How to find ECG report
Reading File
Searching the Web
how to read and interpret ECG report electrocardiogram
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a comprehensive guide on how to read and interpret an ECG (electrocardiogram) report, based on medical physiology and emergency medicine textbooks.
How to Read an ECG Report
What is an ECG?
An ECG provides a direct measurement of the rate, rhythm, and time-dependent electrical vector of the heart. It gives fundamental information about the origin and conduction of the cardiac action potential. The key waves correspond to:
| Wave | Represents |
|---|---|
| P wave | Atrial depolarization |
| QRS complex | Ventricular depolarization |
| T wave | Ventricular repolarization |
| U wave | Small deflection after T wave (sometimes seen) |
The 12-Lead ECG Layout
A standard 12-lead ECG looks like this (normal example):
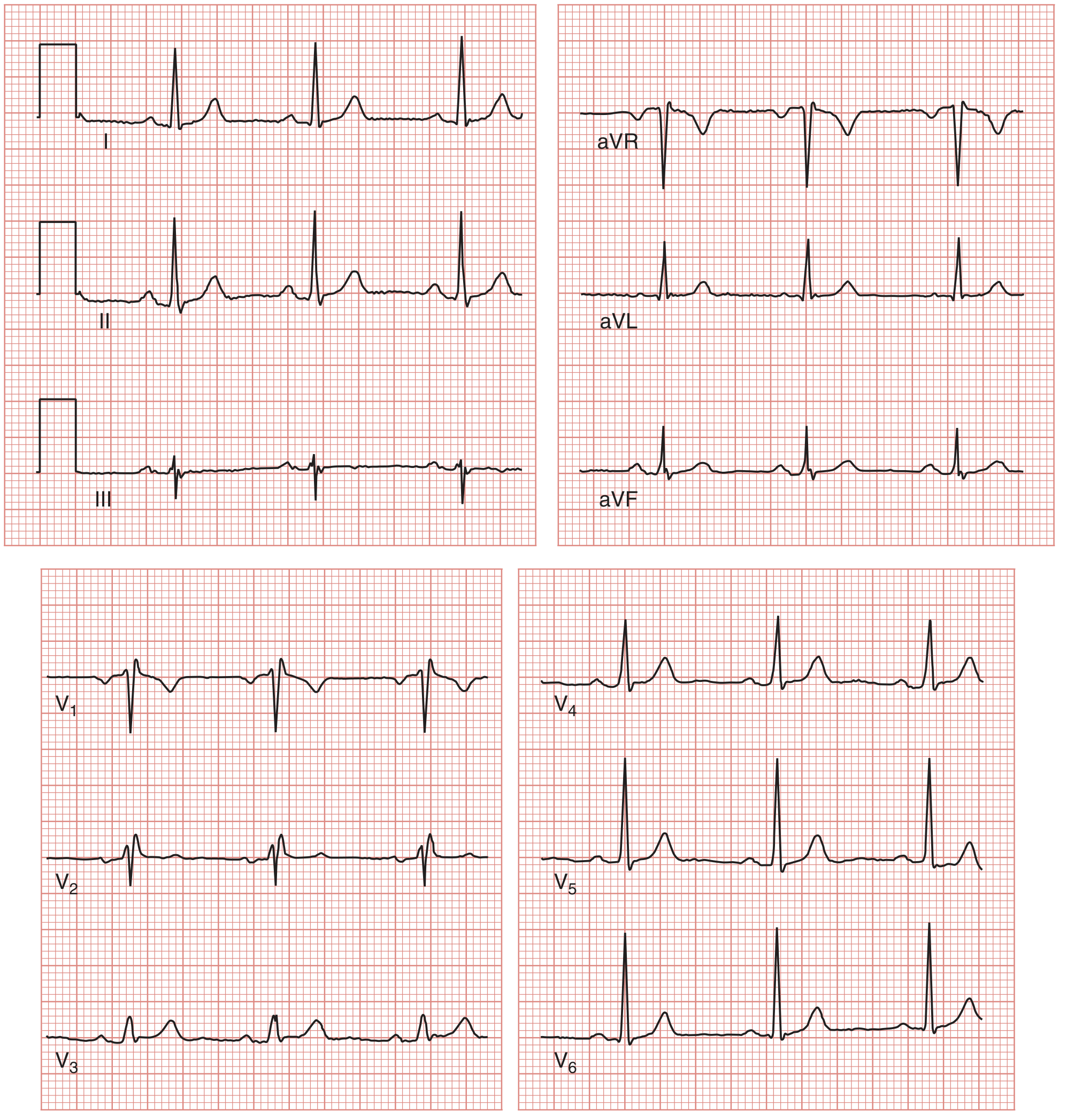
The 12 leads are:
- Limb leads: I, II, III
- Augmented limb leads: aVR, aVL, aVF
- Precordial (chest) leads: V1, V2, V3, V4, V5, V6
ECG Paper Grid
- Small box = 1 mm = 0.04 seconds (horizontal) / 0.1 mV (vertical)
- Large box = 5 mm = 0.2 seconds
- 5 large boxes = 1.0 second
Systematic Steps to Interpret an ECG Report
Step 1 — Rate
Two methods:
- Direct method: Measure the R-R interval in seconds → Rate = 60 ÷ R-R interval
- Quick method: Count large boxes in the R-R interval and use the series: 300 → 150 → 100 → 75 → 60 → 50 (for 1–6 large boxes)
- e.g., 4 large boxes between R waves = 75 bpm
Normal: 60–100 bpm
Step 2 — Rhythm
Answer these questions:
- Is there a P wave before every QRS?
