Klippel feil syndrome definition eloborate etiology signs and symptoms and investigations and evaluation treatment in complete details and with illustrative diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
Klippel-Feil syndrome definition etiology signs symptoms investigations treatment complete
Searching Images
Klippel-Feil syndrome cervical vertebrae fusion X-ray
Reading File
Reading File
Reading File
Reading File
Searching Images
Klippel-Feil syndrome short neck low hairline clinical photo
Reading File
Finding Sources
Searching PubMed
"Klippel-Feil syndrome" management treatment
Searching Images
Klippel-Feil syndrome MRI syringomyelia Chiari malformation spinal cord
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative textbooks and excellent clinical images. Let me compile the complete, detailed response.
Klippel-Feil Syndrome (KFS) — Complete Clinical Review
1. Definition
Klippel-Feil syndrome (KFS), also called brevicollis, is a congenital condition characterized by the fusion (synostosis) of two or more cervical vertebrae due to failure of normal segmentation of the cervical somites during embryonic development. It was first described by Maurice Klippel and André Feil in 1912.
The hallmark is the classic clinical triad:
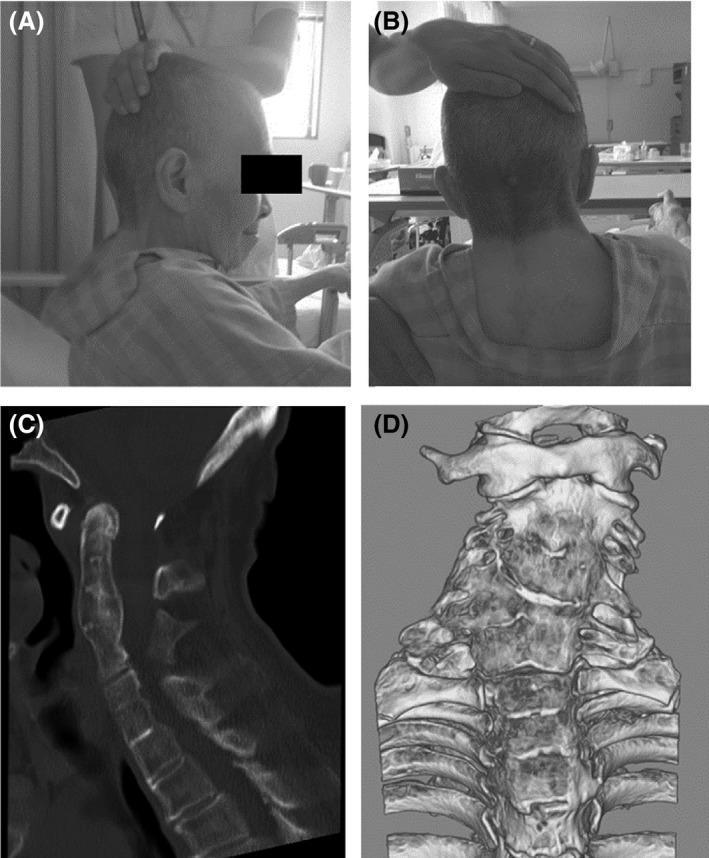
- Short neck (brevicollis)
- Low posterior hairline
- Limited range of cervical motion
⚠️ The complete triad is present in fewer than 50% of patients. Many patients have subtle findings and are diagnosed incidentally on imaging.
— Miller's Review of Orthopaedics 9th Ed.; Bradley and Daroff's Neurology in Clinical Practice
2. Epidemiology
- Incidence: approximately 1 in 40,000–42,000 live births
- Slight female predominance (as noted in Wildervanck/KFS association)
- Can occur sporadically (most cases) or as a familial condition
- Associated with multiple other congenital anomalies (multisystem disorder)
3. Etiology & Pathogenesis
Embryological Basis
KFS results from failure of normal segmentation or formation of cervical somites during weeks 3–8 of gestation — the critical window for cervical vertebral development.
Normally, the somites segment and differentiate into individual cervical vertebrae. In KFS, this process is disrupted, causing adjacent vertebral bodies to fuse into a "block vertebra."
The Developing Human (Clinically Oriented Embryology) describes the pathology:
"In most cases, the reduced number of cervical vertebral bodies results from fusion of vertebrae before birth. In some cases, there is a lack of segmentation of several elements of the cervical region of the vertebral column. The number of cervical nerve roots may be normal, but they are small, as are the intervertebral foramina."
