Thyroid embryology, surgical anatomy include artery,venous, lymphatic drainage,signs and symptoms, type of conditions investigations,preop prep types of surgeries,post OP complications
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Refer from Bailey and love
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Here is the complete thyroid surgery notes from Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 55, covering every topic you requested:
THYROID - Bailey & Love (28th Ed.) Chapter 55
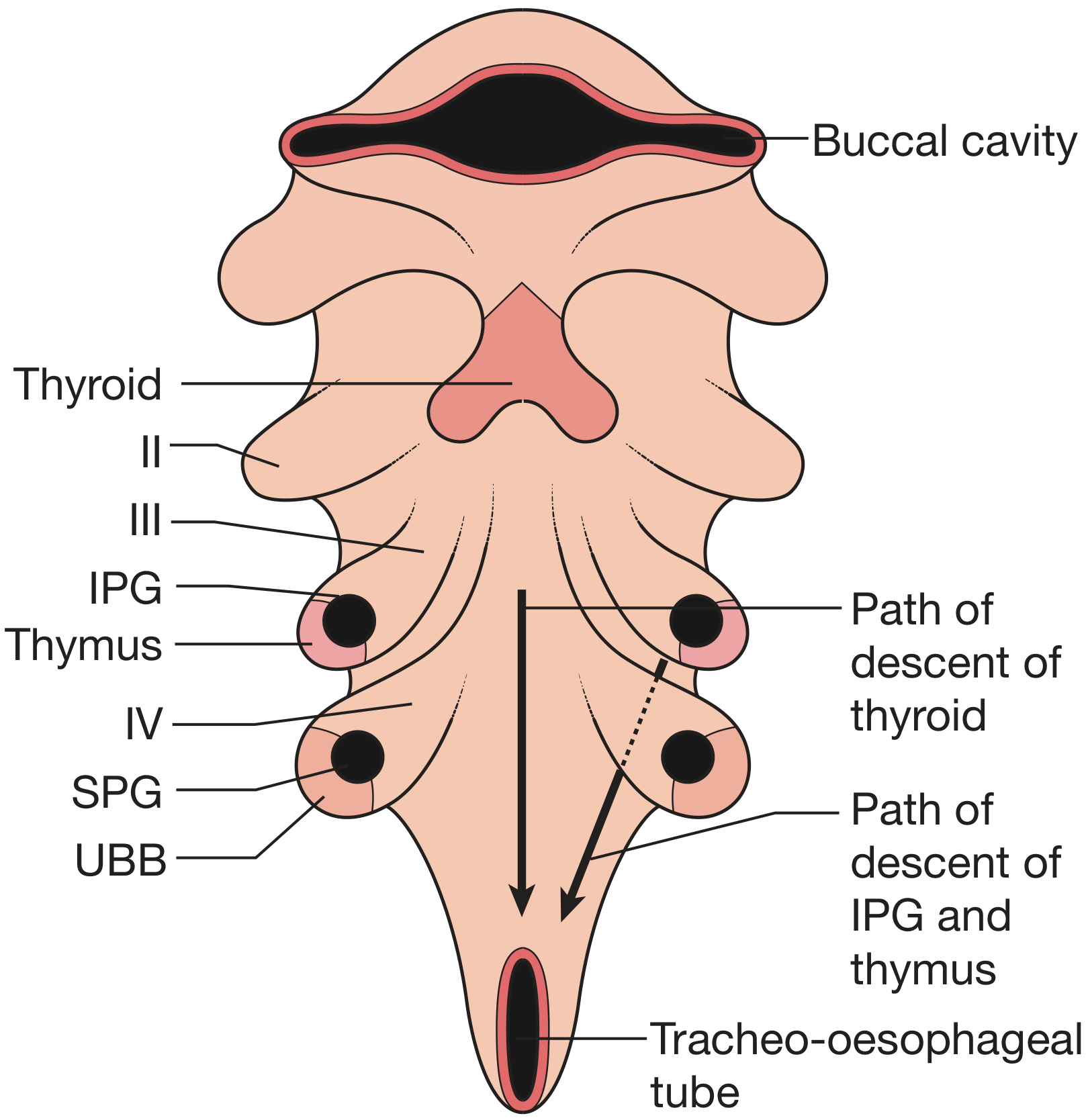
1. EMBRYOLOGY
- The thyroid originates from the median bud of the pharynx (thyroglossal duct)
- The foramen caecum (junction of anterior 2/3 and posterior 1/3 of tongue) is the vestigial remnant
- The duct migrates caudally, passing through or adjacent to the developing hyoid cartilage
- Parathyroids develop from the 3rd and 4th pharyngeal pouches
- The thymus also arises from the 3rd pouch - as it descends it drags the inferior parathyroid with it, which is why the inferior parathyroid lies below the superior (but can be found anywhere along this line of descent)
- Parafollicular C cells (calcitonin-secreting) reach the thyroid from neural crest cells via the ultimobranchial body
2. SURGICAL ANATOMY
Normal gland: 20-25 g. Functioning unit = a lobe supplied by a single arteriole, containing 24-40 follicles lined with cuboidal epithelium; follicles contain colloid (thyroglobulin stored here).
