Spinal anaesthesia differential blockade
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Spinal Anaesthesia - Differential Blockade
Differential blockade is the phenomenon whereby different types of nerve fibers are blocked at different concentrations and to different dermatomal extents during spinal (and neuraxial) anaesthesia. It is one of the most clinically relevant concepts in regional anaesthesia practice.
Definition
When a local anaesthetic is injected intrathecally, not all nerve functions are abolished simultaneously or at the same spinal level. The susceptibility to blockade varies among fibre types, producing a characteristic "staircase" pattern of block that ascends cephalad in the order: autonomic > sensory > motor.
Nerve Fibre Classification and Susceptibility
| Fibre Type | Function | Diameter | Myelination | Susceptibility to Block |
|---|---|---|---|---|
| B fibres (preganglionic sympathetic) | Vasomotor, sudomotor | < 3 µm | Lightly myelinated | Most sensitive (blocked first) |
| Aδ fibres | Sharp pain, temperature, touch | 1-4 µm | Myelinated | Sensitive |
| C fibres | Dull/burning pain, temperature | 0.2-1.5 µm | Unmyelinated | Intermediate |
| Aβ fibres | Light touch, pressure, proprioception | 6-12 µm | Myelinated | Less sensitive |
| Aγ fibres | Muscle spindle tone | 4-8 µm | Myelinated | Less sensitive |
| Aα fibres | Somatic motor, proprioception | 12-20 µm | Heavily myelinated | Least sensitive (blocked last) |
Sympathetic preganglionic B fibres are small and lightly myelinated - they are blocked by the lowest concentrations of local anaesthetic. Large Aα motor fibres require the highest concentrations.
The Classic Segment Differential
The hallmark of spinal differential blockade is the segmental offset between levels of different modalities:
- Sympathetic block (assessed by skin temperature change or loss of sudomotor activity) extends up to 6 spinal segments cephalad beyond the upper limit of sensory block
- Analgesia (pinprick/sharp sensation loss) extends 2 or more segments cephalad beyond anaesthesia (loss of light touch)
- Motor block is the most caudal - typically 1-2 segments below the sensory level
So the complete picture from highest to lowest dermatomal level is:
Sympathetic block (most cephalad)
↓ ~2–6 segments
Analgesia (pinprick)
↓ ~2 segments
Anaesthesia (light touch)
↓ ~1–2 segments
Motor block (most caudal)
As stated in Morgan & Mikhail's Clinical Anesthesiology (7e): "Differential blockade typically results in sympathetic blockade (judged by temperature sensitivity) that may be two segments or more cephalad than the sensory block (pain, light touch), which, in turn, is usually several segments more cephalad than the motor blockade."
Mechanisms of Differential Blockade
1. The Size Principle (Classical Explanation)
Historically, differential blockade was attributed purely to nerve fibre diameter - smaller fibres are blocked at lower drug concentrations than larger fibres. This is because:
- Smaller fibres have a shorter critical length for conduction block
- A smaller cross-sectional area means local anaesthetic can penetrate more easily
2. Limitations of the Simple Size Principle
However, the size principle alone is not sufficient to explain all observations. Notably:
- Aδ fibres (sharp pain, myelinated, 1-4 µm) are preferentially blocked over C fibres (dull pain, unmyelinated, 0.2-1.5 µm) despite C fibres being smaller
- Within C fibres, fast and slow conduction components show distinct drug susceptibilities
- These discrepancies argue against a purely pharmacokinetic/size-based mechanism
3. Decremental Conduction Block
A critical additional mechanism is the critical length concept (Fink's decremental conduction model): A sufficient length of axon must be exposed to local anaesthetic to suppress impulse regeneration. Action potentials travel by passive electrotonic spread along nerve membrane. As this depolarisation decays with distance, the presence of local anaesthetic prevents adjacent nodes of Ranvier from regenerating the impulse - transmission stops when depolarisation falls below the threshold for action potential generation. If the exposed length is too short, the action potential can "skip" over blocked segments and resume conduction.
