UTI in male
Reading File
Finding Sources
Finding Sources
Searching PubMed
"urinary tract infection" AND male
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have enough content to provide a comprehensive, well-structured answer on UTI in males. Let me synthesize the findings.
Urinary Tract Infection (UTI) in Males
Why It's Always "Complicated"
UTI in males is by definition a complicated UTI. Male sex is itself a risk factor listed in complicating factors because men have a much longer urethra, making ascending infection inherently less likely — so when a UTI does occur in a man, an underlying anatomic or functional abnormality must be suspected.
"Suspect underlying anatomic abnormality in men with culture-proven UTI." — Tintinalli's Emergency Medicine
Epidemiology
- UTIs are far less common in men than women due to the longer male urethra
- In young men (<35 years), dysuria is more commonly secondary to a sexually transmitted infection (STI) — chlamydia or gonorrhea — rather than a true UTI
- Incidence rises significantly after age 50 due to benign prostatic hyperplasia (BPH) causing bladder outlet obstruction and incomplete bladder emptying
- A post-void residual volume >180 mL predisposes to bacteriuria in men
Pathophysiology
Routes of Infection
- Ascending (most common) — uropathogenic bacteria from the bowel/perianal skin colonize the urethra and ascend to the bladder. Bacteria possess adhesins, pili, and fimbriae that allow attachment to urothelium.
- Hematogenous — uncommon; seen with S. aureus bacteremia or candidemia; facilitated by obstruction
- Lymphatic — rare; may occur from severe bowel infection or retroperitoneal abscess
Risk Factors / Complicating Factors in Males
| Factor | Significance |
|---|---|
| Male sex | Longer urethra provides protection; infection suggests underlying abnormality |
| BPH / bladder outlet obstruction | High post-void residual → stasis → infection |
| Renal calculi / obstruction | Impairs ureteral peristalsis; raises intrapelvic pressure |
| Instrumentation / catheterization | Disrupts mucosal defense; introduces organisms |
| Immunosuppression (diabetes, HIV, transplant) | Reduces host defenses |
| Structural abnormality | Neurogenic bladder, urethral stricture, vesicoureteral reflux |
| Recent antibiotic use | Selects resistant organisms |
| Indwelling urinary catheter | CAUTI; organisms form biofilm; polymicrobial |
| Hospital acquisition | More resistant organisms |
— Campbell Walsh Wein Urology, Box 55.1
Microbiology
| UTI Type | Common Organisms |
|---|---|
| Community-acquired | E. coli (dominant), Klebsiella pneumoniae, Proteus mirabilis, Enterococcus faecalis |
| Complicated / Male UTI | E. coli, Enterococcus spp., Klebsiella, Pseudomonas aeruginosa, S. aureus, Candida spp. |
| Catheter-associated | Polymicrobial; E. coli, Enterococcus, coagulase-negative Staphylococcus, Candida, Pseudomonas, Proteus, Morganella |
Extended-spectrum β-lactamase (ESBL)-producing E. coli is an emerging problem (~4–6% of outpatient UTIs).
Clinical Presentation
Lower Tract (Cystitis / Prostatitis)
- Frequency, urgency, dysuria, hesitancy
- Suprapubic pain / tenderness
- Gross hematuria
- Perineal/rectal pain — consider prostatitis
- Urethral discharge in young men → think urethritis/STI, not UTI
Upper Tract (Pyelonephritis)
- Fever and chills
- Flank pain, costovertebral angle (CVA) tenderness
- Nausea, vomiting, systemic symptoms
- May coexist with or follow lower tract symptoms
Complicated/Atypical Presentations
- Fever, pain, and inflammatory response may be absent in patients with spinal cord injury, immunocompromise, or the elderly
- Sepsis from a urinary source accounts for ~10–19% of all sepsis cases
Diagnosis
Urinalysis
- Pyuria (WBCs in urine) — hallmark of infection/inflammation
- Bacteriuria without pyuria = likely colonization, not infection
- Positive leukocyte esterase and nitrite (gram-negatives only)
- Pyuria without bacteriuria ("sterile pyuria") — warrants further workup (TB, interstitial nephritis, etc.)