Arterial Supply
| Artery | Origin |
|---|---|
| Superior thyroid artery | First branch of external carotid artery |
| Inferior thyroid artery | Thyrocervical trunk (subclavian artery) |
| Thyroidea ima (~3%, inconstant) | Arch of aorta or brachiocephalic trunk |
Extensive anastomoses occur between main thyroid arteries and branches of tracheal and oesophageal arteries.
Venous Drainage
| Vein | Drains into |
|---|---|
| Superior thyroid vein | Internal jugular vein |
| Middle thyroid vein | Internal jugular vein |
| Inferior thyroid vein | Left brachiocephalic vein |
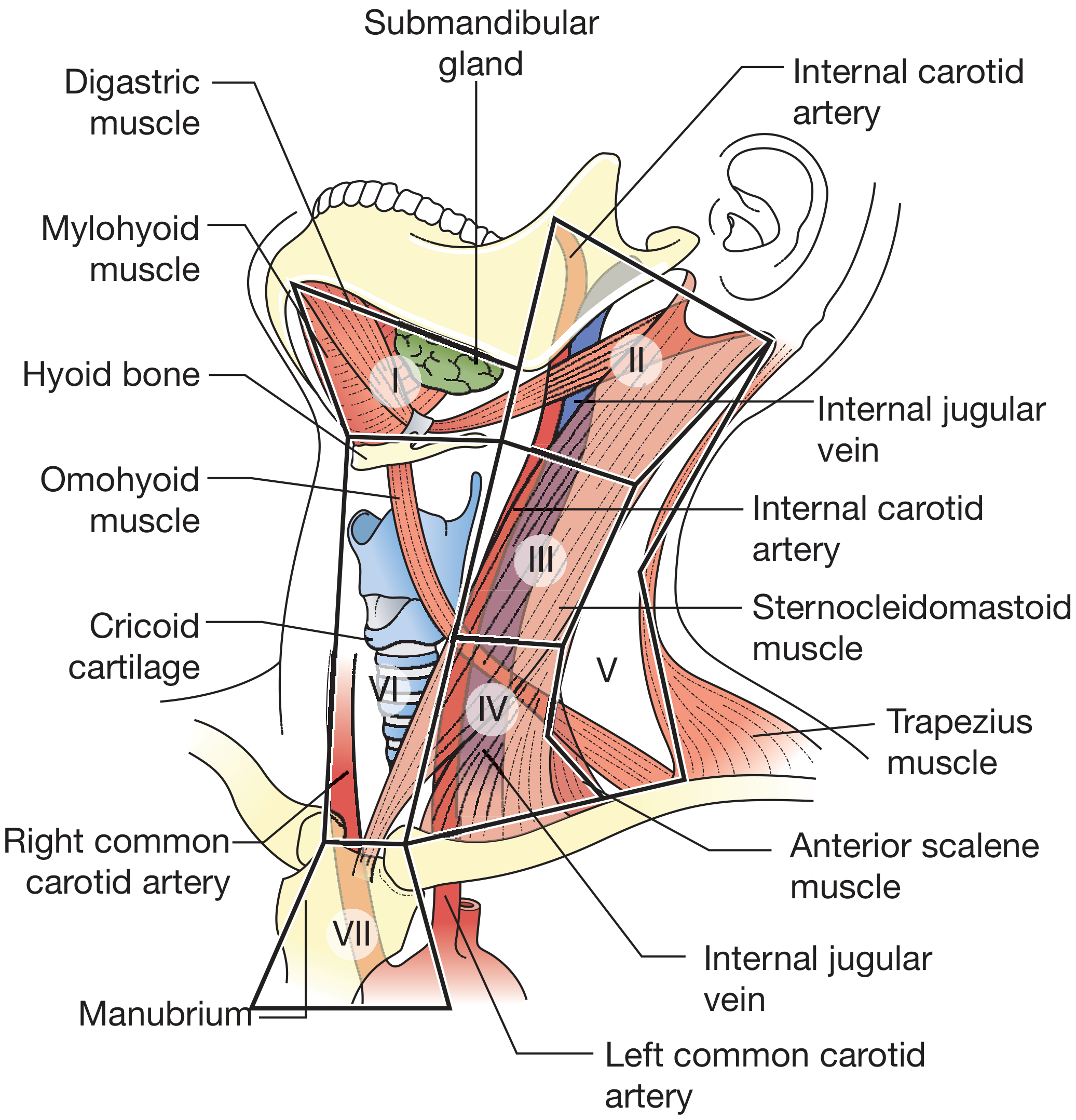
Lymphatic Drainage
The subcapsular plexus drains principally to the central compartment (Level VI):
- Delphian nodes (juxtathyroid/pretracheal)
- Paratracheal nodes
- Nodes on superior and inferior thyroid veins
Then onward to:
- Deep cervical nodes (Levels II, III, IV, V)
- Mediastinal nodes (Level VII)
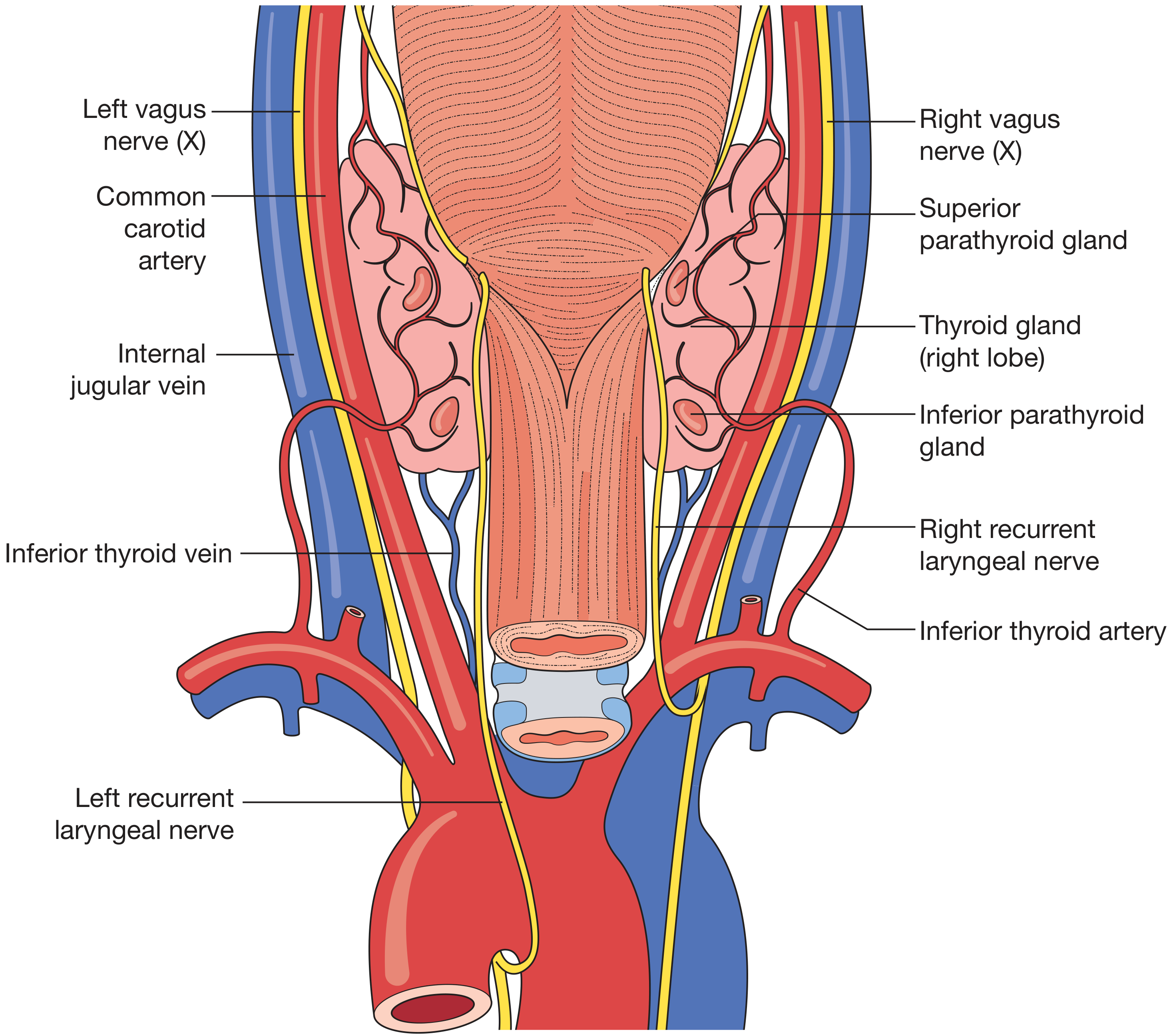
Recurrent Laryngeal Nerve (RLN) - Surgically Critical
- Branch of the vagus nerve
- Left RLN: recurs around the arch of aorta → runs more medially in the tracheo-oesophageal groove
- Right RLN: recurs around the subclavian artery → runs more obliquely
- ~2% on the right are non-recurrent (enter larynx from above - associated with aberrant right subclavian artery)
- Located in the tracheo-oesophageal groove, forms one side of Behr's triangle (carotid artery + inferior thyroid artery + RLN)
- Found under the Tubercle of Zuckerkandl during lateral lobe mobilisation
- Greatest risk at Berry's ligament (pretracheal fascia binding thyroid to trachea at cricothyroid joint)
External Branch of Superior Laryngeal Nerve (EBSLN)