- Are P waves regular and consistent in shape?
- Is the pacemaker coming from the sinus node (normal sinus rhythm) or elsewhere?
Step 3 — Intervals
| Interval | Measurement | Normal Value |
|---|---|---|
| PR interval | Start of P wave → Start of QRS | 0.12–0.20 sec (3–5 small boxes) |
| QRS duration | Start → End of QRS complex | < 0.12 sec (< 3 small boxes) |
| QT interval | Start of QRS → End of T wave | Rate-dependent (corrected QTc ≤ 0.44 sec) |
| R-R interval | Peak-to-peak between QRS complexes | Determines rate |
Step 4 — Axis
- Normal axis: QRS positive in lead I and aVF
- Left axis deviation: Positive I, negative aVF
- Right axis deviation: Negative I, positive aVF
Step 5 — P Wave Morphology
- Should be upright in leads I, II, aVF
- Duration < 0.12 sec; amplitude < 2.5 mm
- Abnormalities suggest atrial enlargement or ectopic rhythm
Step 6 — QRS Morphology
- Q waves: Normal small q waves are okay; pathological Q waves (deep, wide) suggest prior MI
- Bundle branch blocks: Wide QRS (> 0.12 sec) with specific patterns in V1/V6
- Ventricular hypertrophy: Tall R or deep S waves
Step 7 — ST Segment
- Should be isoelectric (flat, at baseline)
- ST elevation: Suggests acute MI (STEMI), pericarditis, or vasospasm
- ST depression: Suggests ischemia, NSTEMI, or digoxin effect
Step 8 — T Wave
- Should be upright in most leads (normally inverted in aVR, V1)
- T wave inversion: Ischemia, LVH, bundle branch block
- Peaked T waves: Hyperkalemia
Step 9 — U Wave
- Small deflection after T wave
- Prominent U waves: Hypokalemia, bradycardia
Key Abnormalities to Recognize
| ECG Finding | Clinical Significance |
|---|---|
| ST elevation in 2+ contiguous leads | STEMI — urgent reperfusion |
| New LBBB | Treat as STEMI equivalent |
| ST depression / T wave inversion | NSTEMI / unstable angina |
| Prolonged PR (> 0.20s) | 1st degree AV block |
| Wide QRS (> 0.12s) | Bundle branch block or ventricular rhythm |
| Prolonged QTc | Risk of torsades de pointes |
| Peaked T waves | Hyperkalemia |
Clinical Tip (Emergency Medicine)
For patients with chest pain, obtain a 12-lead ECG rapidly and compare with any previous tracings. Patients with ST elevation, new LBBB, or ST depression have ACS and require immediate management. Even a normal ECG does not rule out MI (1–6% of patients with a normal ECG still have NSTEMI). — Tintinalli's Emergency Medicine
Sources: Medical Physiology (BOX 21-2), Tintinalli's Emergency Medicine
How to read ECG report explain in telugu
ECG రిపోర్ట్ ఎలా చదవాలి — తెలుగులో వివరణ
ECG అంటే ఏమిటి?
ECG (Electrocardiogram) అంటే హృదయం యొక్క విద్యుత్ చర్యలను కాగితంపై రికార్డ్ చేసే పరీక్ష. ఇది హృదయం ఎంత వేగంగా కొట్టుకుంటుందో, దాని లయ సరిగా ఉందా లేదా అని చెప్తుంది.