Urine Culture
- Required in all male UTIs (complicated UTI)
- Diagnostic threshold: ≥10⁵ CFU/mL (or ≥10³ CFU/mL in catheterized specimen with symptoms)
- Obtain before starting antibiotics
Blood Cultures
- Indicated when sepsis is suspected
- Positive in up to 40% of admitted pyelonephritis; organism matches urine in 97%
Imaging
Indicated in males, diabetics, elderly, immunocompromised, and those failing treatment:
- Ultrasound — first-line; evaluates obstruction, post-void residual, focal parenchymal lesions
- CT (non-contrast/contrast) — best for stones, emphysematous pyelonephritis, renal abscess
- Plain radiography has poor sensitivity for intrarenal gas
Treatment
Antibiotic Therapy (Complicated UTI / Male UTI)
| Clinical Scenario | Preferred Regimen | Duration |
|---|---|---|
| Outpatient (low severity) | Fluoroquinolone (ciprofloxacin, levofloxacin) or TMP-SMX (if susceptible) | 7–14 days |
| Pyelonephritis (outpatient) | Ciprofloxacin 500 mg BID or levofloxacin 750 mg once daily | 7–10 days |
| Inpatient / Sepsis | IV fluoroquinolone, 3rd-gen cephalosporin, aminoglycoside, or piperacillin-tazobactam | Until afebrile 24–48h, then oral step-down |
| ESBL-suspected | Nitrofurantoin or fosfomycin (lower tract only); carbapenem for upper tract/systemic | Variable |
| Catheter-associated UTI | Treat only if symptomatic; remove/replace catheter; guided by culture | 7–14 days |
Note: Nitrofurantoin and fosfomycin are NOT appropriate for male UTI if pyelonephritis or prostatitis is suspected — they do not achieve adequate tissue levels.
Key Principles
- Always obtain a urine culture before starting antibiotics
- Investigate for underlying structural cause (post-void residual, ultrasound, cystoscopy)
- Evaluate prostate (PSA, digital rectal exam) if prostatitis suspected
- Evaluate for STI in men <35 years with dysuria (test for Chlamydia, N. gonorrhoeae)
- Fluoroquinolones are no longer recommended empirically for gonorrhea due to resistance
Differential Diagnosis in Males with Dysuria
| Condition | Distinguishing Features |
|---|---|
| Urethritis (STI) | Urethral discharge, new sexual partner, younger patient |
| Prostatitis (acute bacterial) | Fever, perineal pain, tender boggy prostate |
| Epididymo-orchitis | Scrotal pain/swelling, tenderness |
| BPH | Obstructive LUTS, middle-aged/older |
| Urethral stricture | Prior STI/instrumentation, poor stream |
| Bladder/prostate cancer | Painless hematuria, older age |
| Nephrolithiasis | Colicky flank/groin pain, hematuria |
Special Scenarios
Asymptomatic Bacteriuria in Males
- Prevalence ~30% in male nursing home residents and nearly universal in long-term catheterized patients
- Treatment NOT recommended unless:
- Pre-operative urologic procedure with mucosal bleeding anticipated
- (In women: also treat if pregnant)
Catheter-Associated UTI (CAUTI)
- Diagnosed: ≥10³ CFU/mL + symptoms, with no other source
- Best prevention: restrict catheterization to strict indications; remove catheter ASAP
- Long-term catheters (>30 days) — typically polymicrobial; resistance common
Recent Evidence
A 2024 WikiGuidelines consensus statement (PMID 39495518) in JAMA Network Open provides updated recommendations on UTI prevention, diagnosis, and management across all populations including males. A 2025 living systematic review/meta-analysis (PMID 40228579) in Clinical Microbiology and Infection examined short vs. long antibiotic courses for pyelonephritis and complicated UTI — findings relevant for optimizing treatment duration in male patients.
