Evaluation of airway in patient with huge thyroid swelling+ striodor
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
thyroid goiter airway management stridor tracheal compression
Reading File
Reading File
Loading Image
I now have comprehensive material to write a detailed, authoritative answer. Let me compile everything.
Airway Evaluation in a Patient with Huge Thyroid Swelling + Stridor
A patient presenting with a large goiter and stridor represents an anticipated difficult airway - one of the most dangerous surgical scenarios. Stridor is a red flag indicating significant tracheal compromise (typically >50% luminal reduction), mandating a structured, methodical evaluation before any anesthetic is administered.
1. Why This Is a High-Risk Situation
Tracheal compression, the presence of dyspnoea, and cancerous pathology in patients with a goiter undergoing thyroid surgery are all independently predictive of difficulty with intubation. Stridor specifically indicates that the cross-sectional area of the tracheal lumen is critically reduced. Up to 20% of patients with large cervical and retrosternal goiters present with acute airway distress, and up to 10% require intubation emergently.
2. Clinical History
Take a focused history to stratify urgency and severity:
| Question | Significance |
|---|---|
| Duration and progression of breathing difficulty | Chronic vs. acute-on-chronic |
| Positional worsening (worse lying down or turning head) | Suggests dynamic/positional compression |
| Stridor character: inspiratory vs. expiratory vs. biphasic | Inspiratory = extrathoracic (above glottis/cervical trachea); Biphasic = severe fixed obstruction |
| Dysphagia | Esophageal compression co-existing |
| Voice change / hoarseness | Recurrent laryngeal nerve (RLN) involvement - danger sign |
| Rate of goiter growth | Rapid growth suggests hemorrhage into nodule, malignancy, or Graves' |
| Previous airway/neck surgery or radiotherapy | Worsens difficulty |
| Nocturnal dyspnea, orthopnea, choking | Intrathoracic component likely |
3. Physical Examination
a. General
- Degree of respiratory distress - use of accessory muscles, paradoxical breathing, tracheal tug
- Oxygen saturation on room air
b. Neck/Goiter Assessment
