

IMG_20260713_162013.jpg
IMG_20260713_161906.jpg
Y penis aur scortam ki image mein ismein chote daane ya patch se hai ismein se nami nikal rahi halki halki, itching hai chune par jalan hai
Reading File
analyse_media
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
⚠️ Yah ek medical assessment hai, doctor ka substitute nahin
Images aur aapke symptoms (chote daane/patches, nami, itching, jalana) dekhne ke baad main yeh clinical information de raha hoon - lekin in leisions ke liye turant kisi dermatologist ya skin specialist se milna zaroori hai.
Image Analysis - Kya Dikh Raha Hai
Image 1 (Penis/Scrotal area - darker skin):
- Multiple raised nodules aur thickened plaques
- Kuch areas lichenifield (mota, leathery skin)
- Ek linear raised lesion visible - sinus tract ya chronic inflammatory tract jaisa
- Chronic, repeated infection ya inflammation ke signs
Image 2 (Scrotum - glans area):
- Diffuse laalipan (erythema) - active inflammation
- Elongated linear raw area (erosion/fissure) - moist aur glistening
- Skin thickened aur swollen
- Active moisture/discharge ka indication
Possible Conditions (Differential Diagnosis)
1. Tinea Cruris + Candidiasis (Fungal Infection) - Sabse Zyada Likely
Fungal infection groin area mein bahut common hai. Symptoms bilkul match karte hain:
- Itching (khujli)
- Burning sensation (jalana)
- Nami (moisture)
- Red patches
Textbook of Family Medicine ke anusaar: "Tinea cruris involves the proximal medial thighs... Patients frequently complain of burning and pruritus." Scrotum par jo moist, red erosion hai woh Candidal intertrigo ki taraf point karta hai.
2. Intertrigo / Moisture Dermatitis
Garam, namak environment mein skin rubs hoti hai - scrotal skin especially vulnerable hai.
3. Hidradenitis Suppurativa (HS)
Pehli image mein jo nodules aur scarring hai woh chronic HS ke signs ho sakte hain - ek inflammatory condition jo groin/genital area ke sweat glands ko affect karta hai, painful lumps, discharge, aur scars banata hai.
4. Sexually Transmitted Infection (STI)
- Genital area mein erosion, discharge, burning - STI (jaise herpes, syphilis) ko rule out karna zaroori hai
- Doctor se milne par swab test karaya jana chahiye
Abhi Kya Karein (Self-Care - Doctor ke Jaane Tak)
| Step | Kya Karein |
|---|---|
| Safai | Halke garam paani se dhoyein, scented soap avoid karein |
| Dry Rakhein | Nahanay ke baad achhe se pat dry karein, rub nahin |
| Loose Kapde | Dhili cotton underwear pahnen, tight kapde band karein |
| Kharochna Band | Scratching se infection aur failta hai |
| OTC Cream | Clotrimazole 1% cream (antifungal) din mein 2 baar laga sakte hain - agar fungal infection lag raha hai |
| Avoid | Steroid cream akele mat lagayein - doctor se pehle poochein |
Doctor Se Milna Kab Zaroori Hai
Turant doctor ke paas jayein agar:
- Discharge zyada ho ya pus aaye
- Dard bahut badh jaye
- Bukhar aaye
- Daane fail rahe hon
Aapko chahiye:
- Ek Dermatologist (skin doctor) ya Urologist se milein
- Doctor shayad KOH scraping (fungal test), swab culture, ya biopsy karein
- STI panel bhi test karaya ja sakta hai
Yaad Rakhein: Images se poora diagnosis nahin hota. Jo moist erosion aur nodular lesions hain, woh sirf physical examination aur lab tests se confirm ho sakte hain. Kisi bhi cream ya dawai shuru karne se pehle doctor se confirm karein.
Search for clinical images comparing different types of genital rashes to help with diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Yahan Fitzpatrick's Dermatology textbook se clinical comparison images hain jo aapke case ke liye relevant hain:
Genital Rashes - Clinical Image Comparison (Fitzpatrick's Dermatology)
1. Tinea Cruris (Fungal - Dermatophyte)

Pehchaan: Inner thighs aur groin mein annular (ring-shaped) laal patches, raised scaly border, scrotum generally spare rehta hai. Itching aur burning common. Aapke case se comparison: Agar scrotum involved hai toh pure tinea cruris less likely.
2. Candida Intertrigo (Fungal - Yeast) - Aapke case se sabse zyada milta-julta

Pehchaan: Laal papules jo merge ho jaate hain, scrotum involved hota hai (tinea cruris ke upar se key difference), satellite papules, erosion, moisture/discharge. Itching + burning. Yeh aapke symptoms se bahut match karta hai.