Key Takeaway: Any UTI in a male should trigger investigation for an underlying structural or functional urinary tract abnormality. Empiric fluoroquinolones (ciprofloxacin/levofloxacin) for 7–14 days are the mainstay of outpatient treatment; urine culture must guide definitive therapy. Prostatitis and STI must always be considered in the differential.
— Campbell Walsh Wein Urology | Tintinalli's Emergency Medicine | Comprehensive Clinical Nephrology
Teach me about urine routine test and each conponents
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
urine microscopy sediment casts cells routine examination
I have comprehensive content from all three textbooks. Now I'll compile a thorough, well-organized teaching response.
Urine Routine Examination (Urinalysis)
A urine routine test (urinalysis) is one of the most informative, cost-effective diagnostic tests in medicine. It consists of three components:
- Physical / Gross Examination
- Chemical (Dipstick) Analysis
- Microscopic Examination (Urine Sediment)
🧪 Part 1: Physical / Gross Examination
1. Color
Normal urine is pale to deep yellow from the pigment urochrome. Color reflects concentration and can reveal pathology.
| Color | Causes |
|---|---|
| Colorless | Overhydration, diabetes insipidus |
| Cloudy/milky | Phosphaturia (benign), pyuria, chyluria |
| Red/pink | Hematuria, hemoglobinuria, myoglobinuria; drugs (rifampin, phenothiazines); beets |
| Orange | Dehydration; phenazopyridine (Pyridium); sulfasalazine |
| Yellow | Normal; riboflavin; phenacetin |
| Green-blue | Biliverdin, methylene blue, amitriptyline, pseudomonal infection |
| Brown/cola | Old hematuria/glomerular bleeding; urobilinogen; porphyria; metronidazole; nitrofurantoin |
| Brown-black | Alkaptonuria (homogentisic acid); melanin; myoglobin |
"Brown or cola-colored urine can be a sign of glomerular bleeding and disease." — Campbell Walsh Wein Urology
2. Turbidity (Clarity)
- Normal: Clear to slightly hazy
- Cloudy: Most commonly phosphaturia (precipitates in alkaline urine → clears with acetic acid) or pyuria
- Rare: Chyluria, lipiduria, hyperoxaluria, hyperuricosuria
3. Odor
- Normal: Faint, aromatic
- Foul/pungent: UTI (bacterial metabolism)
- Sweet/fruity: Ketones (diabetic ketoacidosis, starvation)
- Musty/mousy: Phenylketonuria (PKU)
4. Volume
- Normal adult 24-hour output: 800–2,000 mL/day
- Oliguria: <400 mL/day (prerenal, renal, postrenal causes)
- Anuria: <100 mL/day (severe AKI, complete obstruction)
- Polyuria: >3,000 mL/day (diabetes insipidus, diabetes mellitus, excessive fluid intake)
🧫 Part 2: Chemical (Dipstick) Analysis
The dipstick detects 8–10 parameters simultaneously using colorimetric reagent pads.