Runs with the superior thyroid artery near the upper pole. Injury → loss of vocal cord tension → diminished power and pitch range.
3. CONDITIONS / CLASSIFICATION
Table 55.3 - Classification of Thyroid Swellings:
| Category | Sub-type |
|---|---|
| Simple goitre (euthyroid) | Diffuse hyperplastic (physiological, pubertal, pregnancy); Multinodular |
| Toxic | Graves' disease (diffuse); Toxic MNG; Toxic adenoma (Plummer's) |
| Inflammatory | Autoimmune (Hashimoto's); Subacute (de Quervain's); Riedel's; Suppurative |
| Neoplastic - Benign | Follicular adenoma |
| Neoplastic - Malignant | Papillary 80%, Follicular 10%, Anaplastic 5%, Medullary 2.5%, Lymphoma 2.5% |
4. SIGNS AND SYMPTOMS
All Thyroid Swellings
- Anterior neck swelling moving on swallowing (hallmark)
- Pressure symptoms: dysphagia, dyspnoea, stridor (retrosternal extension)
- Superior vena cava obstruction (large retrosternal goitre)
Hypothyroidism
- Weight gain, cold intolerance, constipation, fatigue, bradycardia
- Dry skin, hair loss, periorbital oedema, hoarse voice
- Menorrhagia, hyporeflexia
Hyperthyroidism (Thyrotoxicosis)
- Weight loss with good appetite, heat intolerance, sweating
- Palpitations, tachycardia, atrial fibrillation
- Tremor, anxiety, diarrhoea, oligomenorrhoea
- Proximal myopathy
Graves' Disease (additional)
- Exophthalmos, lid lag, lid retraction, chemosis
- Pretibial myxoedema
- Thyroid acropachy (clubbing)
- Thyroid bruit (very vascular gland)
Features Suggesting Malignancy
- Extremes of age, male sex
- Hard, irregular, fixed swelling
- Hoarseness + non-occlusive cough = RLN palsy (almost pathognomonic)
- Cervical lymphadenopathy along internal jugular vein (almost diagnostic of PTC)
- Rapid growth or sudden pain (usually haemorrhage, but exclude malignancy)