3. Candida Intertrigo B - Plaques with Erosion

Pehchaan: Erythematous plaques ke saath erosion (skin peeling/rawness) aur satellite papules. Aapki dusri image (scrotum) mein jo moist erosion dikh rahi thi woh bilkul aise hi dikhti hai.
4. Hidradenitis Suppurativa (HS) - Sinus Tracts

Pehchaan: Chronic nodules jo drain karte hain, sinus tracts (tunnel-like tracks), scarring, darker skin mein visible. Aapki pehli image (penis area) ke nodules aur linear tract HS se milte-julte hain.
Aapke Case mein Image Comparison Summary
| Feature | Tinea Cruris | Candida Intertrigo | Hidradenitis Suppurativa |
|---|---|---|---|
| Scrotum involved | ❌ Nahin | ✅ Haan | ✅ Haan |
| Moist erosion | Rare | ✅ Common | Possible |
| Nami/discharge | Rare | ✅ Haan | ✅ Purulent |
| Nodules/scarring | ❌ | Rare | ✅ Chronic |
| Itching + burning | ✅ | ✅ | Painful mainly |
Aapke symptoms (scrotum mein nami, erosion, itching + burning) aur pehli image mein nodules dekhkar - yeh combination Candida Intertrigo aur/ya Hidradenitis Suppurativa dono ka combination ho sakta hai.
⚠️ In images ko dekhkar apna diagnosis mat karein. Yeh sirf educational comparison hai. Ek dermatologist physical examination aur agar zaroorat ho toh KOH test ya culture se confirm karega. Jaldi doctor se milein.
Candida Intertrigo image aur treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Yahan sab kuch Fitzpatrick's Dermatology aur Harrison's Internal Medicine se liya gaya hai:
Candida Intertrigo - Clinical Images
Image 1: Candida Intertrigo - Genital Area (Inguinal)
Pichli conversation mein yeh image di gayi thi:
Kya dikh raha hai: Laal papules jo milkr ek badi jagah ban rahe hain, scrotum involved hai, satellite papules (alag alag chote daane bahar ki taraf) - yeh aapke case se bahut milta-julta hai.
Image 2: Candida Balanoposthitis (Glans Penis par Candida)

Kya dikh raha hai: Glans penis (sir) aur foreskin par chote chote pustules (pus-filled daane), skin shiny aur moist. Candida ka classic genital presentation. Fitzpatrick's ke anusar: "Pustules are seen more frequently in balanitis and balanoposthitis than in vulvitis."
Candida Intertrigo ke Lakshan (Recognition Guide)
| Feature | Candida Intertrigo |
|---|---|
| Color | Beefy-red (gahra laal) |
| Texture | Moist, macerated |
| Daane | Satellite papules/pustules periphery par |
| Location | Scrotum, groin, skin folds - scrotum involved |
| Discharge | Halki nami ya white discharge |
| Symptoms | Itching + Burning dono |
Key diagnostic point (Fitzpatrick's): Tinea cruris mein scrotum spare rehta hai, lekin Candida intertrigo mein scrotum involved hota hai - yeh dono ko alag karne ka sabse bada sign hai.
Treatment - Dawa Kya Lagaein
(Source: Harrison's Principles of Internal Medicine 22E, Fitzpatrick's Dermatology)
Topical (Cream lagana) - Pehli Line of Treatment
| Dawa | Kaise Lagaein |
|---|---|
| Clotrimazole 1% cream (Candid, Canesten) | Din mein 2 baar, 2-4 hafte |
| Miconazole 2% cream (Daktarin) | Din mein 2 baar, 2-4 hafte |
| Nystatin cream | Din mein 2-3 baar, 2 hafte |
| Ketoconazole 2% cream | Din mein 1-2 baar, 2-4 hafte |
Fitzpatrick's: "Treatment includes topical imidazoles and nystatin... effective topicals include nystatin or azoles (miconazole, clotrimazole, econazole, or ketoconazole)."
Agar Inflammation zyada ho (Laalipan + Jalan)
Halka steroid + antifungal combination:
- Hydrocortisone 1% + Clotrimazole (Candid B / Canesten HC) - thodi der ke liye, doctor ke batane par
- Harrison's: "The associated inflammatory response... can be treated with a mild glucocorticoid lotion or cream (2.5% hydrocortisone)."
