Treatment for thyroiditis
Reading File
Finding Sources
Searching PubMed
thyroiditis management treatment
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information on all major types of thyroiditis. Let me compile the full answer.
Treatment of Thyroiditis
Thyroiditis is not a single disease but a group of inflammatory thyroid disorders. Treatment depends entirely on the type. Here is a systematic breakdown:
1. Subacute (de Quervain's / Granulomatous) Thyroiditis
This is the most common cause of a painful thyroid, typically following a viral URI, often with fever, jaw/ear-referred pain, and markedly elevated ESR.
Thyrotoxic phase:
- NSAIDs or aspirin (e.g., aspirin 600 mg every 4-6 h) are first-line for mild-to-moderate pain. Add gastroprotective cover (PPI).
- Glucocorticoids (prednisone 15-40 mg/day, Goldman-Cecil uses 40-60 mg/day) if symptoms are severe or NSAIDs inadequate. Taper slowly over 6-8 weeks, guided by symptom improvement and falling ESR. Rapid taper risks relapse.
- Beta-blockers (e.g., atenolol 25-50 mg/day) for symptomatic thyrotoxicosis (palpitations, tachycardia). Antithyroid drugs (PTU, methimazole) have no role - hormone synthesis is not increased, only release.
Hypothyroid phase:
- If prolonged or symptomatic: levothyroxine (LT4) 50-100 µg/day (low dose to allow TSH-mediated recovery). Most patients recover spontaneously within 6-9 months.
- Permanent hypothyroidism occurs in ~15% (more common with coincident thyroid autoimmunity).
2. Silent (Painless) / Postpartum Thyroiditis
An autoimmune process with a clinical course similar to subacute thyroiditis but without pain and with a normal ESR. Postpartum variant occurs within 12 months of delivery in ~5-10% of women; strongly associated with TPO antibodies antepartum.
Thyrotoxic phase:
- Usually mild and self-limited. Glucocorticoids are NOT indicated.
- If severe: short course of propranolol 20-40 mg TID/QID (or atenolol 25-50 mg/day).
- Antithyroid drugs again play no role.
Hypothyroid phase:
- Levothyroxine if symptomatic or severe. Taper after 6-9 months to assess recovery.
- If pregnant or attempting conception: continue LT4 throughout pregnancy without tapering.
Prognosis: Up to 50% develop permanent hypothyroidism (more likely with high TPO Ab titers). Postpartum thyroiditis recurs after ~70% of subsequent pregnancies.
3. Drug-Induced Thyroiditis
Caused by IFN-alpha, tyrosine kinase inhibitors (sorafenib), immune checkpoint inhibitors (pembrolizumab, nivolumab - in 5-20% of patients), and amiodarone.
- Treatment is the same as for silent thyroiditis - beta-blockers for symptomatic thyrotoxicosis, LT4 for prolonged hypothyroid phase.
- Routine monitoring of thyroid function tests is recommended throughout treatment.
4. Infectious (Acute/Suppurative) Thyroiditis
Rare, caused mainly by Staphylococcus aureus and Streptococcus pyogenes (adults), anaerobes (children), or fungi (immunocompromised patients).
- Antibiotics guided initially by Gram stain, then by FNA culture results.
- Surgical drainage if an abscess has formed (localize by CT or ultrasound).
- Thyroid function is usually normal; monitor for rare thyrotoxicosis or hypothyroidism.
- Complications (septicemia, mediastinitis, tracheal obstruction) are prevented by prompt antibiotic use.
5. Hashimoto's (Chronic Autoimmune) Thyroiditis
Most common cause of hypothyroidism. Autoimmune lymphocytic infiltration, TPO antibodies positive.
- If hypothyroid: Levothyroxine replacement is the cornerstone. Target TSH within normal range (typical adult dose ~1.6 µg/kg/day, individualized). In subclinical hypothyroidism (TSH <10 mIU/L), treat if TPO Abs positive, symptoms present, or atherosclerotic vascular disease is present.
- If euthyroid: Monitor periodically; no treatment required.