5. INVESTIGATIONS
Biochemical
- Serum TSH - most sensitive test (immunochemiluminometric assay; can detect very low values)
- Free T3 and Free T4 - interpreted with TSH
- Thyroid autoantibodies: Anti-TPO (>25 U/mL significant), antithyroglobulin (>1:100 significant)
- TRAb (TSH receptor antibodies) - for Graves' disease
- Calcitonin - for suspected medullary carcinoma
| State | TSH | FT4 | FT3 |
|---|---|---|---|
| Euthyroid | Normal | Normal | Normal |
| Florid failure | Very raised | Low | Low |
| Incipient failure | Raised | Low-normal | Low-normal |
| Thyrotoxicosis | Suppressed | Raised | Raised |
Imaging
- Ultrasound - gold standard for nodule evaluation; guides FNAC
- Scintigraphy (Tc99m or I123) - hot vs cold nodules; toxic adenoma
- CT/MRI - retrosternal extension, tracheal compression (arms-down position preferred)
- PET - selected oncology cases
Cytology - FNAC (Thy Classification)
| Grade | Meaning |
|---|---|
| Thy1 | Non-diagnostic |
| Thy1c | Non-diagnostic, cystic |
| Thy2 | Non-neoplastic (benign) |
| Thy3 | Follicular lesion (adenoma vs carcinoma cannot be distinguished cytologically) |
| Thy4 | Suspicious of malignancy |
| Thy5 | Malignant |
Thy3-5 → Surgery indicated. Follicular adenoma vs carcinoma requires histological assessment of capsular/vascular invasion.
Other
- Laryngoscopy - preop vocal cord assessment (especially if hoarse or previous neck surgery)
6. PREOPERATIVE PREPARATION
For All Thyroid Patients
- Vocal cord assessment (laryngoscopy)
- Baseline TFTs and calcium/PTH
- Cross-sectional imaging if retrosternal/large goitre
- Intraoperative nerve monitoring (IONM) setup if planned
Mandatory for Thyrotoxic Patients (to prevent thyroid storm)
Option 1 - Antithyroid Drugs