- Size and consistency of the swelling - hard/fixed raises concern for malignancy
- Tracheal deviation - visible or palpable shift from midline
- Substernal extension - goiter descending below sternal notch on swallowing
- Fixity to underlying structures
- Pemberton's sign: Ask the patient to raise both arms above the head. Development of venous engorgement, facial plethora, or subjective respiratory discomfort suggests obstruction at the thoracic inlet from a large/substernal goiter - a positive Pemberton's sign is a critical finding.
c. Laryngeal/Airway Examination
- Vocal cord mobility - must be assessed in ALL patients (indirect laryngoscopy or flexible nasendoscopy); bilateral RLN palsy post-compression is catastrophic
- Stridor character: inspiratory stridor suggests supraglottic or extrathoracic tracheal obstruction; biphasic stridor indicates a fixed, severe obstruction
- Mallampati classification - though less predictive in this context, still useful
- Thyromental distance (<3 fingerbreadths = likely difficult intubation)
- Mouth opening, neck mobility, jaw prognathism
d. Standard Difficult Airway Predictors (ASA 2022)
Per the ASA airway examination table:
- Long upper incisors, prominent overbite
- Distance between incisors ≤3 cm
- Uvula not visible with tongue protruded (Mallampati III/IV)
- Highly arched/narrow palate
- Noncompliant mandibular space
- Short thick neck, limited head/neck range of motion
4. Investigations
a. Imaging
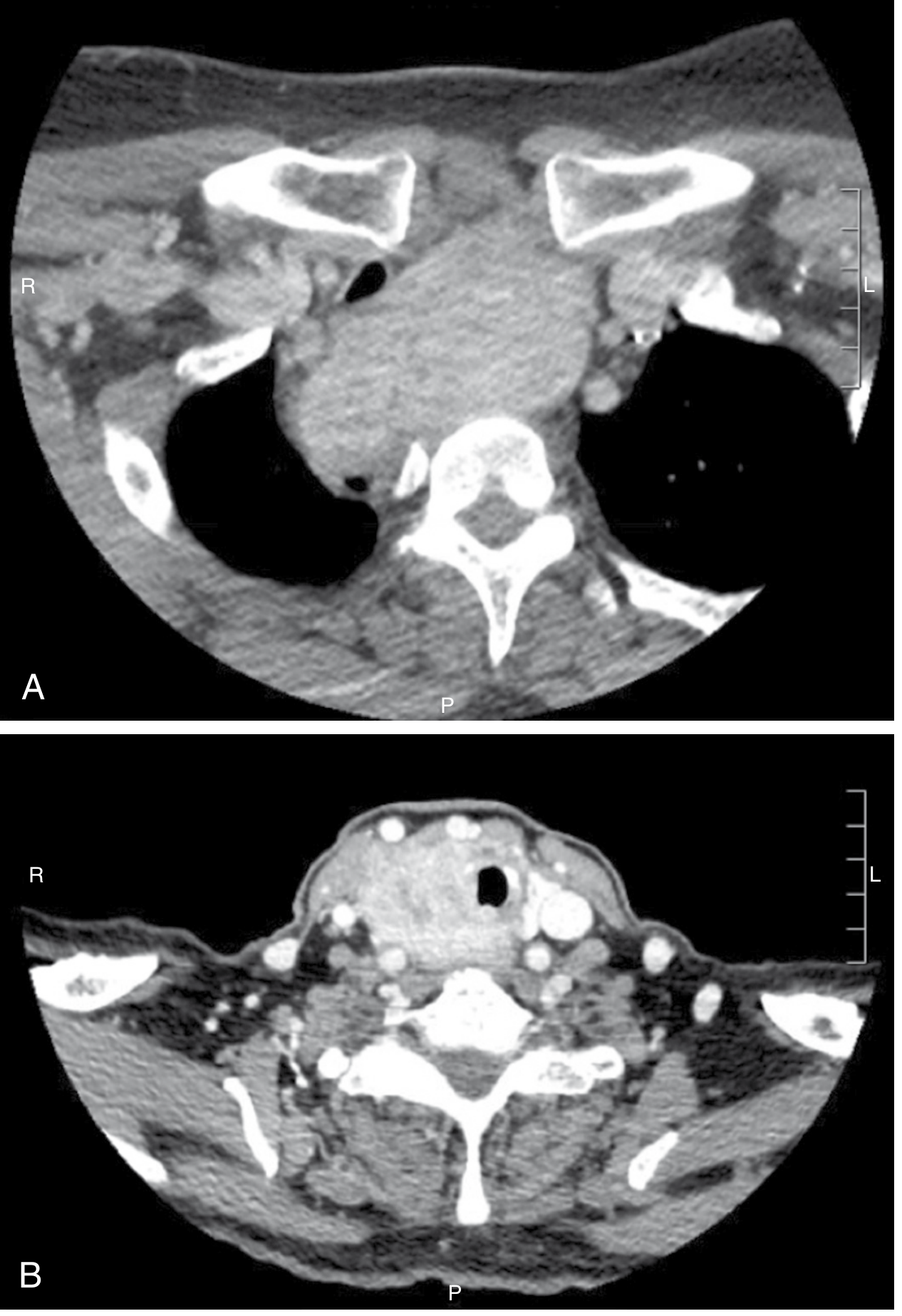
CT scan of neck and chest (without IV contrast for pure compression assessment) is the gold standard:
- Determines degree and level of tracheal compression/deviation
- Assesses substernal/posterior mediastinal extension
- Identifies vascular anomalies (e.g., lusoria artery, rare non-recurrent laryngeal nerve)
- Scan should span skull base to tracheal bifurcation for complete assessment
- Detects lateral or anteroposterior compression that plain films may miss
Plain X-rays (chest + thoracic inlet views) can show:
- Tracheal narrowing or deviation
- Retrosternal extension
- Calcification within the goiter
MRI: Alternative to CT, especially for soft tissue delineation; less useful for lymph node staging and tracheal calcification.