Oral (Khane ki) Dawa - Zyada Severe Cases mein
(Sirf doctor ke prescription ke baad)
| Dawa | Dose |
|---|---|
| Fluconazole | 150 mg ek baar; ya severe mein 50-100 mg daily |
| Oral dawa tab di jaati hai jab topical cream se fayda na ho ya infection zyada failah ho |
Ghar par Dekhbhal (Self-Care)
- Dry rakhein - naha ke baad cotton cloth se thapthapa kar sukhaein, rub nahin
- Loose cotton underwear pahnen
- Cream lagane se pehle area bilkul saaf aur sukha hona chahiye
- Cream lagaate waqt daane ke upar aur 1-2 cm bahar tak bhi lagaein
- Agar diabetes hai toh sugar control karna zaroori hai - Candida sugar mein zyada barhta hai
- Antibiotic chal rahi hai toh doctor ko bataein - antibiotics Candida ko badhate hain
⚠️ Yaad rakhein: Yeh educational information hai. Cream shuru karne se pehle ya agar 1-2 hafte mein sudhar na aaye, doctor se zaroor milein. Diagnosis confirm karna zaroori hai.
Candid cream ya powder better hai
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Goldman-Cecil Medicine se yeh textbook answer mil gaya. Ab complete jawab:
Candid Cream vs Candid Powder - Kaun Behtar?
Aapke case ke liye: Pehle Cream, baad mein Powder
Textbook Kya Kehta Hai
Goldman-Cecil Medicine ke anusar topical formulations ke baare mein:
"A powder promotes dryness and is used to reduce maceration in intertriginous areas... Creams are less greasy than ointments and are useful for the face, groin, and intertriginous areas. Ointments should be avoided in infected or intertriginous areas."
Matlab:
- Cream - active infection treat karne ke liye groin/scrotal area mein sabse suitable formulation hai
- Powder - nami kam karne ke liye, maceration (skin ka geela ho ke galna) rokne ke liye
Dono ka Alag Role
| Candid Cream | Candid Powder | |
|---|---|---|
| Active ingredient | Clotrimazole 1% | Clotrimazole 1% |
| Kaam | Fungus ko directly maarta hai, skin mein achhe se penetrate karta hai | Nami sookh ke fungi ko failne se rokta hai |
| Best for | Active infection - laalipan, daane, erosion (jab symptoms hain) | Prevention ya halki infection mein, dry rakhne ke liye |
| Aapke case mein | ✅ Pehle yahi lagaein - erosion aur active daane hain | ✅ Cream ke baad, ya nahaney ke baad dry karne ke liye |
| Kab avoid karein | Agar skin bahut zyada moist/soaked ho toh pehle dry karo | Raw/open erosion par seedha mat lagao |
Aapke Case ke Liye Ideal Routine
Nahanay ke baad:
1. Area ko cotton kapde se thapthap kar dry karein
2. Candid Cream lagaein - thin layer, 2x din
(sone se pehle aur subah)
3. Din mein jab zyada paseena ho:
Candid Powder halka dust karein - nami absorb karega
Summary
- Cream = Ilaj (treatment) - active infection ke liye zaroori
- Powder = Raksha (prevention/support) - nami control ke liye
- Dono saath use kar sakte hain - cream subah/raat, powder din mein
⚠️ Agar 2 hafte mein sudhar na ho, ya daane barhein, toh doctor se milein. Oral fluconazole tablet (150mg) bhi ho sakti hai doctor ke advice se.
Candida se bachne ke liye lifestyle changes aur prevention tips
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Fitzpatrick's Dermatology se poori risk factor list aur Harrison's se treatment guidance mil gayi. Ab comprehensive answer:
Candida se Bachne ke Liye - Evidence-Based Prevention Guide
(Source: Fitzpatrick's Dermatology, Harrison's Principles of Internal Medicine)
🔴 Samjhein Pehle - Candida Kyon Hota Hai?
Fitzpatrick's Dermatology ke anusaar confirmed risk factors:
"Risk factors for localized/superficial Candida infections include extremes of age; diabetes; obesity; pregnancy; HIV/AIDS; and use of broad-spectrum antibiotics, corticosteroids, or immunosuppressive medications."