- Carbimazole or propylthiouracil
- Restore to euthyroid state; takes weeks
Option 2 - Beta-Adrenergic Blockade (faster)
- Propranolol 40 mg TDS (up to 80 mg TDS; or Nadolol 320 mg OD)
- Also blocks peripheral T4 → T3 conversion
- Patient euthyroid in days
- Must continue for 7 days postoperatively (thyroid hormone levels remain elevated for days after surgery)
Lugol's Iodine (10 days preop)
- Given with carbimazole or beta-blocker
- Reduces gland vascularity
- Adds safety if beta-blocker dose is missed on the day of operation
- Not universally used
7. TYPES OF THYROID OPERATIONS
All operations are built from three basic elements:
- Total lobectomy
- Isthmusectomy
- Subtotal lobectomy
| Operation | Components |
|---|---|
| Total thyroidectomy | Total lobectomy (×2) + isthmusectomy |
| Subtotal thyroidectomy | Subtotal lobectomy (×2) + isthmusectomy |
| Near-total (Dunhill) | Total lobectomy + isthmusectomy + subtotal lobectomy |
| Hemithyroidectomy | Total lobectomy + isthmusectomy |
Procedure Selection by Indication
| Condition | Choice |
|---|---|
| Graves' disease | Total/near-total thyroidectomy (residual tissue = risk of recurrence) |
| Bilateral toxic MNG | Total thyroidectomy |
| Asymmetric MNG | Total lobectomy on affected side ± Dunhill |
| Toxic adenoma | Lobectomy or hemithyroidectomy |
| Follicular lesion | Lobectomy (histology required) |
| Differentiated thyroid cancer | Total thyroidectomy ± central neck dissection |
| Retrosternal goitre | Transcervical approach (>95%); sternotomy if posterior mediastinum, malignant, or diameter exceeds thoracic inlet |
Bailey's dictum on Graves': "Thyroid failure should not be regarded as a failure of treatment, but recurrent toxicity is."