- Thyroid replacement therapy increases cortisol clearance - always check ACTH status before starting LT4 in secondary hypothyroidism to avoid precipitating adrenal crisis.
6. Riedel's Thyroiditis
Rare, fibrosclerosing disorder in middle-aged women causing a "stony hard" goiter with compressive symptoms; associated with IgG4-related disease.
- Glucocorticoids - first-line for initial management.
- Tamoxifen - used as second-line therapy, with demonstrated efficacy.
- Surgery may be needed to relieve tracheal or esophageal compression (isthmusectomy).
Quick Reference Summary
| Type | Key Treatment |
|---|---|
| Subacute (de Quervain's) | NSAIDs/aspirin → prednisone; beta-blocker for thyrotoxicosis; LT4 if hypothyroid phase prolonged |
| Silent/Postpartum | Beta-blocker (thyrotoxic); LT4 (hypothyroid); no glucocorticoids |
| Drug-induced | Same as silent thyroiditis |
| Infectious/Suppurative | Antibiotics ± surgical drainage |
| Hashimoto's | LT4 if hypothyroid; monitor if euthyroid |
| Riedel's | Glucocorticoids; tamoxifen; surgery if compressive |
Key principle across all types: Antithyroid drugs (methimazole/PTU) are never indicated in thyroiditis-related thyrotoxicosis because the excess hormone comes from gland destruction/leakage, not from overproduction.
Sources: Harrison's Principles of Internal Medicine 22E, 2025 (McGraw Hill); Goldman-Cecil Medicine, International Edition; Textbook of Family Medicine 9e
Post partum thyroiditis
Finding Sources
Searching PubMed
postpartum thyroiditis
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive, authoritative content from multiple textbooks plus the clinical diagram. Here is the full answer.
Postpartum Thyroiditis (PPT)
Definition
Postpartum thyroiditis is a transient autoimmune destructive thyroiditis occurring within the first 12 months after delivery or pregnancy loss in patients who were euthyroid before conception. It is considered a variant of Hashimoto's thyroiditis triggered by the postpartum immune rebound.
Epidemiology & Risk Factors
- Occurs in 4-8% of postpartum women (some studies report up to 22% depending on screening methods and population)
- Among TPO antibody-positive women identified in the first trimester, 33-50% will develop PPT
- Higher risk in women with 60-70% TPO Ab positivity vs. <1% without TPO Abs
- Type 1 diabetes mellitus - PPT occurs in ~25%
- History of prior PPT - ~70% recurrence rate in subsequent pregnancies
- Associated HLA haplotypes: HLA-DR3, DR4, DR5
- Also increased in women with Graves disease, SLE, chronic viral hepatitis
Pathophysiology
The postpartum period involves a rebound of cellular and humoral immunity suppressed during pregnancy:
- Phase 1 (1-4 months postpartum): Cytotoxic T cells and NK cells rise, exacerbating tissue injury in the thyroid (Hashimoto-like), causing the thyrotoxic phase
- Phase 2 (4-10 months postpartum): CD5+ B cells rise, can cause Graves disease relapse separately
The thyroid injury causes proteolysis of thyroglobulin stores and release of preformed T4 and T3 - this is destruction-induced thyrotoxicosis, not overproduction.