Candida normally humare skin par rehta hai - tab hi infection deta hai jab:
- Nami - warm + moist environment bane
- Immunity - kamzor ho
- Normal bacteria - antibiotics se khatam ho jaayein
1. Skin Hygiene aur Moisture Control
| Kya Karein | Kyun Zaroori |
|---|---|
| Rozana nahaein, skin folds (groin, scrotum) achhe se dhoyein | Candida nami mein pahta hai |
| Nahanay ke baad pat dry karein, rub nahin - especially folds mein | Nami = Candida ka ghar |
| Garm mausam mein ya paseena aane ke baad ek baar extra dhoyein | Paseena nami badhata hai |
| Candid Powder ya plain talcum powder use karein skin folds mein | Moisture absorb karta hai |
| Underwear ko din mein zyada gila hone par badlein | Geela kapda = infection risk |
2. Kapde ka Chunaav
| Sahi Kapda | Galat Kapda |
|---|---|
| ✅ Loose cotton underwear (dhila, breathable) | ❌ Tight synthetic underwear (nylon, polyester) |
| ✅ Dhili salwar/pajama | ❌ Tight jeans, tight pants |
| ✅ Cotton fabric jo paseena sookhe | ❌ Occlusive/plastic-y fabric |
| ✅ Roz kapde badle, saaf rakhein | ❌ Ek hi underwear kaafi din pahenna |
3. Diet aur Blood Sugar
Yeh sabse important point hai:
Candida sugar khaata hai - diabetes ya high sugar wale logo mein Candida bahut fast barhta hai.
- Agar diabetes hai: Sugar control karna treatment se bhi zyada zaroori hai - doctor se HbA1c check karaiye
- Meetha kam karein: Refined sugar, maida, cold drinks Candida ko badhate hain
- Fasting sugar check karwaein: Agar baar baar Candida ho raha hai toh diabetes screen zaroori hai
- Weight control: Obesity ek confirmed risk factor hai - Fitzpatrick's ke anusaar
4. Antibiotic aur Dawa Sambhalkaar Lein
- Antibiotic khane ke baad Candida bahut common hota hai - normal bacteria khatam hone se yeast barhta hai
- Agar antibiotic chal rahi hai toh doctor se poochein: "Kya saath mein antifungal bhi lena chahiye?"
- Steroid cream (betamethasone, clobetasol etc.) long term groin par mat lagaein - Candida barhata hai
- Steroid tablets bhi risk factor hain
5. Immunity Majboot Rakhein
| Kya Karein | Fayda |
|---|---|
| Poori neend lein (7-8 ghante) | Immune system strong rehta hai |
| Alcohol kam karein | Immunity par asar paRta hai |
| Smoking band karein | Mucosal immunity kamzor karta hai |
| Balanced diet - sabziyan, protein | Zinc aur Vitamin deficiency Candida badhata hai |
| Stress kam karein | Cortisol se immunity kamzor hoti hai |
6. Baar Baar Hone par (Recurrence Prevention)
Agar Candida baar baar aata hai toh:
- Blood sugar test karwaein (fasting glucose + HbA1c)
- HIV test karwaein agar risk factors hain
- Partner ko bhi check karwaein - partner se reinfection ho sakti hai
- Infection theek hone ke baad 1-2 hafte aur cream lagaein (relapse rokne ke liye)
- Weekly ek baar Candid Powder use karte rahein prevention ke liye
- Doctor se prophylactic fluconazole ke baare mein poochein agar bahut baar aata hai
Quick Summary Card
DAILY ROUTINE:
✅ Roz nahaein + pat dry karein
✅ Loose cotton underwear
✅ Roz kapde badle
✅ Sugar/meetha kam karein
✅ Skin folds mein powder use karein
AVOID:
❌ Tight synthetic kapde
❌ Geeli/nami skin pe kapda pahenna
❌ Self-se steroid cream lagana
❌ Antibiotic ke baad antifungal ignore karna
❌ Diabetes uncontrolled rehne dena
⚠️ Agar yeh sab karne ke baad bhi baar baar Candida ho raha hai toh yeh underlying diabetes, immune problem, ya STI ka sign ho sakta hai - doctor se proper workup zaroor karaiye.
Oral complete treatment batao
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
⚠️ Zaroori Disclaimer Pehle
Yeh medical education ke liye hai. Koi bhi oral antifungal tablet doctor ke prescription ke BINA mat lein. Fluconazole aur itraconazole ke side effects aur drug interactions serious ho sakte hain. Doctor se milne ke baad hi lein.
Oral Antifungal - Complete Treatment Guide
(Source: Dermatology 5e - Fluconazole Dosing Table; Harrison's Principles 22E; Goodman & Gilman's Pharmacology)
Kab Oral Dawa Zaroor Lagti Hai?
Harrison's ke anusar:
"Systemic therapy is usually reserved for immunosuppressed patients or individuals with chronic or recurrent disease who fail to respond to appropriate topical therapy."