Surgical Technique (Key Steps)
- Patient position: Supine, neck extended, shoulder roll, reverse Trendelenburg
- Incision: Kocher's collar incision 2 finger-breadths above clavicle in skin crease
- Subplatysmal flaps, strap muscles divided in midline
- Superior pole: vessels ligated close to thyroid (protect EBSLN)
- RLN identified and traced throughout its course throughout the case
- Parathyroids identified and preserved with vascular pedicles
- Berry's ligament divided carefully
- Haemostasis; strap muscles not closed watertight (allows haematoma to escape subcutaneously)
- Drain: not proven to prevent haematoma
8. POSTOPERATIVE COMPLICATIONS
A. Early, Life-Threatening
1. Haematoma / Haemorrhage
- Most frequent life-threatening complication (~1 in 50 patients)
- Almost all develop within first 24 hours
- Mechanism: arterial bleed → rising central compartment pressure → exceeds venous pressure → laryngeal venous oedema → airway obstruction → death
- Management: Immediately remove skin sutures (releases pressure), call senior, secure airway with ETT, evacuate haematoma, control bleeding point
- Wound drains do NOT have a protective effect
2. Bilateral RLN Injury
- Immediate respiratory obstruction
- Requires emergency tracheostomy
B. Early, Non-Life-Threatening
3. Unilateral RLN Palsy
- BAETS audit: 1.8% at 1 month, declining to 0.5% at 3 months for first operations
- Transient more common than permanent
- Permanent paralysis rare if nerve identified intraoperatively
- If transected → reanastomose immediately; if segment excised → ansa cervicalis anastomosis
- Long-term: speech therapy, medialization procedures
4. EBSLN Injury
- Loss of vocal tension → diminished power and pitch range
- Often subtle; critical for professional voice users
5. Hypocalcaemia / Parathyroid Insufficiency
- Ischaemia of parathyroids (vascular injury) more important than inadvertent removal
- Permanent hypoparathyroidism < 1%
- Onset: typically 2-5 days postop (rarely 2-3 weeks)
- Symptoms: paraesthesia of fingers, toes, perioral; tetany; Chvostek's sign; Trousseau's sign
- Highest risk: total thyroidectomy + central neck dissection
- Management: serial calcium monitoring, oral/IV calcium, calcitriol
6. Thyroid Storm (Thyrotoxic Crisis)
- Occurs in inadequately prepared thyrotoxic patient - now very rare with proper preop
- Supportive: IV fluids, ice packs, O2, diuretics, digoxin (for AF), sedation, IV hydrocortisone
- Specific: Carbimazole 10-20 mg 6-hourly, Lugol's iodine 10 drops 8-hourly (or sodium iodide 1 g IV), Propranolol IV 1-2 mg or oral 40 mg 6-hourly
7. Thyroid Insufficiency
- 100% after total thyroidectomy
- ~1 in 3 patients after lobectomy
- Higher with positive thyroid autoantibodies
- Thyroxine started day 1 postoperatively after total thyroidectomy
C. Late
8. Wound Infection - cellulitis, occasionally deep infection
9. Stitch Granuloma - from non-absorbable (especially silk) sutures; use absorbable sutures throughout
10. Recurrent Goitre - after subtotal resection; reoperation is more difficult and hazardous
11. Keloid Scar - young women particularly affected
9. POSTOPERATIVE CARE (Summary)
- Overnight inpatient observation (UK standard - haematoma risk)
- Hourly wound observations for haematoma in first 24 hours; staff must know to remove sutures if swelling develops
- Serial calcium levels after total thyroidectomy; educate patient on symptoms of hypocalcaemia
- Start thyroxine day 1 (total thyroidectomy)
- 4-week follow-up: histology review, wound check, laryngoscopy, TFTs, calcium
Source: Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 55 - Thyroid Gland
This is a shared conversation. Sign in to Orris to start your own chat.