Clinical Phases
The classic triphasic pattern occurs in only ~25% of patients:
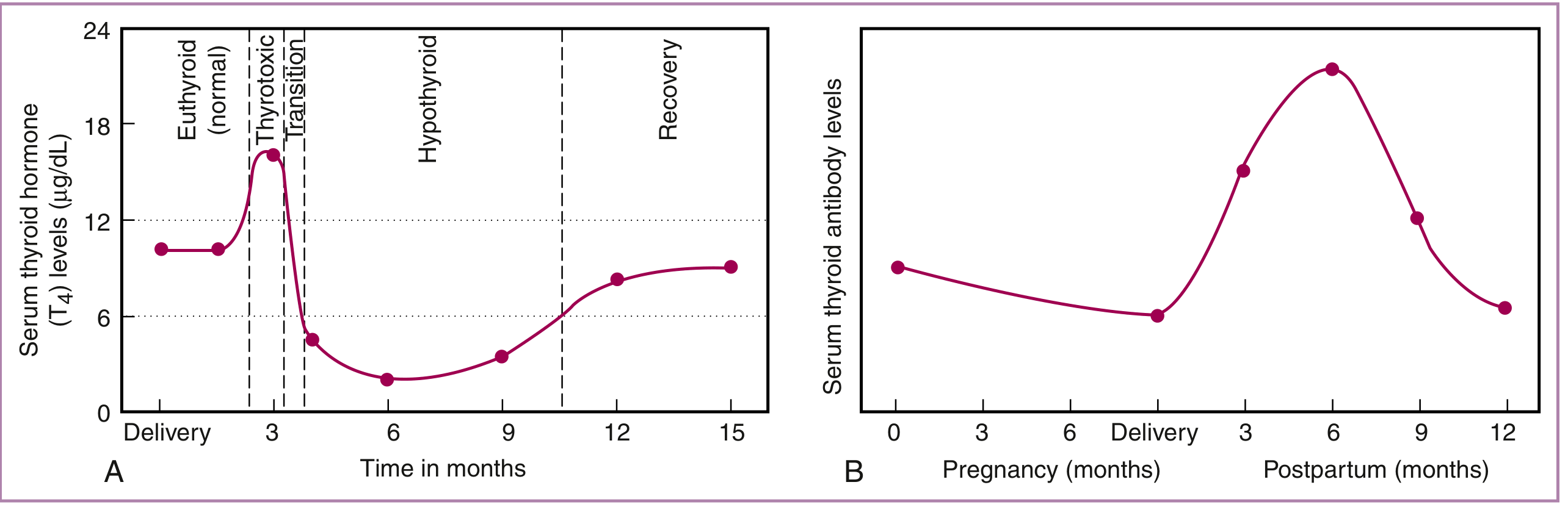
Figure: (A) Classic biphasic course - thyrotoxic phase peaks ~3 months, hypothyroid phase through 6-9 months, with recovery. (B) Thyroid antibody levels surge 3-6 months postpartum then decline. (Creasy & Resnik's Maternal-Fetal Medicine)
| Phase | Timing | Frequency |
|---|---|---|
| Thyrotoxic only | 6 weeks - 4 months (median 13 weeks) | ~25% |
| Hypothyroid only | Median onset 19 weeks; lasts up to 1 year | ~50% |
| Both (triphasic) | Classic full course | ~25% |
Clinical Features
Thyrotoxic phase (milder than Graves'):
- Fatigue, insomnia, nervousness, palpitations, heat intolerance, anxiety, weight loss, irritability
- Painless goiter (nontender), no exophthalmos, no bruit
- TSH low/undetectable; free T4 elevated; T4:T3 ratio >20:1 (reflects stored hormone release)
- TPO antibodies positive; TRAb negative (key distinction from Graves)
- Radioactive iodine uptake: low to undetectable
Hypothyroid phase:
- Fatigue, weight regain, depression, impaired concentration, paresthesia, dry skin
- Symptoms often missed as they overlap with normal postpartum complaints
- TSH may still be suppressed from the prior thyrotoxic phase - check FT4 as well
- TSH elevated when the hypothyroid phase is established
Differentiating PPT from Graves Disease
| Feature | PPT | Graves |
|---|---|---|
| Timing | 1-4 months postpartum | 4-12 months postpartum |
| Thyrotoxicosis severity | Mild | More severe |
| Duration of toxic phase | <2 months | Prolonged |
| T4:T3 ratio | High (>20:1) | Low (<20) |
| TRAb/TSI antibodies | Negative | Positive |
| TPO antibodies | Positive | Usually negative (unless mixed) |
| Goiter | Small, nontender | May be diffuse |
| Exophthalmos/bruit | Absent | May be present |
| RAIU | Low | High |
| Thyroid ultrasound | Hypoechoic, low Doppler flow | Increased vascularity |
Thyroid scintigraphy (¹²³I or Tc-99m pertechnetate) is rarely needed given the above distinctions. If performed while breastfeeding: pump and discard milk for 2-3 days after ¹²³I, 24 hours after Tc-99m.