Matlab - oral tab lein jab:
- Topical cream 2-4 hafte lagane ke baad bhi fayda na ho
- Infection bahut zyada failah ho
- Baar baar ho raha ho (recurrent infection)
- Diabetes ya kamzor immunity ho
Dawa 1: Fluconazole (Forcan / Zocon / Fluka)
Sabse common aur safe oral antifungal
| Condition | Dose | Duration |
|---|---|---|
| Genital/Skin Candidiasis | 150 mg - ek baar | Aksar ek tablet kaafi |
| Zyada badha hua infection | 150 mg - hafte mein ek baar | 2-4 hafte |
| Tinea Cruris (saath mein) | 50-100 mg daily ya 150 mg hafte mein | 2-4 hafte |
| Baar baar aane par (recurrence) | 150 mg hafte mein ek baar | Doctor ke anusar |
(Dermatology 5e, Table 127.17)
Kaise lein:
- Khane ke saath ya bina khane ke - koi farq nahin
- Pani ke saath nigle
- Alcohol avoid karein jab le rahe hon
Dawa 2: Itraconazole (Canditral / Sporanox)
Jab fluconazole se fayda na ho ya doctor suggest karein
| Condition | Dose | Duration |
|---|---|---|
| Skin fungal infection | 100 mg din mein 2 baar | 7-14 din |
| Severe / widespread | 200 mg daily | 2-4 hafte |
Itraconazole lene ka sahi tarika:
- Khane ke SAATH lena zaroori hai - khali pet absorption bahut kam hoti hai
- Fatty meal ke saath lena sabse better hai
Side Effects - Kya Dhyan Rakhein
| Side Effect | Fluconazole | Itraconazole |
|---|---|---|
| Nausea / Pet dard | Kabhi kabhi | Kabhi kabhi |
| Headache | Kabhi kabhi | Rare |
| Liver pe asar | Rare (lekin serious) | Rare |
| Rash / Allergic reaction | Rare | Rare |
Turant doctor ko batao agar:
- Peeli aankhein ya skin (jaundice)
- Bahut zyada pet dard / ulti
- Dawa lene ke baad rash ya saans lene mein takleef
Drug Interactions - Yeh Dawaiyan Saath Mat Lein
Goodman & Gilman's ke anusaar Fluconazole ke saath avoid karein:
- Antacids / Omeprazole - kuch effect ho sakta hai
- Rifampicin (TB ki dawa) - fluconazole ka asar kam ho jaata hai
- Blood thinners (warfarin) - bleeding risk badh jaata hai
- Some heart medicines
Doctor ko zaroor batao agar koi aur dawa chal rahi hai.
Complete Treatment Protocol (Doctor Supervision mein)
STEP 1 - Topical (Pehle 2 hafte):
• Candid Cream (Clotrimazole 1%) - 2x din
• Candid Powder - nami control ke liye
STEP 2 - Agar improvement nahin:
• Fluconazole 150 mg - hafte mein ek baar x 2-4 hafte
• Topical cream jaari rakhein saath mein
STEP 3 - Baar baar ho raha hai:
• Blood sugar test (diabetes rule out)
• Doctor se recurrence prevention plan lein
• Lifestyle changes (prev. tips follow karein)
India mein Available Brands
| Generic | Brand Name | Price approx |
|---|---|---|
| Fluconazole 150mg | Forcan-150, Zocon-150, Fluka-150 | Rs. 30-60 per tablet |
| Itraconazole 100mg | Canditral, Itaspor, Itrasys | Rs. 50-80 per capsule |
| Clotrimazole cream | Candid cream, Canesten | Rs. 40-80 per tube |
⚠️ Yaad rakhein: Fluconazole 150mg akele ek baar se halke genital Candida mein fayda hota hai, lekin aapke case mein nodules aur chronic changes bhi hain - iska matlab doctor se physical examination aur diagnosis confirm karana ZAROORI hai. Self-treatment se kuch conditions (jaise Hidradenitis ya STI) miss ho sakti hain.
Kya mujhe herpes ya other STI test karwana chahiye? Abhi tak pateint virgin hai
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Bahut important information mil gayi. Ab complete, honest jawab:
STI Test Zaroor Hai? - Virgin Patient ke Liye
Short Answer: Aapke case mein STI (jaise Herpes, Syphilis, Gonorrhea) ka risk bahut kam hai - kyunki sexual contact nahin hua.