Genetic Basis
- GDF6 gene (growth differentiation factor 6) on chromosome 8 — involved in somite segmentation; mutations cause autosomal dominant KFS
- GDF3 gene — associated with additional vertebral fusions
- MEOX1 gene — autosomal recessive form; associated with more severe phenotype
- TBX6 gene variants — associated with congenital vertebral anomalies
- SGMI gene on chromosome 8 has also been cited (Miller's Review of Orthopaedics)
- Most sporadic cases are idiopathic; familial cases follow autosomal dominant or autosomal recessive inheritance
Classification (Feil Classification)
| Type | Description |
|---|---|
| Type I | Massive fusion of many or all cervical and upper thoracic vertebrae into a single block |
| Type II | Fusion of one or two pairs of cervical vertebrae (most common type) |
| Type III | Type I or II with additional thoracic or lumbar vertebral fusions |
4. Clinical Features — Signs & Symptoms
The Classic Triad (present in <50% of cases)

Musculoskeletal / Cervical Symptoms
| Feature | Details |
|---|---|
| Short neck | Due to reduced number of mobile vertebral segments |
| Low posterior hairline | Hairline extends toward the shoulders |
| Limited cervical ROM | Restricted flexion, extension, rotation |
| Neck pain | Common; from stress on hypermobile adjacent segments |
| Torticollis | Wry neck deformity; may be the presenting symptom in children |
| Pterygium colli | Neck webbing (soft tissue); superficially resembles Turner syndrome |
| Sprengel deformity | Congenitally elevated scapula; present in ~30% of KFS cases |
| Congenital scoliosis | Lateral curvature of the thoracolumbar spine |
| Cervical ribs | Predispose to thoracic outlet syndrome |
Neurological Symptoms
KFS causes neurological compromise through:
- Direct nerve root compression (narrowed intervertebral foramina)
- Cervical spinal cord compression (stenosis, hypermobile adjacent segments)
- Vertebral or spinal artery compression
- Associated Chiari I malformation → secondary syringomyelia/syringobulbia
- Atlantoaxial instability → cord compression by dens
| Neurological Feature | Notes |
|---|---|
| Mirror movements (synkinesia) | Most characteristic of KFS — involuntary mimicking of voluntary hand movements in the contralateral hand; caused by abnormal decussation at cervicomedullary junction |
| Myelopathy | Spasticity, hyperreflexia, weakness from cord compression |
| Radiculopathy | Dermatomal pain, paresthesia, weakness |
| Hearing loss | Most common cranial nerve symptom; sensorineural +/− conductive |
| Hydrocephalus | From associated Chiari malformation |
| Syringomyelia / syringobulbia | Central cord cavitation; presents with cape-like sensory loss |
| Headache / occipital neuralgia | From upper cervical nerve root compression |
"Klippel-Feil syndrome is the anomaly most likely to cause mirror movements (synkinesia), particularly of the hands." — Bradley and Daroff's Neurology in Clinical Practice
Associated Anomalies (Multisystem)
| System | Anomaly | Frequency |
|---|---|---|
| Renal | Renal aplasia/agenesis, horseshoe kidney, duplicated collecting system | ~33% |
| Auditory | Sensorineural deafness, middle ear anomalies, external auditory canal atresia | ~30% |
| Musculoskeletal | Sprengel deformity, congenital scoliosis | ~30% |
| Cardiac | ASD, VSD, coarctation of the aorta | 14–29% |
| Neurological | Brainstem abnormalities, syringomyelia, Chiari I | Variable |
| Spinal cord | Diastematomyelia (split cord), tethered cord | Variable |
| ENT | Hearing loss, branchial arch anomalies | Common |
| Ocular | Duane retraction syndrome (Wildervanck syndrome) | Subset |
5. Investigations & Evaluation
Step 1: Plain Radiographs (First-line)
AP and Lateral cervical spine X-rays are the initial investigation confirming the diagnosis.