ECG లో కనిపించే తరంగాలు (Waves)
| తరంగం | అర్థం |
|---|---|
| P Wave | గుండె యొక్క పై భాగం (Atria) కుంచించుకోవడం |
| QRS Complex | గుండె యొక్క కింది భాగం (Ventricles) కుంచించుకోవడం |
| T Wave | Ventricles విశ్రాంతి తీసుకోవడం |
| U Wave | కొన్నిసార్లు T తరంగం తర్వాత కనిపిస్తుంది |
ECG పేపర్ అర్థం చేసుకోవడం
- చిన్న చతురస్రం = 0.04 సెకన్లు (సమయం) / 0.1 mV (శక్తి)
- పెద్ద చతురస్రం = 0.2 సెకన్లు
- 5 పెద్ద చతురస్రాలు = 1 సెకను
ECG చదవడానికి క్రమపద్ధతి (Systematic Steps)
దశ 1 — హృదయ స్పందన వేగం (Heart Rate)
సులభమైన పద్ధతి:
రెండు R తరంగాల మధ్య ఉన్న పెద్ద చతురస్రాలు లెక్కించి ఈ సూత్రం వాడండి:
Rate = 300 ÷ పెద్ద చతురస్రాల సంఖ్య
| పెద్ద చతురస్రాలు | హృదయ స్పందన |
|---|---|
| 1 | 300/min |
| 2 | 150/min |
| 3 | 100/min |
| 4 | 75/min ✅ సాధారణం |
| 5 | 60/min |
| 6 | 50/min |
సాధారణ రేటు: 60–100 bpm
దశ 2 — లయ (Rhythm)
- ప్రతి QRS కి ముందు P తరంగం ఉందా?
- అన్ని P తరంగాలు ఒకే ఆకారంలో ఉన్నాయా?
- సాధారణ లయ = Normal Sinus Rhythm (NSR)
దశ 3 — Intervals (వ్యవధులు)
| Interval | కొలత | సాధారణ విలువ |
|---|---|---|
| PR Interval | P తొలి→ QRS తొలి | 0.12–0.20 సెకన్లు |
| QRS Duration | QRS మొదలు→ చివర | < 0.12 సెకన్లు |
| QT Interval | QRS మొదలు→ T చివర | రేటుపై ఆధారపడుతుంది |
దశ 4 — ST Segment పరిశీలన
| ST స్థితి | అర్థం |
|---|---|
| ST ఎత్తుగా ఉంటే (ST Elevation) | గుండె పోటు (STEMI) — అత్యవసరం ⚠️ |
| ST తక్కువగా ఉంటే (ST Depression) | గుండె నొప్పి / ischemia |
| సాధారణ స్థాయిలో | సాధారణం |
దశ 5 — T తరంగం
- సాధారణంగా పైకి ఉండాలి
- తిరగబడి ఉంటే (T inversion): గుండె నొప్పి సూచన
- చాలా పొడవుగా ఉంటే: పొటాషియం ఎక్కువగా ఉందని (Hyperkalemia) సూచన
ముఖ్యమైన అసాధారణతలు — గుర్తించడం
| ECG లో కనిపించేది | అర్థం |
|---|---|
| ST ఎత్తు (2+ leads లో) | తీవ్రమైన గుండెపోటు (STEMI) |
| కొత్త LBBB | STEMI తో సమానం |
| PR interval పెరిగితే (> 0.20s) | 1st Degree AV Block |
| QRS వెడల్పు (> 0.12s) | Bundle Branch Block |
| పొడవైన QT | Torsades ప్రమాదం |
| చాలా ఎత్తైన T తరంగాలు | Hyperkalemia |
12-Lead ECG లో Lead అర్థాలు
| Leads | హృదయంలో ఏ భాగాన్ని చూస్తాయి |
|---|---|
| II, III, aVF | కింది భాగం (Inferior wall) |
| I, aVL, V5, V6 | పక్క భాగం (Lateral wall) |
| V1–V4 | ముందు భాగం (Anterior wall) |
| aVR | గుండె లోపలి వైపు |
సాధారణ ECG రిపోర్ట్ చదివేటప్పుడు గుర్తుంచుకోవలసిన విషయాలు
- రేటు సాధారణంగా ఉందా? (60–100 bpm)
- లయ సక్రమంగా ఉందా?
- PR, QRS, QT intervals సరిగా ఉన్నాయా?
- ST segment సాధారణ స్థాయిలో ఉందా?
- T తరంగాలు సరిగా ఉన్నాయా?
- Q తరంగాలు అసాధారణంగా ఉన్నాయా? (పాత గుండెపోటు సూచన)
⚠️ గమనిక: ECG రిపోర్ట్ చదవడం వైద్యులకు సహాయకరంగా అర్థం చేసుకోవడానికి ఈ వివరణ ఇవ్వబడింది. ఏదైనా అసాధారణత కనిపిస్తే వెంటనే డాక్టర్ను సంప్రదించండి.
This is a shared conversation. Sign in to Orris to start your own chat.