Lekin poori picture samajhna zaroori hai:
STI vs Non-STI - Kaise Sochen
STIs ke liye Sexual Contact Zaroori Hota Hai
| STI | Transmission |
|---|---|
| Herpes (HSV-2) | Sexual contact se - genital |
| Syphilis | Sexual contact se |
| Gonorrhea / Chlamydia | Sexual contact se |
| HPV (warts) | Sexual contact se mainly |
| HIV | Blood / sexual contact |
Virgin patient mein yeh sabhi STIs practically not possible hain - jab tak blood transfusion, needle sharing ya koi aur route na ho.
⚠️ Ek exception: Herpes HSV-1 (jo usually muh par hota hai) - yeh kabhi kabhi haath se genital area tak bhi ja sakta hai (auto-inoculation) - lekin yeh bahut rare hai aur presentation alag hoti hai (clear blisters).
Toh Aapke Case mein Kya Hai?
Images aur symptoms (daane, nami, itching, burning, nodules, scarring) dekhkar non-STI conditions zyada likely hain:
1. Candida Intertrigo (Fungal - Most Likely)
- Sexual contact ki zaroorat NAHIN
- Nami, garm environment, diabetes, antibiotics se hota hai
- Virgin mein bhi completely possible
2. Hidradenitis Suppurativa (HS) - Pehli Image ke Nodules ke Liye
Goldman-Cecil Medicine ke anusar:
"Hidradenitis suppurativa is a chronic and recurrent inflammatory disease characterized by painful, deep-seated nodules and abscesses that result from occlusion of the follicular infundibula followed by inflammation. Cigarette smoking and obesity are risk factors."
HS ka sexual contact se koi lena dena nahin - yeh hair follicles ke band hone se hoti hai. Genital, groin, axilla (kaankhon) mein hoti hai. Aapki pehli image ke nodules aur linear tracts bilkul HS jaisi dikhti hain.
3. Folliculitis / Infected Ingrown Hairs
- Shaving ya friction se hota hai
- Sexual contact ki zaroorat nahin
Recommended Tests - Kya Karawaein
| Test | Zaroor? | Kyun |
|---|---|---|
| KOH Scraping (Fungal test) | ✅ Haan | Candida confirm karne ke liye |
| Blood Sugar (Fasting glucose) | ✅ Haan | Candida baar baar ho raha hai toh diabetes check |
| Skin Biopsy (agar doctor suggest karein) | Consider karein | HS confirm karne ke liye |
| STI panel (Herpes, Syphilis, HIV) | ❌ Virgin mein generally nahin | Sexual contact nahin toh risk nahin |
Kab STI Test Karwana Ho Sakta Hai
Sirf tab agar:
- Sexual contact hua ho (even once, even non-penetrative)
- Blood transfusion ya injection ka history ho
- Partner ne test karaane ko kaha ho
Final Summary
Aapke patient ke liye sabse likely diagnosis:
- Candida Intertrigo - scrotum par nami, erosion, burning (sexual contact se nahin)
- Hidradenitis Suppurativa - penis par chronic nodules, scarring, sinus tracts (sexual contact se nahin - hair follicle disease hai)
Action plan:
- Dermatologist se milein
- KOH test + blood sugar test karawaein
- STI testing is case mein zaroor nahin - lekin doctor decide karenge
- Candid Cream treatment shuru kar sakte hain jaate jaate
Doctor ko bata dein ki patient virgin hai - isse doctor proper differential diagnosis karega aur unnecessary tests order nahin karega.
Hidradenitis Suppurativa ka diagnosis aur treatment details
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Fitzpatrick's aur Andrews' Diseases of the Skin se complete HS information mil gayi. Ab detailed answer:
Hidradenitis Suppurativa (HS) - Complete Guide
(Source: Fitzpatrick's Dermatology Vol 1-2, Andrews' Diseases of the Skin, Goldman-Cecil Medicine)
HS Kya Hai?
Goldman-Cecil ke anusar:
"Hidradenitis suppurativa is a chronic and recurrent inflammatory disease characterized by painful, deep-seated nodules and abscesses that result from occlusion of the follicular infundibula (hair follicle ka band hona) followed by inflammation."
Yeh STI nahin hai. Yeh ek inflammatory/immune disease hai jisme hair follicles band ho jaate hain aur neeche inflammation aur infection hoti hai.
HS ki Clinical Image (Groin Area)

Fig 13.20 - Andrews' Diseases of the Skin: Hidradenitis of the groin. Sinus tracts, discharge, chronic scarring visible.
Diagnosis Kaise Hota Hai?