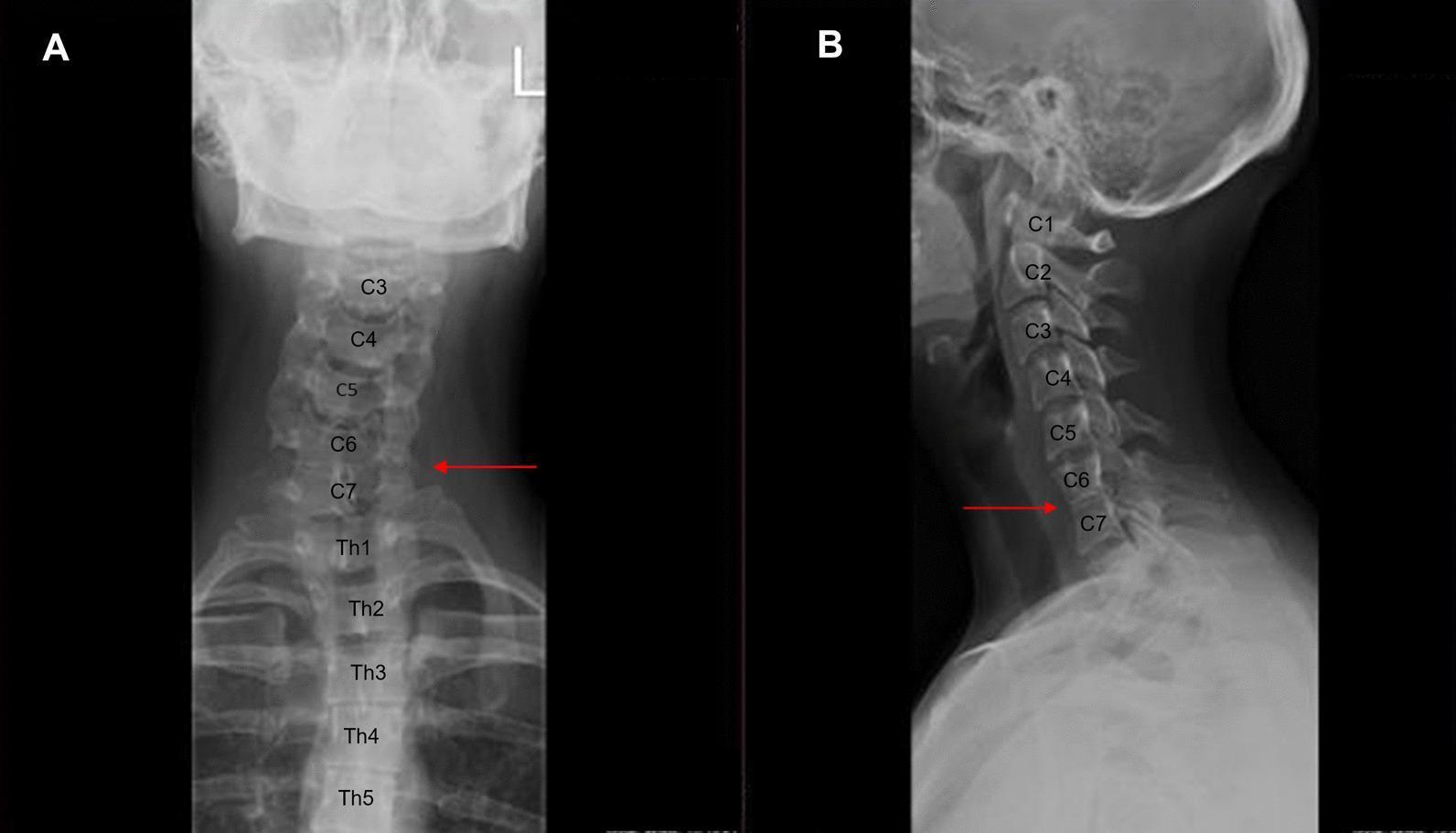

Radiographic findings include:
- Block vertebrae — absent disc spaces, vertebral bodies fused
- Reduced height of the cervical spine
- Hypermobility at non-fused ("transitional") segments — compensatory
- Atlanto-occipital assimilation in some cases
- Assess for: Atlantoaxial instability (ADI >3 mm in adults, >5 mm in children)
Step 2: CT Scan
CT with 3D reconstruction provides superior bony detail:
- Delineates extent of vertebral fusions precisely
- Identifies posterior element fusion, facet fusion
- Assesses foramen magnum, Atlantoaxial joint
- Invaluable for surgical planning
Dynamic CT (neutral + maximal rotation): Used to diagnose atlantoaxial rotatory displacement
Step 3: MRI (Mandatory)
MRI of the entire cervical and thoracic spine is mandatory in all KFS patients to rule out intraspinal pathology.

MRI reveals:
- Syringomyelia — central cord cavitation (T2 bright)
- Chiari I malformation — tonsillar herniation below foramen magnum
- Cord compression — at fused or hypermobile levels
- Diastematomyelia (split cord)
- Intraspinal tumors, lipomas
- Tethered cord
- Mirror movement anatomy — abnormal clefts/division at cervicomedullary junction
Step 4: Additional Investigations
| Investigation | Purpose |
|---|---|
| Renal ultrasound | Screen all patients for renal agenesis/dysplasia (33% prevalence) |
| Cardiac echocardiography | Congenital heart defect screening (14–29%) |
| Audiometry / BAER | Sensorineural or conductive hearing loss (30%) |
| Flexion-extension radiographs | Assess instability at non-fused segments |
| Scoliosis series (standing AP + lateral) | Evaluate thoracolumbar scoliosis |
| Genetic testing | GDF6, GDF3, MEOX1 mutations in familial cases |
| Ophthalmology referral | Screen for Duane syndrome (especially female patients) |
6. Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Turner syndrome | Web neck + 45,X karyotype; no cervical fusion on X-ray |
| Noonan syndrome | Web neck + normal karyotype; RAS pathway mutations |
| Juvenile idiopathic arthritis | Acquired cervical fusion with inflammatory markers |
| Ankylosing spondylitis | Bamboo spine; sacroiliac involvement; HLA-B27 |
| Torticollis (isolated) | No vertebral fusion; resolves with physiotherapy |
| Wildervanck syndrome | KFS + Duane syndrome + deafness (female-predominant) |
7. Treatment
Treatment is individualized based on the severity of fusion, neurological involvement, and associated anomalies.