1. Specific Gravity (SG)
| Parameter | Details |
|---|---|
| Normal range | 1.003 – 1.030 |
| Purpose | Reflects kidney concentrating ability; surrogate for urine osmolality |
| Isosthenuria | SG = 1.010 (urine osmolality = plasma osmolality) → loss of concentrating/diluting ability |
| ↑ SG | Dehydration, SIADH, glycosuria, proteinuria |
| ↓ SG | Overhydration, diabetes insipidus, renal tubular disease |
| Falsely elevated by | Glucose, high protein, iodine-based contrast, ketoacids |
2. pH
| Parameter | Details |
|---|---|
| Normal range | 4.5 – 8.0 (average: 5–6) |
| Purpose | Reflects renal tubular H⁺ secretion |
| Acidic urine (↓ pH) | High-protein diet, metabolic/respiratory acidosis, fever, starvation |
| Alkaline urine (↑ pH) | Vegetarian diet, UTI with urease-splitting organisms (Proteus, Klebsiella), renal tubular acidosis (RTA), metabolic alkalosis, vomiting |
| Clinical use | Alkaline urine + UTI → suspect struvite stone risk; persistent alkaline urine with acidosis → distal RTA |
3. Protein
| Parameter | Details |
|---|---|
| Normal | Negative (trace amounts <10 mg/dL not detected) |
| Dipstick scale | Trace, 1+ (~30 mg/dL), 2+ (~100 mg/dL), 3+ (~300 mg/dL), 4+ (~1000 mg/dL) |
| Confirms with | Spot urine protein-to-creatinine ratio (P:Cr) or 24-hour urine collection |
Types of proteinuria:
| Type | Mechanism | Examples |
|---|---|---|
| Glomerular | Damaged filtration barrier → albumin leaks | Nephrotic syndrome, diabetes, SLE |
| Tubular | Proximal tubules fail to reabsorb filtered proteins | ATIN, Fanconi syndrome, AKI, toxins |
| Overflow | Excessive plasma proteins overwhelm tubules | Myeloma (Bence Jones protein), myoglobinuria |
| Orthostatic | Occurs only when upright | Benign, young patients |
Note: Dipstick primarily detects albumin — it may miss Bence Jones proteins (light chains). A sulfosalicylic acid (SSA) test can detect non-albumin proteins.
Falsely positive: Alkaline urine, concentrated urine, contamination with antiseptics
Falsely negative: Very dilute urine, non-albumin proteins
Falsely negative: Very dilute urine, non-albumin proteins
4. Glucose
| Parameter | Details |
|---|---|
| Normal | Negative |
| Detected when | Plasma glucose exceeds renal threshold (~180 mg/dL) |
| Causes of glycosuria | Diabetes mellitus (most common), pregnancy, Fanconi syndrome (tubular glucosuria with normal blood glucose) |
| Falsely positive | Ascorbic acid interference (varies by brand) |
Key teaching point: Glucosuria with normal serum glucose = proximal tubular dysfunction (Fanconi syndrome)
5. Ketones
| Parameter | Details |
|---|---|
| Normal | Negative |
| Detected ketones | Acetoacetate and acetone (NOT β-hydroxybutyrate) |
| Causes | DKA, starvation/fasting, alcoholic ketoacidosis, prolonged vomiting, low-carb diet |
| Clinical use | Strongly positive ketones + glycosuria = DKA until proven otherwise |
6. Blood (Heme)
| Parameter | Details |
|---|---|
| Normal | Negative |
| Detects | Intact RBCs, free hemoglobin, myoglobin (all turn dipstick positive) |
| Positive dipstick + RBCs on microscopy | True hematuria |
| Positive dipstick + NO RBCs on microscopy | Hemoglobinuria or myoglobinuria |
Causes of hematuria:
- Glomerular: Cola/brown urine, dysmorphic RBCs, RBC casts → IgA nephropathy, GN
- Non-glomerular: Bright red, normal RBCs → UTI, stones, tumor, trauma, BPH, prostatitis
7. Leukocyte Esterase (LE)
| Parameter | Details |
|---|---|
| Normal | Negative |
| Significance | Enzyme released by neutrophils → proxy for pyuria |
| Positive | UTI, urethritis, pyelonephritis, ATIN, TB |
| Sterile pyuria (LE+ but no organisms on culture) | Suspect ATIN, TB, chlamydial urethritis, genitourinary TB, renal papillary necrosis |
| Falsely negative | Very dilute urine, glycosuria, elevated urobilinogen, vitamin C |
8. Nitrite
| Parameter | Details |
|---|---|
| Normal | Negative |
| Principle | Certain bacteria (gram-negatives) convert dietary nitrates → nitrites |
| Positive suggests | Gram-negative bacteriuria: E. coli, Klebsiella, Proteus |
| Negative nitrite does NOT rule out UTI | Gram-positives (Enterococcus, Staph saprophyticus), Pseudomonas, fungi do NOT produce nitrite |
| Requires | Urine in bladder ≥4 hours (incubation time); first morning specimen most reliable |
| Combined LE + Nitrite positive | High predictive value for UTI |
9. Bilirubin
| Parameter | Details |
|---|---|
| Normal | Negative |
| Type detected | Conjugated (direct) bilirubin only — water-soluble, filtered by kidney |
| Positive | Hepatocellular disease, obstructive jaundice (biliary obstruction) |
| NOT detected in | Pre-hepatic jaundice (hemolysis) — unconjugated bilirubin is albumin-bound, not filtered |
10. Urobilinogen
| Parameter | Details |
|---|---|
| Normal | Trace amounts (0.1–1.0 EU/dL) — normally reabsorbed from gut, re-excreted in urine |
| ↑ Urobilinogen | Hemolytic anemia, hepatocellular disease (liver cannot re-cycle it) |
| ↓ / Absent urobilinogen | Complete biliary obstruction (no bile reaching gut → no urobilinogen formed) |
| Tip | Bilirubinuria + normal/↑ urobilinogen = hepatocellular disease; Bilirubinuria + absent urobilinogen = obstructive jaundice |
🔬 Part 3: Microscopic Examination (Urine Sediment)
Urine is centrifuged and the sediment is examined under a microscope. This is the most informative part of urinalysis.
