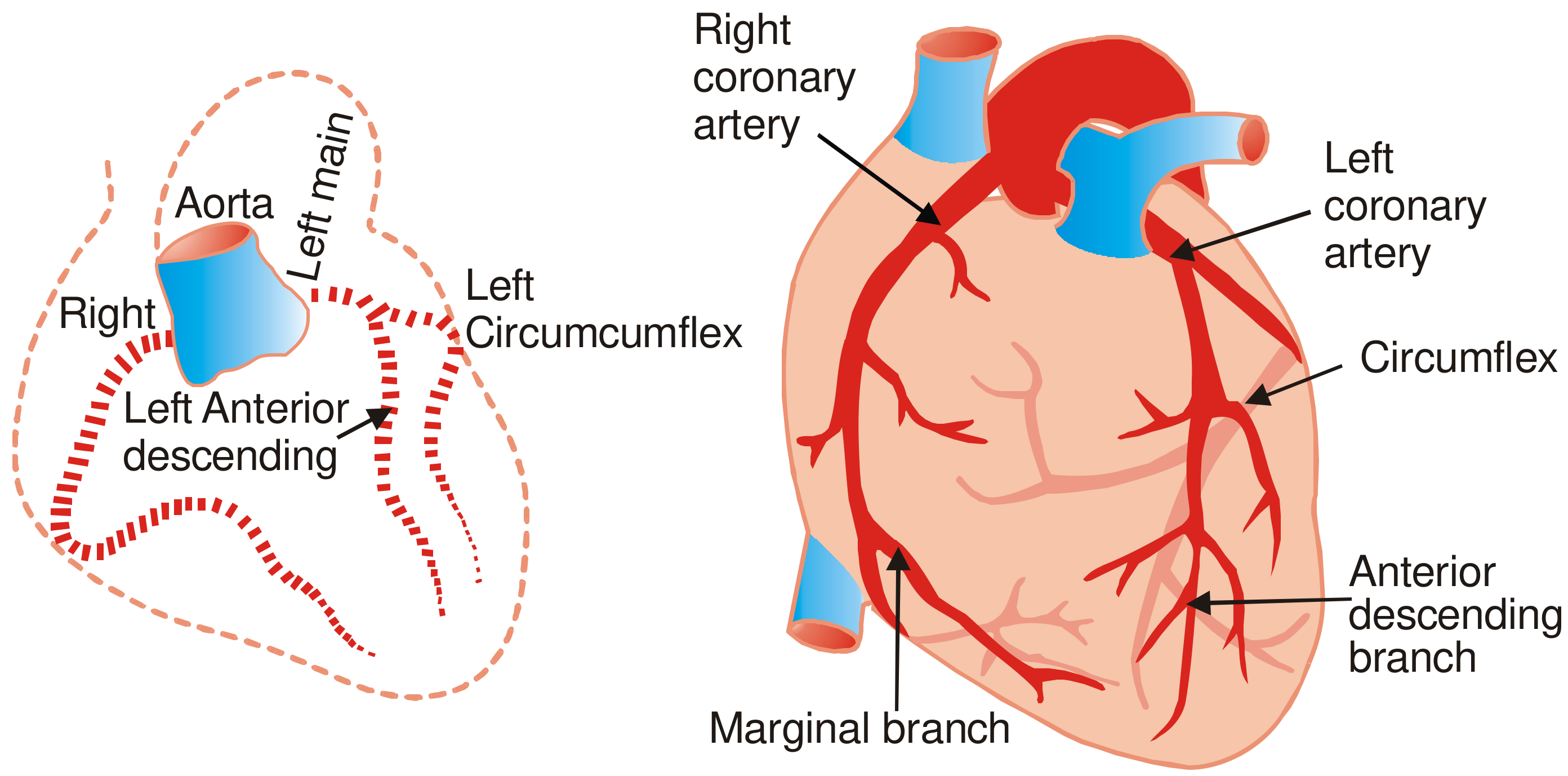
Diagram - Blood Supply Overview
Venous Drainage
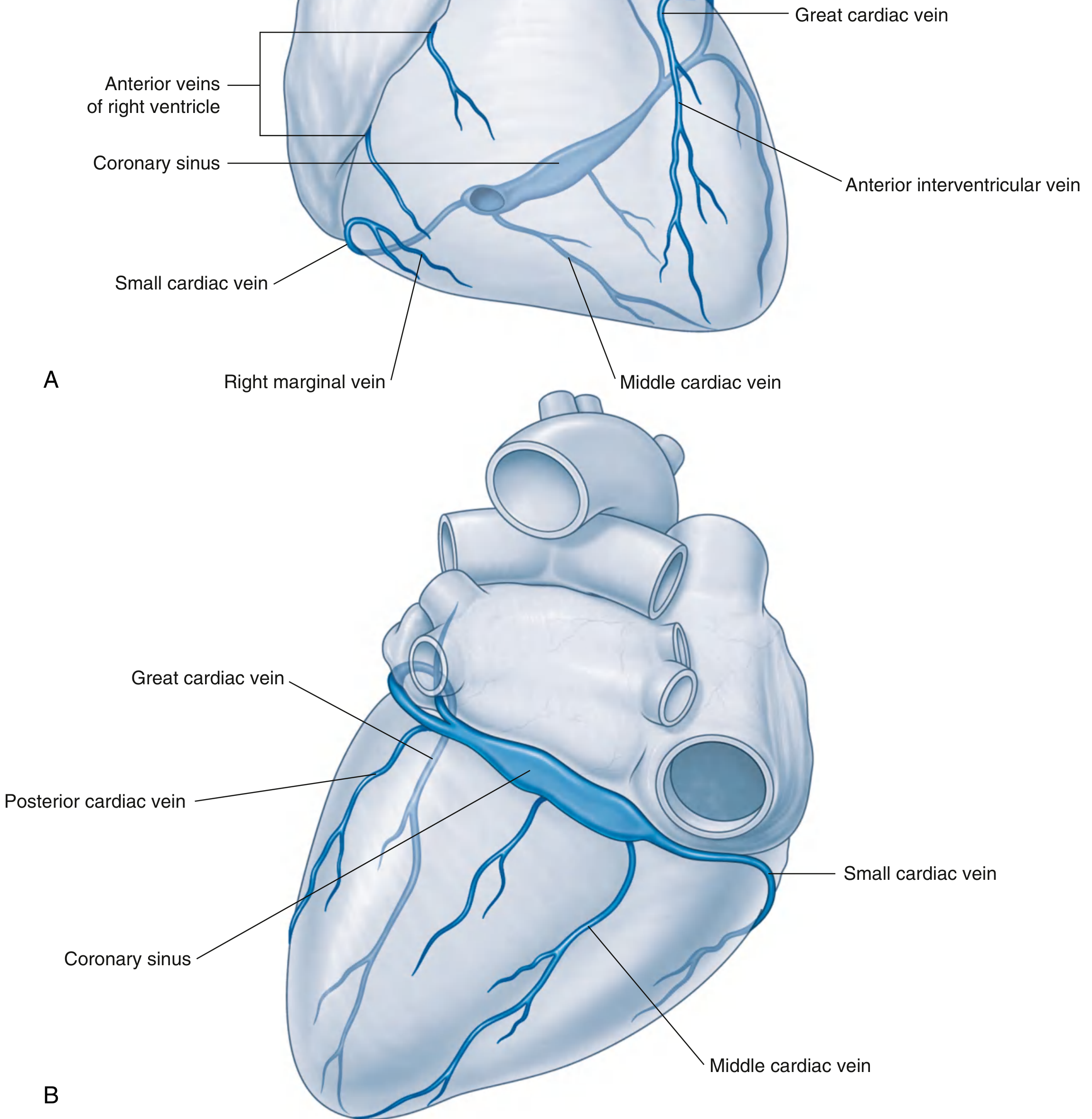
Most venous blood (~75%) drains via the coronary sinus into the right atrium. The coronary sinus runs in the posterior coronary sulcus and receives:
| Vein | Drains | Notes |
|---|---|---|
| Great cardiac vein | Anterior interventricular vein; runs alongside LAD, then in left AV sulcus | Main tributary of coronary sinus |
| Middle cardiac vein | Posterior interventricular sulcus (with PDA) | Enters coronary sinus near its opening |
| Small cardiac vein | Right atrium and right ventricle | Runs alongside right marginal artery |
| Posterior cardiac vein | Posterior left ventricle | Enters coronary sinus or great cardiac vein |
| Anterior cardiac veins | Anterior right ventricle | Drain directly into right atrium (bypass coronary sinus) |
| Thebesian veins (venae cordis minimae) | Myocardium | Drain directly into all cardiac chambers; most numerous in right side |
Coronary Perfusion - Key Physiology
- Left ventricle is perfused almost entirely during diastole - intramyocardial pressure during systole nearly occludes intramural vessels.
- Right ventricle is perfused during both systole and diastole (lower wall pressure).
- Coronary perfusion pressure = Aortic diastolic pressure - Left ventricular end-diastolic pressure (LVEDP).
- The endocardium is most vulnerable to ischemia (highest wall tension, last to be perfused).
Frequency of Coronary Stenosis
The most common sites of fatal coronary stenosis/thrombosis:
- LAD (anterior interventricular) - 45-64%
- RCA (right main) - 24-46%
- Left circumflex - 3-10%
- Left main - 0-10%
Right marginal and posterior interventricular branches are relatively spared.
Lymphatic Drainage
Cardiac lymphatics follow the coronary arteries and drain mainly into:
- Brachiocephalic nodes (anterior to the brachiocephalic veins)
- Tracheobronchial nodes (at the inferior end of the trachea)
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 679-680 | Gray's Anatomy for Students, p. 238-246 | P.C. Dikshit Textbook of Forensic Medicine & Toxicology, p. 155
This is a shared conversation. Sign in to Orris to start your own chat.