Treatment
Thyrotoxic Phase
- Usually mild and self-limiting - no specific treatment often needed
- Beta-blockers (propranolol 20-40 mg TID/QID, or metoprolol) for symptomatic palpitations, tachycardia, or tremor
- Antithyroid drugs (PTU, methimazole) are CONTRAINDICATED - the excess hormone is from destruction/release, not overproduction; ATDs will have no effect
- Glucocorticoids are NOT indicated (unlike subacute thyroiditis)
- Follow TFTs every 4-8 weeks to monitor for transition to hypothyroid phase
Hypothyroid Phase
Treat if any of the following:
- TSH ≥10 mIU/L with symptoms
- Overt hypothyroidism (low FT4)
- Patient is lactating
- Patient is attempting future conception or pregnant
Levothyroxine (LT4):
- Full replacement dose (1.6 µg/kg/day) usually not needed; start low: 50-75 µg/day
- If not actively trying to conceive, taper at 12 months postpartum to assess whether hypothyroidism has resolved
- If pregnant or attempting conception: continue LT4 without tapering throughout pregnancy
- TSH/FT4 recheck every 4-8 weeks until stable
Prognosis & Long-term Follow-up
- 50-80% recover to euthyroidism by 1 year
- 20-70% ultimately develop permanent hypothyroidism (wide range due to study differences)
- Risk factors for permanent hypothyroidism:
- Higher TPO antibody titers
- Greater severity of initial hypothyroidism
- Multiparity, older age
- Thyroid hypoechogenicity on ultrasound
Monitoring:
- Annual TSH in all women with a history of PPT (even if recovered)
- Women who are TPO antibody-positive: check TSH at 6-12 weeks gestation AND again at 6 months postpartum in future pregnancies
- Recurrence risk in subsequent pregnancies: ~70-80%
PPT and Postpartum Depression
- A statistically significant association exists (incidence rate ratio ~1.99 for first-onset psychiatric disorders in PPT vs. non-PPT)
- However, a prospective RCT of LT4 in TPO-positive women found no reduction in postpartum depression rates
- Causality is uncertain, but hypothyroidism is a partially treatable contributor to mood symptoms
- The ATA and Endocrine Society recommend screening for thyroid dysfunction in all patients with depression
Screening & Prevention
- Universal screening of all postpartum women is NOT recommended (insufficient evidence)
- Screen high-risk groups:
- History of prior PPT
- Known TPO antibody positivity
- Type 1 diabetes
- Personal or first-degree family history of autoimmune disease
- New postpartum depression or anxiety
- Prevention: Selenium supplementation, LT4, and iodine have NOT been shown to reliably prevent PPT and are not recommended
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Tietz Textbook of Laboratory Medicine 7e; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine
Post partum thyroiditis
I just covered postpartum thyroiditis in detail in my previous response! Here's a quick summary of the key points:
Definition: Transient autoimmune destructive thyroiditis within 12 months of delivery, a variant of Hashimoto's triggered by postpartum immune rebound.
Phases:
- Thyrotoxic (1-4 months) - 25% of patients
- Hypothyroid (median onset 19 weeks) - 50% of patients
- Both/triphasic - 25% of patients
Treatment:
- Thyrotoxic phase: Beta-blockers if symptomatic; NO antithyroid drugs, NO glucocorticoids
- Hypothyroid phase: Levothyroxine 50-75 µg/day if TSH ≥10, symptomatic, lactating, or trying to conceive; taper at 12 months to check for recovery
Key facts:
- Incidence: 4-8% of postpartum women
- TPO antibodies positive in ~85%
- Recurs in ~70% of subsequent pregnancies
- 20-70% develop permanent hypothyroidism
- Annual TSH monitoring recommended long-term
Would you like me to go deeper into any specific aspect - such as the pathophysiology, differentiation from Graves disease, management in pregnancy, or screening guidelines?