A. Red Blood Cells (RBCs)
- Normal: 0–2 RBCs/HPF (high-power field)
- Hematuria: ≥3 RBCs/HPF (AUA definition)
- Dysmorphic RBCs (acanthocytes, "mickey-mouse" cells) → glomerular source → GN
- Isomorphic (normal) RBCs → lower urinary tract (bladder, urethra, prostate)
- RBC casts = definitive evidence of glomerulonephritis
B. White Blood Cells (WBCs / Leukocytes)
- Normal: 0–5 WBCs/HPF
- Pyuria: >5 WBCs/HPF
- Causes: UTI (most common), pyelonephritis, urethritis, ATIN, TB
- WBC casts → pyelonephritis or ATIN (infection/inflammation involving tubules)
- Eosinophils in urine (Hansel stain) → acute interstitial nephritis (ATIN) (though sensitivity limited)
C. Epithelial Cells
| Type | Origin | Significance |
|---|---|---|
| Squamous epithelial cells | Urethra / vagina / skin | Indicate contamination; specimen should be repeated |
| Transitional (urothelial) cells | Bladder / ureter / renal pelvis | Few are normal; many → catheter trauma, or if atypical → malignancy |
| Renal tubular epithelial cells (RTECs) | Proximal/distal tubules | Significant — indicate tubular injury (AKI, ATN, nephrotoxins, transplant rejection) |
D. Casts
Casts are cylindrical structures formed from Tamm-Horsfall (uromodulin) protein in the tubular lumen. Their contents reveal the type of injury.
| Cast Type | Appearance | Clinical Significance |
|---|---|---|
| Hyaline casts | Clear, homogeneous | Non-specific; seen in normal concentrated urine, fever, exercise, mild dehydration |
| RBC casts | Red-orange, granular | Glomerulonephritis (pathognomonic) |
| WBC casts | Pale, contain WBCs | Pyelonephritis or ATIN |
| Granular casts | Coarse or fine granules | Tubular cell debris — seen in AKI |
| "Muddy brown" granular casts | Dark, brownish | Acute tubular necrosis (ATN) — highly specific |
| Waxy casts | Broad, waxy, sharp edges | Advanced chronic kidney disease (CKD), slow tubular flow |
| Fatty casts | Lipid droplets ("Maltese cross" under polarized light) | Nephrotic syndrome |
| Broad casts | Very wide | Late CKD — form in dilated/atrophied tubules |
| Tubular epithelial cell casts | Contain RTECs | ATN, nephrotoxic injury |
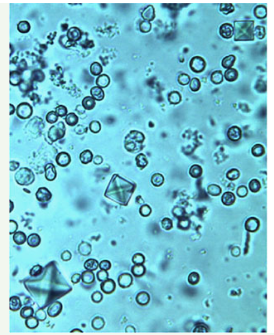
E. Crystals
| Crystal | Appearance | Conditions |
|---|---|---|
| Calcium oxalate | Envelope-shaped (dihydrate) or dumbbell (monohydrate) | Normal; calcium oxalate stones; ethylene glycol poisoning |
| Uric acid | Yellow-brown, rhomboid/rosette | Acidic urine; gout; tumor lysis syndrome |
| Triple phosphate (Struvite) | Coffin-lid shape | Alkaline urine; UTI with urea-splitters (Proteus); struvite stones |
| Calcium phosphate (Apatite) | Amorphous in alkaline urine | Alkaline urine, hyperparathyroidism, RTA |
| Cystine | Hexagonal | Cystinuria (pathological — always significant) |