HS ka koi specific lab test nahin hai - yeh clinical diagnosis hai (dekhkar aur history se):
Hurley Staging System (Severity ke 3 Stages)
| Stage | Kya Hota Hai | Aapke Case mein? |
|---|---|---|
| Stage I (Mild) | Ek ya do isolated nodules/abscess, koi sinus tract nahin, koi scarring nahin | - |
| Stage II (Moderate) | Recurrent nodules/abscesses, sinus tracts (tunnels), scarring, multiple lesions | Likely Stage II |
| Stage III (Severe) | Diffuse, widespread involvement, multiple sinus tracts, extensive scarring | - |
Aapki image (penis/groin area) mein jo nodules, linear tracts aur chronic changes hain - woh Hurley Stage II jaisi dikhti hain.
Diagnosis ke Criteria:
- Location: Axilla (kaankh), groin, perineum, genital area, under breasts
- History: Baar baar hona (recurrence), heal hona aur wapas aana
- Appearance: Nodules jo pus discharge karein, sinus tracts (tunnels under skin), scarring
- Biopsy (agar doubt ho): Follicular occlusion, lymphocytic inflammation dikhti hai
Differential Diagnosis (Inhe rule out karna padta hai):
Andrews' ke anusar: Furuncles, Bartholin abscess, scrofuloderma, actinomycosis, granuloma inguinale, lymphogranuloma venereum
Treatment - Stage-Wise
HS Treatment Algorithm (Fitzpatrick's Dermatology - European Guidelines)
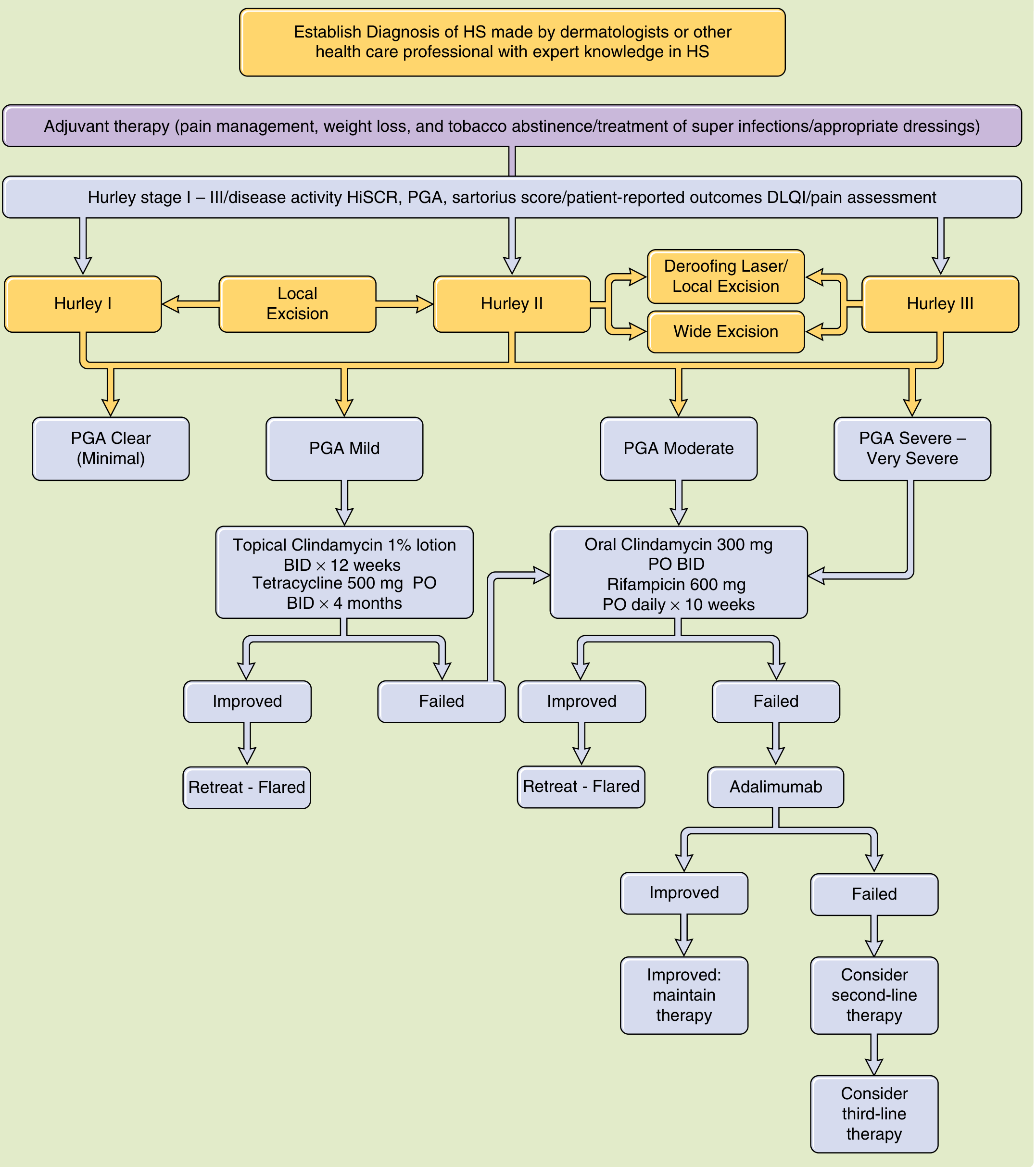
Figure 84-11 - Fitzpatrick's Dermatology: Proposed algorithm for management of HS based on disease severity
Step 1 - Lifestyle Changes (Har Stage mein)
Andrews' ke anusar:
"Daily cleansing with chlorhexidine gluconate (Hibiclens) solution or benzoyl peroxide wash is important. Reduction of friction by wearing loose-fitting clothing and weight loss, avoidance of excessive sweating, smoking cessation, and heat avoidance."