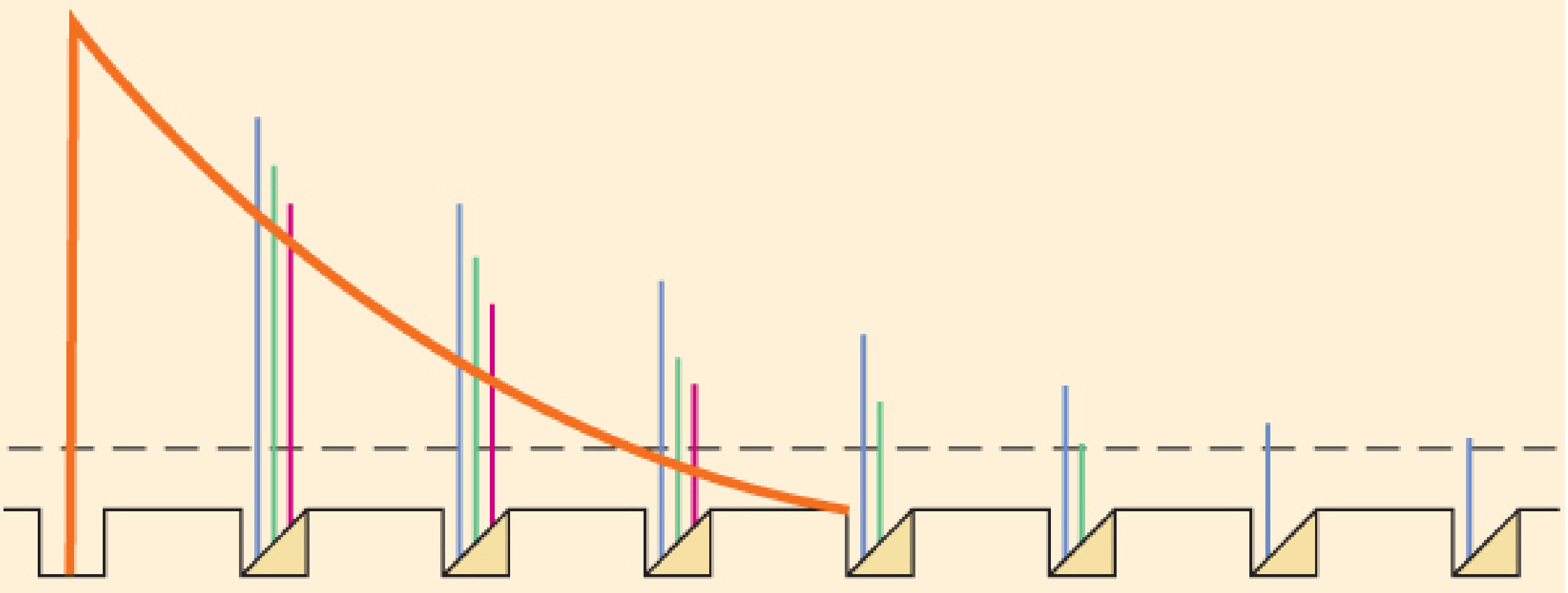
This diagram illustrates how action potential amplitudes (coloured vertical bars) decrease at successive nodes of Ranvier exposed to local anaesthetic (red curve = drug concentration gradient). Propagation fails when amplitude falls below threshold (dashed line). Even sub-blocking concentrations at multiple nodes can cumulatively extinguish conduction.
4. Sodium Channel Isoform Expression
More recent evidence implicates differential expression of sodium channel isoforms:
- NaV 1.7 and NaV 1.8 are highly expressed on dorsal root ganglia and show distinct sensitivities to lidocaine
- Intrinsic differences in channel kinetics and distribution contribute to different blocking characteristics independent of fibre size
5. Pattern of Stimulation (Use-Dependent Block)
Repetitive stimulation (use-dependent block) increases conduction failure at a given drug concentration compared to tonic stimulation. Fibres with higher physiological firing frequencies (like pain fibres during nociception) are thus more susceptible.
Clinical Implications
Sympathetic Block - Cardiovascular Effects
Since sympathetic B fibres are blocked most easily and over the widest segmental range:
- Vasomotor tone (primarily T5-L1 sympathetics) is disrupted, causing venodilation and venous pooling in the lower extremities and viscera
- Arterial vasodilation also reduces SVR
- Cardiac accelerator fibres (T1-T4) - when blocked in high spinal - cause bradycardia
- Combined vasodilation + reduced venous return + possible bradycardia = hypotension (the most common serious complication)
- Unopposed vagal tone can cause profound bradycardia or even cardiac arrest
Sympathetic Block vs Epidural - Key Difference
Unlike spinal anaesthesia, epidural anaesthesia produces no differential zone of sympathetic blockade - the level of sympathetic block corresponds closely with the sensory level. This is because the drug concentration gradient in epidural anaesthesia is different; in spinal anaesthesia, dilution of local anaesthetic in CSF as it spreads cephalad means the more peripherally-located (and susceptible) sympathetic fibres continue to be affected at low concentrations while the central motor fibres are not.
Testing Block Levels
Because each modality is blocked at a different level, clinicians use different tests to assess them:
- Sympathetic block: skin temperature sensation (cold spray/ice), sudomotor function, laser Doppler
- Sensory block: pinprick (Aδ) vs. light touch (Aβ) - these differ by ~2 segments
- Motor block: Bromage scale (Aα fibres)
Sequence of Block Onset and Recovery
The order of onset follows susceptibility (sympathetic first, motor last), and recovery follows the reverse order (motor recovers first, sympathetic tone returns last).
Differential Block and Epidural Analgesia
Differential blockade is actively exploited clinically in labour epidural analgesia - by using low concentrations of local anaesthetic, it is possible to produce sympathetic and fine sensory (Aδ/C) blockade while largely preserving motor function (Aα), allowing the parturient to remain mobile ("walking epidural").
Summary Table
| Feature | Sympathetic (B) | Sensory Aδ/C | Sensory Aβ | Motor (Aα) |
|---|---|---|---|---|
| Fibre size | Smallest | Small | Medium | Largest |
| Sensitivity to LA | Highest | High | Moderate | Lowest |
| Block level in spinal | Most cephalad | +2–6 below sympathetic | ~2 below Aδ | Most caudal |
| Assessed by | Temperature, skin colour | Pinprick | Light touch | Bromage scale |
| Recovery order | Last | Before sympathetic | Earlier | First |
Sources:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Differential Nerve Block, Mechanism of Nerve Blockade (pp. 1686-1687, 2853)
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Somatic Blockade, Autonomic Blockade (pp. 1801-1802)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Physiological Effects of Spinal Anesthesia (p. 519)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - Activity Profile During Neuronal Blockade
This is a shared conversation. Sign in to Orris to start your own chat.