Conservative (Non-operative) Management
Indications: Asymptomatic or mildly symptomatic patients
| Intervention | Details |
|---|---|
| Activity restriction | Avoid collision sports with multilevel fusion, C2 involvement, or limited cervical ROM |
| Cervical orthosis | Collar or brace for neck pain; protective during participation in permitted activities |
| Physical therapy | Muscle strengthening, posture correction, stretching within safe ROM limits |
| NSAIDs / analgesics | Neck pain management |
| Hearing aids | For sensorineural hearing loss |
| Regular surveillance | Serial neurological exams, repeat MRI if new symptoms develop |
Surgical Management
Indications for Surgery:
- Chronic myelopathy (spinal cord compression causing neurological deficits)
- Cervical cord compression from instability or stenosis that is progressive or severe
- Syringomyelia with neurological deterioration → posterior fossa decompression
- Chiari I malformation causing symptoms → foramen magnum decompression
- Atlantoaxial instability with ADI >10 mm or neurological signs → posterior C1–C2 fusion
- Progressive scoliosis >25–30° with adequate pulmonary reserve → spinal fusion
| Surgical Procedure | Indication |
|---|---|
| Posterior cervical fusion | Instability; myelopathy from unstable segments |
| Anterior cervical discectomy and fusion (ACDF) | Herniation or stenosis at mobile adjacent levels |
| Foramen magnum decompression | Chiari I with syringomyelia |
| Atlantoaxial fusion (C1–C2) | Atlantoaxial instability with neurological signs |
| Scapuloplasty/Woodward procedure | Sprengel deformity (cosmetic + functional) |
| Scoliosis correction | Progressive curves in growing children |
Treatment Decision Flowchart (Summarized)
KFS Diagnosed
│
├─ Asymptomatic ──────────────► Surveillance + Activity restriction
│
├─ Pain only ─────────────────► NSAIDs, PT, orthosis
│
├─ Neurological symptoms ─────► MRI mandatory
│ │
│ ├─ Syringomyelia/Chiari ► Posterior fossa decompression
│ ├─ Cord compression ───► Cervical decompression ± fusion
│ └─ Instability ────────► Fusion (C1–C2 or subaxial)
│
└─ Associated anomalies ──────► Treat each system independently
(cardiac, renal, hearing)
8. Prognosis & Complications
- Without neurological involvement: excellent prognosis; many patients live normal lives
- Hypermobile adjacent segments carry risk of accelerated degenerative disc disease and post-traumatic cord injury from minor trauma
- Myelopathy, once established, may not fully reverse after decompression
- Mirror movements do not reliably improve with treatment
- Long-term follow-up is essential given the risk of progressive instability at non-fused levels
Summary Table
| Feature | Key Points |
|---|---|
| Definition | Congenital fusion of ≥2 cervical vertebrae |
| Embryology | Failure of somite segmentation, weeks 3–8 |
| Genetics | GDF6, GDF3, MEOX1; AD or AR; mostly sporadic |
| Classic triad | Short neck, low hairline, limited cervical ROM (<50% have all three) |
| Most characteristic sign | Mirror movements (synkinesia) of hands |
| Most common cranial nerve sx | Hearing loss |
| Key association | Sprengel deformity (30%), renal anomalies (33%), cardiac defects (14–29%) |
| First-line imaging | Cervical X-ray (AP + lateral) |
| Mandatory investigation | MRI whole spine (rule out syringomyelia, Chiari, cord compression) |
| Medical treatment | Activity restriction, NSAIDs, PT, orthosis |
| Surgery | For myelopathy, instability, Chiari/syringomyelia, scoliosis |
Sources:
- Miller's Review of Orthopaedics, 9th Edition
- Bradley and Daroff's Neurology in Clinical Practice
- The Developing Human: Clinically Oriented Embryology
- K.J. Lee's Essential Otolaryngology
- Goldman-Cecil Medicine
- Recent review: Cardiovascular Findings in KFS — Niewchas et al., Cureus 2024 [PMID: 39610582]
This is a shared conversation. Sign in to Orris to start your own chat.