IMG_2738.png
Interpretation of this report
Here is the interpretation of Deepika Sharma's thyroid panel:
Patient Details
- Name: Deepika Sharma | Age: 31 years, Female
- Sample drawn: 21/05/2026
- Lab: Agilus Diagnostics (formerly SRL), Indore
Results at a Glance
| Test | Current Result | Reference (Non-Pregnant) | Status |
|---|---|---|---|
| T3 | 310.90 ng/dL | 80.0 - 200.0 | 🔴 HIGH |
| T4 | 14.55 µg/dL | 5.10 - 14.10 | 🔴 HIGH |
| TSH (Ultrasensitive) | 0.005 µIU/mL | 0.27 - 4.20 | 🔴 VERY LOW |
Trend Analysis (Serial Reports)
| Test | Current (21/05/26) | Previous 1 (22/02/26) | Previous 2 (17/09/25) | Previous 3 (08/07/25) |
|---|---|---|---|---|
| T3 | 310.90 ↑ | 331.20 ↑ | 130.70 (normal) | 235.50 ↑ |
| T4 | 14.55 ↑ | 17.06 ↑ | 10.16 (normal) | 11.74 (normal) |
| TSH | 0.005 ↓↓ | <0.005 ↓↓ | 1.150 (normal) | 3.740 (normal) |
Interpretation
Pattern: Overt Thyrotoxicosis (suppressed TSH + elevated T3 and T4)
The triad of very low TSH + elevated T3 + elevated T4 confirms active thyrotoxicosis. The TSH has been essentially undetectable (<0.005) for at least 3 months (since February 2026), with T3 and T4 persistently elevated.
Key clinical context to consider:
1. Is this Graves' disease or Postpartum Thyroiditis?
Given that this patient:
- Is a 31-year-old woman
- Has had our prior discussion about postpartum thyroiditis
- Shows a pattern of thyroid dysfunction evolving since mid-2025
The timeline is very suggestive of postpartum thyroiditis - the thyroid values were normal in July 2025, became elevated by September 2025, and have remained in a thyrotoxic state since. This is consistent with the thyrotoxic phase of PPT persisting or recurring.
However, Graves' disease cannot be excluded without:
- TRAb / TSI antibodies (thyroid-stimulating immunoglobulin) - if positive, confirms Graves'
- TPO antibodies - if positive, supports Hashimoto's/PPT
- Thyroid ultrasound with Doppler - low flow favors PPT; high flow favors Graves'
- RAIU scan - low uptake = PPT; high uptake = Graves' (rarely needed)
2. Why the distinction matters critically:
- PPT thyrotoxicosis: treat only with beta-blockers; antithyroid drugs are contraindicated
- Graves' thyrotoxicosis: requires antithyroid drugs (carbimazole/PTU)
Recommended Next Steps
- TRAb (TSH receptor antibody) - most important single test to distinguish Graves' vs PPT
- TPO antibodies - supports autoimmune thyroiditis
- Thyroid ultrasound with color Doppler - assess vascularity
- Clinical history - date of last delivery, breastfeeding status, current symptoms (palpitations, weight loss, heat intolerance, tremor)
Immediate Clinical Concerns
- TSH of 0.005 for 3+ months is associated with risks of:
- Atrial fibrillation
- Bone loss (osteoporosis with prolonged exposure)
- Cardiovascular strain
- This patient needs urgent endocrinology review, not self-referral (report shows "REF. DOCTOR: SELF")
- If symptomatic (palpitations, tremor, tachycardia): beta-blocker (propranolol 20-40 mg TID) is appropriate while awaiting further workup
⚠️ This report requires urgent clinical evaluation by an endocrinologist. The prolonged suppressed TSH over 3 months with elevated T3/T4 is not a self-resolving pattern and needs definitive diagnosis and treatment.
This is a shared conversation. Sign in to Orris to start your own chat.