| Kya Karein |
|---|
| Chlorhexidine wash (Savlon-type) se roz dhoyein |
| Dhile cotton kapde, loose underwear |
| Wajan kam karein (obesity risk factor hai) |
| Smoking band karein |
| Garmi/paseena avoid karein |
Step 2 - Medical Treatment (Stage ke Hisaab se)
Hurley Stage I (Mild) - Topical Treatment
| Dawa | Dose | Duration |
|---|---|---|
| Clindamycin 1% lotion/gel (Clindac A) | 2x din, affected area par | 12 hafte |
| Topical Metronidazole 0.75% | Alternative | 12 hafte |
| Intralesional Triamcinolone (injection) | Doctor se, nodule ke andar | Acute flares mein |
Hurley Stage II (Moderate) - Oral Antibiotics
| Dawa | Dose | Duration |
|---|---|---|
| Tetracycline / Doxycycline | 500 mg 2x din | 4 mahine |
| Clindamycin 300 mg + Rifampicin 300 mg | Dono 2-3x din | 10 hafte |
| Triple therapy (severe): Rifampicin + Moxifloxacin + Metronidazole | Doctor ke anusar | Resistant cases mein |
Fitzpatrick's ke anusar: "A regimen of 300 mg of clindamycin and 300 mg of rifampin taken 2 to 3 times daily may be effective for Hurley stage II disease."
Hurley Stage III (Severe) - Biologic Therapy
| Dawa | Dose |
|---|---|
| Adalimumab (Humira) - FDA approved | 40 mg weekly subcutaneous injection |
| Infliximab | 5 mg/kg at weeks 0, 2, 6 then every 8 weeks |
Step 3 - Surgical Treatment
Andrews' ke anusar:
"Wide surgical excision, using intraoperative color marking of sinus tracts, is most effective at limiting recurrence and has been shown to improve quality of life."
| Surgery | Kab |
|---|---|
| Deroofing (sinus tracts khol dena) | Moderate HS mein |
| Wide excision (poori area nikalna) | Severe/chronic HS mein |
| CO2 Laser / Nd:YAG Laser | Evidence-based option - effective |
| I&D (incision & drainage) | Strongly discouraged - wapas aata hai |
Treatment Evidence Table (Fitzpatrick's Guidelines)
| Therapy | Evidence Level | Recommendation |
|---|---|---|
| Topical Clindamycin | IIb | B |
| Oral Clindamycin + Rifampicin | III | C |
| Adalimumab | I | A (Strongest) |
| Tetracycline oral | IIb | B |
| CO2 / Nd:YAG Laser | Ib | A |
| Wide excision | IIb | B |
| Isotretinoin | IV | D (weak) |
Aapke Patient ke Liye Next Step
- Dermatologist se milein - HS staging confirm karne ke liye
- Chlorhexidine wash shuru karein abhi se
- Candid Cream jaari rakhein - Candida jo saath mein hai uske liye
- Doctor se topical Clindamycin prescription lein
- Agar Stage II confirm ho - oral doxycycline + clindamycin combination doctor ke prescription se
- I&D (drain karne ki surgery) mat karaein - HS mein wapas aata hai aur scar barhta hai
⚠️ HS ek chronic disease hai jo cure nahin hoti lekin properly managed ho sakti hai. Dermatologist ke regular follow-up se quality of life bahut improve hoti hai.
This is a shared conversation. Sign in to Orris to start your own chat.