| Cholesterol | Notched rectangles | Nephrotic syndrome |
| Bilirubin | Yellow-brown needles | Bilirubinuria, liver disease |
F. Bacteria
- Normal: None (in properly collected mid-stream specimen)
- Bacteria + pyuria → infection (UTI)
- Bacteria without pyuria → colonization or contamination
- Gram stain can guide empiric therapy before culture results
G. Other Elements
- Yeast (Candida): Oval budding cells ± pseudohyphae → candiduria (catheterized patients, immunocompromised, diabetics)
- Parasites: Schistosoma haematobium eggs (terminal spine) → urinary schistosomiasis (endemic areas)
- Spermatozoa: Normal finding in males; may appear after ejaculation
- Mucus threads: Usually insignificant
Summary Table: Quick Reference
| Component | Normal | Key Abnormal Findings |
|---|---|---|
| Color | Pale–deep yellow | Red (hematuria), brown (glomerular bleed/liver) |
| Turbidity | Clear | Cloudy = phosphaturia or pyuria |
| SG | 1.003–1.030 | Fixed 1.010 = isosthenuria (CKD, DI) |
| pH | 4.5–8.0 | Alkaline = UTI/RTA/obstruction; Acidic = acidosis/DKA |
| Protein | Negative | Glomerular, tubular, or overflow proteinuria |
| Glucose | Negative | DM (>180 mg/dL), Fanconi (normal BG) |
| Ketones | Negative | DKA, starvation |
| Blood | Negative | Hematuria, hemoglobinuria, myoglobinuria |
| Leukocyte esterase | Negative | UTI, ATIN, TB |
| Nitrite | Negative | Gram-negative bacteriuria |
| Bilirubin | Negative | Obstructive/hepatocellular jaundice |
| Urobilinogen | Trace | ↑ = hemolysis/liver; absent = obstruction |
| RBCs | 0–2/HPF | ≥3 = hematuria; dysmorphic = GN |
| WBCs | 0–5/HPF | >5 = pyuria; WBC casts = pyelonephritis/ATIN |
| Casts | None (± hyaline) | RBC casts = GN; muddy brown = ATN; waxy = CKD |
| Crystals | Occasional | Cystine = always pathological; coffin-lid = struvite |
Clinical Patterns to Know
| Urinalysis Pattern | Diagnosis to Consider |
|---|---|
| RBC casts + proteinuria + hematuria | Nephritic syndrome / GN |
| Heavy proteinuria + fatty casts + lipiduria | Nephrotic syndrome |
| Muddy brown granular casts + RTECs | Acute tubular necrosis (ATN) |
| WBC casts + sterile pyuria | Acute interstitial nephritis (ATIN) |
| Leukocyte esterase + nitrite + bacteriuria | Urinary tract infection |
| Sterile pyuria + alkaline urine | TB, ATIN, partially treated UTI |
| Glycosuria + normal blood glucose | Fanconi syndrome (proximal tubular dysfunction) |
| Bilirubinuria + absent urobilinogen | Obstructive jaundice |
| Hexagonal crystals | Cystinuria |
| Cola urine + dysmorphic RBCs + RBC casts | Glomerulonephritis |
Sources: Campbell Walsh Wein Urology | Brenner and Rector's The Kidney | Harriet Lane Handbook (Johns Hopkins) | Harrison's Principles of Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.