b. Pulmonary Function Tests - Flow-Volume Loop
This is a key non-invasive test for airway physiology:
| Pattern | Interpretation |
|---|---|
| Inspiratory plateau (flattened inspiratory limb) | Variable extrathoracic obstruction - typical for cervical tracheal compression by goiter |
| Expiratory plateau | Variable intrathoracic obstruction |
| Both inspiratory AND expiratory plateau (box-shaped loop) | Fixed obstruction - severe, site-independent tracheal narrowing |
An inspiratory plateau confirms the clinical finding of inspiratory stridor and quantifies the functional severity of obstruction. Note: patients may have radiographic tracheal compression and abnormal flow-volume loops while being asymptomatic - underscoring the value of objective testing.
c. Flexible Nasendoscopy / Laryngoscopy
- Performed under topical anaesthesia as an awake procedure
- Assesses supra- and glottic pathology, vocal cord mobility
- Can inspect subglottis and upper trachea
- Identifies any co-existing laryngeal pathology
- Helps plan tube size and placement
d. Laboratory
- TSH - to exclude subclinical hyperthyroidism/thyrotoxicosis (thyroid storm risk perioperatively)
- Thyroid antibodies - autoimmune aetiology
- Serum calcium - baseline before surgery
- FNA cytology of suspicious nodules under ultrasound guidance
e. Ultrasound
- Assess vascularity, nodule characteristics
- Does NOT reliably assess tracheal compression (CT is superior for this)
5. Anaesthetic/Pre-operative Airway Planning
Once evaluation is complete, the anesthesia/surgical team must formulate a plan:
Key decisions:
- Awake vs. asleep intubation - In patients with significant tracheal compression and stridor, awake fiberoptic bronchoscopic intubation is the technique of choice. Induction of anaesthesia and muscle relaxants can precipitate complete airway collapse in a patient with tracheal softening (tracheomalacia) from chronic compression.
- Tube size - A narrowed trachea may require a smaller ETT; rigid bronchoscopy may be needed if the tube cannot pass
- Tracheostomy readiness - A surgical airway setup must be immediately available
- Tracheomalacia risk - Chronic tracheal compression can cause cartilage softening; post-extubation collapse is a known complication even after goiter removal (see recent meta-analysis on tracheomalacia post-thyroidectomy, PMID 40070511)
Red flags requiring urgent/emergency intervention:
- Rapidly worsening stridor
- Acute respiratory failure (SpO2 falling)
- Recent sudden enlargement (hemorrhage into nodule at thoracic inlet)
- Bilateral vocal cord paralysis
Summary: Evaluation Framework
HISTORY → Severity, progression, positional, voice change, dysphagia
↓
EXAMINATION → Pemberton's sign, tracheal deviation, vocal cord mobility,
difficult airway predictors (Mallampati, TMD, mouth opening)
↓
INVESTIGATIONS
→ CT neck/chest (skull base to carina) — anatomy, compression degree
→ Flow-volume loop — functional severity (inspiratory plateau = extrathoracic)
→ Flexible nasendoscopy — cord mobility, subglottic status
→ TSH, FNA of concerning nodules
↓
AIRWAY PLAN → Awake FOB intubation preferred
→ Surgical airway standby
→ Tracheomalacia precautions post-op
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1 - Prediction of Difficulty, p. 360
- K.J. Lee's Essential Otolaryngology - Euthyroid Goiter, p. 729
- Bailey and Love's Short Practice of Surgery, 28th ed. - Goitre Investigations
- Sabiston Textbook of Surgery, 7e - Cross-Sectional Imaging, p. 1494
- Cummings Otolaryngology Head and Neck Surgery - Difficult Airway, p. 104
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Airway Examination Table 23-7
- Tracheomalacia post-thyroidectomy: PMID 40070511 (2025 systematic review)
This is a shared conversation. Sign in to Orris to start your own chat.